ORIGINAL ARTICLE
Rheumatic Diseases in Chihuahua, México
A COPCORD Survey
Danyella Del Río Nájera, MD,* Susana Aideé González-Chávez, MSc,* Celia María Quiñonez-Flores, MSc,*
Ingris Peláez-Ballestas, MD, PhD,† Norma Hernández-Nájera, HM,‡ and César F. Pacheco-Tena, MD, PhD*
Background: Rheumatic diseases (RDs) represent a global problem for
health care systems and patients. Community Oriented Program for Control of Rheumatic Diseases (COPCORD) is a low-cost screening tool for
detecting musculoskeletal (MSK) pain and RDs.
Objective: The aim of this study was to examine the pattern of MSK pain
and RDs in clinic population in Chihuahua City, Mexico.
Methods: A cross-sectional study was conducted in 7 primary health
clinics using the COPCORD methodology in subjects older than 18 years.
People with MSK pain not induced by trauma (positive cases) were evaluated by primary care physicians and rheumatologists.
Results: The study included 1006 individuals with a mean age of 46.0
(SD, 15.8)years; 751 (74.7%) were women. Musculoskeletal pain in the
previous 7 days was reported by 571 individuals (56.75%; 95% confidence interval [CI], 53.8%–60.1%), and 356 cases (35.4%; 95% CI,
32.5%–38.4%) were COPCORD positive. The mean pain intensity in
visual analog scale was 6.62 (SD, 2.4). The most common painful joint
was the knee (54.7%; 95% CI, 51.1%–59.0%). Two hundred eighty subjects with MSK pain (49.0%) previously sought medical attention, and
375 (65.7%) were under treatment. Functional impairment was reported
by 69.8% of the COPCORD-positive subjects. The prevalence of RDs
was 21.4% (95% CI, 18.9%–23.8%). The most prevalent disease was osteoarthritis (10.3%; 95% CI, 8.6%–12.4%), followed by regional pain syndromes (5.5%; 95% CI, 4.1%–7.0%), rheumatoid arthritis (1.4%; 95% CI,
0.8%–2.2%), and mechanical low-back pain (1.4%; 95% CI, 0.7%–2.2%).
Conclusions: Musculoskeletal pain is an important problem that affects our community. The data provided in this study will be presented
to the local authorities to help in the development of prevention strategies.
Key Words: disability, musculoskeletal, osteoarthritis, pain, rheumatic
(J Clin Rheumatol 2016;00: 00–00)
R
heumatic diseases (RDs) represent a burden to the societies
worldwide. They constitute a group of clinical conditions that
affect the musculoskeletal (MSK) system.1,2 Their principal symptoms are pain, stiffness, and swelling. These symptoms and their
consequent complications significantly reduce the life expectancy and quality of life of the affected.3
Rheumatic diseases entail a high cost for both health care system and patients. Their costs depend on the severity and type of
the disease.4–6 Epidemiology data for specific populations could
help in the design of prevention strategies to reduce costs and
achieve optimized health coverage.7
From the *Facultad de Medicina, Universidad Autónoma de Chihuahua,
Chihuahua; †Rheumatology Department, General Hospital of México
“Eduardo Liceaga,” Mexico City; and ‡Facultad de Ciencias de la Cultura
Física, Universidad Autónoma de Chihuahua, Chihuahua, Mexico.
The authors declare no conflict of interest.
Correspondence: César F. Pacheco-Tena, MD, PhD, Facultad de Medicina,
Universidad Autónoma de Chihuahua, Circuito No. 1, Nuevo Campus
Universitario, Chihuahua, Chihuahua, México C.P. 31240.
E-mail: dr.cesarpacheco@gmail.com.
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved.
ISSN: 1076-1608
DOI: 10.1097/RHU.0000000000000380
The Community Oriented Program for Control of Rheumatic Diseases (COPCORD) was developed by the World
Health Organization and the International League of Associations for Rheumatology. COPCORD was proposed as a screening tool for MSK pain in developing countries.2 It has 3 main
stages. The first stage is also divided in 3 phases: the evaluation
of pain (intensity, location, association to trauma, and treatment),
clinical assessment of the positive cases (pain without trauma
history), and the medical approach by a rheumatologist. Second
and third stages are about situational diagnosis and design of
prevention programs.8–10
COPCORD has been used internationally in the last 30 years,
and its accuracy has been proven with satisfactory results.2 In
Mexico, this program has been applied in the states of Nuevo
León, Yucatán, Sinaloa, Distrito Federal, and Chihuahua. The
prevalence of pain found in these studies varies between 7.1%
and 43.7%. The most prevalent specific disease per region was osteoarthritis (OA) in all cases. However, significant variations were
found in specific diagnoses.3,11–13 The Chihuahua survey was developed in Aldama City, which is a semirural community nearby
the capital city (Chihuahua). Its population at the time of the survey (2010) was 22,302 (0.65% of the state population).14 In that
COPCORD study, 13% of the interviewed reported pain in the last
7 days. Osteoarthritis was the most common RD (20.5%), but a
relatively high prevalence of rheumatoid arthritis (RA) of 1.9%
was also described. As many regional variations were seen in
the previous researches, it is important to establish the characteristics of each population.3
It has been reported that 5.5% of the Chihuahua population
has some kind of functional impairment, of which 36.4% are associated with some disease15; however, the epidemiological data of
prevalence of MSK pain and RDs have not been previously reported for Chihuahua City. Therefore, the aim of this study was
to examine MSK pain and RDs in individuals older than 18 years
who are beneficiaries of the Mexican Popular Healthcare System
in Chihuahua City.
MATERIALS AND METHODS
Participants
A cross-sectional study was performed using the Mexican
COPCORD Core Questionnaire (CCQ) from September 2014 to
April 2015. This study aimed to assess RDs in individuals older
than 18 years who are beneficiaries of the Mexican Popular
Healthcare System (Spanish: Seguro Popular), who receive medical care at community clinics of Chihuahua City. For this purpose, the Chihuahua’s Department of Health authorized the
study in 7 community clinics in Chihuahua City.
Inclusion Criteria
The subjects included in the sample were present in the
clinics’ waiting rooms and verbally agreed to answer the CCQ after an explanation of the procedure.
JCR: Journal of Clinical Rheumatology • Volume 00, Number 00, Month 2016
www.jclinrheum.com
1
�Del Río Nájera et al
JCR: Journal of Clinical Rheumatology • Volume 00, Number 00, Month 2016
Sampling Design
The sample size was calculated using the formula for finite
population. Chihuahua City had 819,543 inhabitants in 2010
(24.05% of the state’s total population).16 In Chihuahua, 87,342
families belong to the Popular Healthcare System. The confidence
level was calculated at 95% with a margin of 5% and a probability
level of 0.5. The estimated value was 385; still the size was amplified to 1000 in order to have a more representative sample.
Screening Tool
The CCQ was previously adapted and validated in Mexican
population by Goycochea-Robles et al17 to detect MSK pain.
Interview
Phase 1: CCQ Application
Medicine students and health care–related personnel were recruited for the survey application. There were a total of 10 interviewers previously trained for the application of CCQ. They
applied the CCQ in the clinic’s waiting room of the community
clinics at Chihuahua City.
Phase 2: Clinical Evaluation by Primary
Care Physicians
The CCQ was considered positive when individuals reported
nontraumatic MSK pain of greater than 1 on a visual analog scale
(VAS) during the last 7 days.3,17 A physician examined all CCQpositive individuals at the moment of the identification. When this
was not possible, the patients were scheduled later. The medical
assessment consisted of a medical history. The results of this
phase allowed the physician to classify the patients in 2 main
groups: suggestive inflammatory or noninflammatory diseases.
The first group included RA, gout, spondyloarthritis, connective
tissue diseases, and undefined arthritis. The second group comprised OA, fibromyalgia, regional pain syndrome (RRPS), mechanic
low-back pain, osteoporosis, and non-RDs (vascular dysfunction
or neuropathic disease). All of the diagnoses were established
under the basis of the current accepted classification criteria.18–22
A board-certified rheumatologist clinically assessed suggestive
cases of inflammatory disease.
Phase 3: Clinical Evaluation by a Rheumatologist
To confirm the diagnosis, the rheumatologist evaluated subjects with suspected inflammatory RD. If necessary, these patients underwent laboratory and radiographic studies. They also
received medication according to their disease. The noninflammatory disease cases were sent to their family physician for follow-up
with full information of their disease and care advice.
Ethical Aspects
This study was approved by the ethical committee of the
Medicine School of the Autonomous University of Chihuahua.
The study also was approved by the Health Department (Spanish:
Secretaría de Salud) of Chihuahua’s government. This institution
authorized the survey in the selected community attention clinics.
For the CCQ application, all participants were invited to voluntarily participate in the study. A verbal consent was obtained
from subjects who agreed to answer the questionnaire. If a patient needed to be evaluated by a specialist, an informed consent was signed; confirmatory tests including blood samples or
imaging tests were used if required. The entire process, including
interviews, medical examination by a physician and rheumatologist, and laboratory or radiographic studies (when necessary),
2
www.jclinrheum.com
was conducted in health centers of the Health Department of
Chihuahua’s government.
Statistical Analysis
The statistical analysis was made in IBM SPSS Statistics for
Windows, Version 21.0 (IBM Corp, Armonk, NY). The analysis
yielded measures of central tendency and dispersion for continuous variables. In addition, absolute and relative frequencies
for ordinal, nominal, or categorical variables were used. Prevalence (%) and 95% confidence interval (CI) were calculated for
the variables of the CCQ. Prevalence was calculated dividing
the total number of patients with RD by the population surveyed.
RESULTS
The sociodemographic data of this study are shown in
Table 1. One thousand and six interviews were included. Women comprised 74.7% of the total surveyed population. The mean age was
TABLE 1. Sociodemographic Data
Variable
n = 1006; n (%)
Total population (n)
Age, mean (SD); range, y (n = 1006)
Women
Age, mean (SD); range, y (n = 751)
Men
Age, mean (SD); range, y (n = 255)
Distribution by communitarian center
CAAPS
Age, mean (SD); range, y/women,
n (%)
Cerro Prieto
Age, mean (SD); range, y/women,
n (%)
Nombre de Dios
Age, mean (SD); range, y/women,
n (%)
Revolución
Age, mean (SD); range, y/women,
n (%)
San Felipe
Age, mean (SD); range, y/women,
n (%)
San Jorge
Age, mean (SD); range, y/women,
n (%)
Tierra y Libertad
Age, mean (SD); range, y/women,
n (%)
Occupation (n = 224)a
Domestic service/housekeeping
Seller/employee
Laborer/industry
Retired/student
Construction
Farmer
Other
1006
46.0 (15.8); 18–87
751 (74.7)
45.2 (15.5); 18–87
255 (25.3)
48.3 (16.5); 18–85
479 (47.6)
44.1 (14.2); 18–79/362 (75.6)
54 (5.4)
42.2 (13.4); 18–73/47 (87.0)
20 (2.0)
53.1 (14.1); 24–78/15 (75.0)
29 (2.9)
58.7 (13.5); 29–83/22 (75.9)
321 (31.9)
48.1 (17.6); 18–87/226 (70.4)
82 (8.2)
45.5 (15.7); 19–80/66 (80.5)
21 (2.1)
44.4 (17.9); 19–81/13 (61.9)
120 (53.6)
38 (17.0)
30 (13.4)
17 (7.6)
11 (4.9)
6 (2.7)
2 (0.9)
a
The question was formulated to the COPCORD-positive cases
(n = 356), of which only 224 responded (224/356 = 0.63).
CAAPS, advanced center for primary health care.
© 2016 Wolters Kluwer Health, Inc. All rights reserved.
�JCR: Journal of Clinical Rheumatology • Volume 00, Number 00, Month 2016
TABLE 2. Characteristics of Subjects With Reports of MSK Pain
in the Last 7 Days
Variable
n = 1006, n (%; 95% CI)
MSK pain in the last 7 d
Trauma related
Non–trauma related
Pain intensity, mean (SD)
Medical attention
Treatment
NSAIDs
Acetaminophen
Supplementsa
Pain adjuvantsb
Opioids
Steroids
DMARDs
Othersc
Medical prescription
Self-medication
571/1006 (56.8; 53.8–60.1)
215/571 (37.7; 33.6–41.7)
356/571 (62.3; 58.3–66.4)
6.6 (2.4)
280/571 (49.0; 44.8–52.8)
375/571 (65.7; 61.8–69.5)
305/375 (81.3; 77.3–85.2)
81/375 (21.6; 18.1–25.5)
55/375 (14.7; 11.5–18.1)
12/375 (3.2; 1.6–5.1)
10/375 (2.7; 1.1–4.5)
5/375 (1.3; 0.3–2.4)
5/375 (1.3; 0.3–2.6)
27/375 (7.2; 4.3–10.0)
274/375 (73.1; 69.1–77.3)
101/375 (26.9; 22.7–30.9)
a
Calcium and vitamin B complex.
Gabapentin, pregabalin, muscle relaxant.
c
Allopurinol and nonspecified.
DMARDs indicates disease-modifying antirheumatic drugs.
b
COPCORD Chihuahua México
46.0 years. The most common occupation was domestic work in
53.6% of the respondents (120/224), followed by employee work
in 17.0% (38/224) and laborer in 13.4% (30/224) (Table 1).
A total of 571 patients (56.8%) reported MSK pain in the last
7 days (Table 2), and 356 cases (35.4%; 95% CI, 32.5%–38.4%)
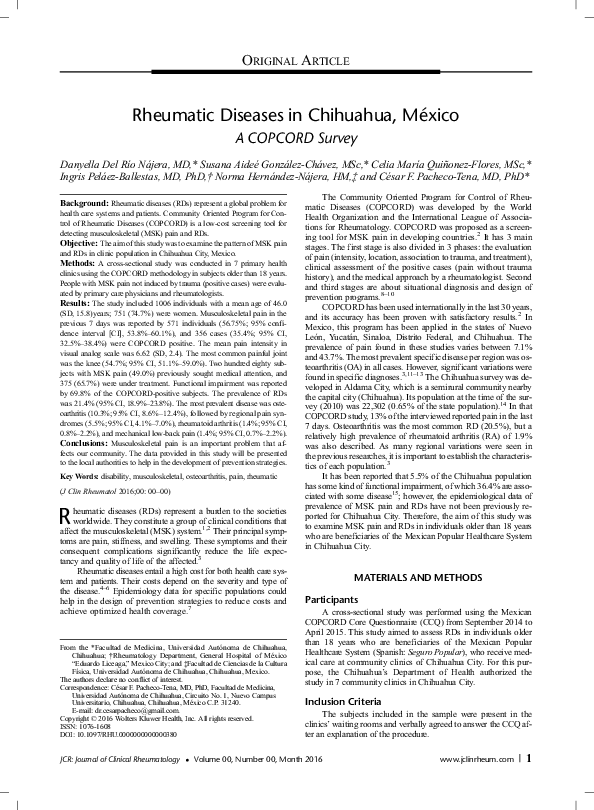
were considered COPCORD positive. The mean VAS pain intensity was 6.6 (SD, 2.4). In regard to the affected joints, the knees
were the most affected site (54.7%), followed by the hands
(29.1%) and shoulders (22.1%) (Figure). Two hundred eighty
(49.0%) of the individuals with MSK pain had sought medical
attention. The most used medication was nonsteroidal antiinflammatory drugs (NSAIDs) (81.3%). The treatment was prescribed by a physician in 274 cases (73.1%), and unfortunately,
101 individuals (26.9%) were self-prescribed (Table 2).
The characteristics of COPCORD-positive subjects are described in Table 3. The mean VAS pain intensity for these individuals was 7.0 (SD, 2.3). Sixty-nine percent of them had
allopathic treatment, whereas 24.5% used alternative medication.
Twenty-six individuals (11.8%) reported family history of rheumatic symptoms. Functional impairment was reported by 69.8%
of the COPCORD-positive subjects. Only 72.7% (259/356) of
COPCORD-positive subjects completed their medical care until
a definitive diagnosis was established; whereas the remaining
patients could not be diagnosed because of the lack of commitment to attend subsequent medical appointments or laboratory studies. It was of interest that only 67 patients (18.8%) of
the total positive COPCORD cases had an established diagnosis
prior to our investigation.
The prevalence of RDs was 21.4% (95% CI, 18.9%–23.8%).
The most prevailing group diseases were the noninflammatory diseases of which OA affected 10.3% of the total studied
FIGURE. Body regions most frequently affected by pain in the last 7 days. Prevalence rates are shown as percentage; 95% CI.
© 2016 Wolters Kluwer Health, Inc. All rights reserved.
www.jclinrheum.com
3
�JCR: Journal of Clinical Rheumatology • Volume 00, Number 00, Month 2016
Del Río Nájera et al
TABLE 3. Characteristics of COPCORD-Positive Subjects
Variable
n = 356, n (%; 95% CI)
Pain intensity, mean (SD)
Medical attention
Treatment
NSAIDs
Acetaminophen
Supplementsa
Pain adjuvantsb
Opioids
Steroids
DMARDs
Othersc
Medical prescription
Self-medication
Use of alternative treatmentd
Family history of rheumatic symptomsd
Functional impairmentd
Mild
Moderate
Severe
7.0 (2.3)
196/356 (55.1; 50.0–59.9)
249/356 (69.9; 64.9–74.5)
211/249 (84.7; 79.9–89.6)
52/249 (20.9; 14.9–25.9)
42/249 (16.9; 12.0–22.0)
9/249 (3.6; 1.6–6.3)
5/249 (2.0; 0.4–3.6)
5/249 (2.0; 0.5–4.0)
5/249 (2.0; 0.4–4.0)
15/249 (6.0; 3.2–9.1)
190/249 (76.3; 70.0–81.9)
59/249 (23.7; 18.1–30.0)
58/236 (24.5)
26/220 (11.8)
157/225 (69.8)
44/157 (28.0)
60/157(38.2)
53/157 (33.8)
a
Calcium and vitamin B complex.
Gabapentin, pregabalin, muscle relaxant.
c
Allopurinol and nonspecified.
d
The question was formulated to the COPCORD-positive cases
(n = 356), but not everyone agreed to respond.
DMARDs indicates disease-modifying antirheumatic drugs.
b
population. Although inflammatory RDs affected only 3.2%,
they were found to have a higher mean pain intensity (VAS,
7.2) and physical limitation (up to 90%) than in noninflammatory
disease patients. Rheumatoid arthritis was the most prevalent inflammatory disease, with a prevalence of 1.4% (95% CI, 0.8%–
2.2%) (Table 4).
DISCUSSION
Previous research in Mexico has shown a notable prevalence
of MSK pain, with local variations between cities.3,11,22,23 In the
state of Chihuahua, an earlier survey was made in Aldama City
population; however, Chihuahua City had not been surveyed.
Our study, unlike the vast majority of studies using the methodology COPCORD, has the peculiarity that the prevalence of
MSK pain and RDs was determined in a clinical population. This
allowed us to examine a population that had the benefit of a public
Popular Healthcare System. Surprisingly, even though our surveys
were conducted with individuals who receive medical care at community attention clinics of Chihuahua City, we found prevalence
rates of 56.8% and 21.4% of MSK pain and RDs, respectively.
Although our study is not a community survey, the strategy
for the detection of MSK pain and RDs is equivalent to that applied in community studies in Mexico. Overall prevalence found
in our study was higher than that reported in the biggest epidemiological study of RDs in Mexico.3 The prevalence of MSK pain is
higher than that reported by other Mexican populations (ranging
from 7.1% to 43.7%) including Aldama City population (13.0%).
Even when our study was conducted with patients who have
medical coverage, and they were in the health centers at the time
of the interviews, only 49% of patients with present pain in the last
7 days had gone for medical assistance to treat their discomfort.
4
www.jclinrheum.com
However, 65% of the patients with pain had a treatment established. Musculoskeletal pain is frequently treated on the basis of
self-medication, which was reported to have reached 26.9%.
By far the most common self-prescribed drugs for MSK pain were
NSAIDs (81.3%), which unexplainably are available without
medical prescription at full therapeutic doses in Mexico; the rate
for self-prescription of NSAIDs in our population is consistent
with other studies in our country.3 Self-prescription represents a
potential risk for the patient’s health. In this specific case, with
NSAIDs as the most used drugs, gastrointestinal and renal complications may occur.24–26 In patients with non–trauma-related
MSK pain, the use of alternative medicine was reported by
24.5%, whereas the epidemiological study in Mexico reported
1.3%.3 The high use of this type of medication could be related
to the socioeconomic level of the studied population and also to
cultural intertias. Even when the economic income was not considered as part of the study, we could infer that our population
has a low socioeconomic level because of the type of health
coverage used by them. They may seek the alternative treatment because it represents a lower cost rather than buying another
treatment options.
The COPCORD-positive individuals reported a high functional impairment (69.8%), and 33.8% of them perceived this disability as severe. However, despite these rates and although 55.1%
of these individuals had sought for professional help, only 18.8%
had a diagnosis established. This could mean that there are multiple cases of RDs that are underdiagnosed, which at some point
could end with some type of disability. Importantly, our results uncover a potential area of opportunity for the Popular Healthcare
System to improve the skills of primary care physicians in the
detection of patients with potential RD, and in this way, these
patients can be directed to the rheumatologist for a definitive diagnosis and early treatment. Early accurate referral of patients with
inflammatory RD has become a primary objective in modern
rheumatology and requires continual medical education to primary care physicians; such referral is crucial to gain advantage
of the therapeutic windows, especially at early stages. As can be
noted, the situation in Chihuahua is far from ideal.
TABLE 4. Prevalence of RDs and MSK Disorders
Diagnosis
COPCORD negative
RD
OA
RRPS
RA
Mechanic low-back pain
Fibromyalgia
Gout
Nonclassified arthritis
Ankylosis spondylitis
Systemic lupus erythematosus
Juvenile idiopathic arthritis
Reactive arthritis
MSK disorders
Associated with neurologic disorders
Associated with vascular disorders
Osteoporosis
n (%)
95% CI
747 (74.3)
71.6–76.8
104 (10.3)
55 (5.5)
14 (1.4)
14 (1.4)
9 (0.9)
8 (0.8)
3 (0.3)
3 (0.3)
3 (0.3)
1 (0.1)
1 (0.1)
8.6–12.4
4.1–7.0
0.8–2.2
0.7–2.2
0.4–1.6
0.3–1.4
0.0–0.7
0.0–0.7
0.0–0.6
0.0–0.3
0.0–0.3
29 (2.9)
11 (1.1)
4 (0.4)
2.0–4.0
0.5–1.8
0.1–0.8
RRPS indicates rheumatic regional pain syndrome.
© 2016 Wolters Kluwer Health, Inc. All rights reserved.
�JCR: Journal of Clinical Rheumatology • Volume 00, Number 00, Month 2016
In our study, OA was the most prevalent RD (10.3%), and the
prevalence of RA was 1.4%. These findings, like those found for
other RDs, are generally consistent with prevalence rates reported
in other regions of Mexico including Aldama City,3 and specifically the RA prevalence was found to be greater than that reported
in the world population (0.23%).27
Although our results provide valuable data of our population,
the limitations of our study are worth mentioning. Even if the
study was limited to gathering information from community
clinics of Popular Healthcare System in Chihuahua, leaving aside
the population of people who have other medical coverage and
those who have none, nevertheless the population attending these
centers is the most representative of Chihuahua City. Moreover,
although 2 of the largest health centers in the city were included,
it was not possible to survey the beneficiaries from all community
clinics of this health care system, so sampling bias could affect
our results.
In addition, only 72.7% of COPCORD-positive patients
completed their medical care until a definitive diagnosis, whereas
the remaining patients could not be diagnosed because of the lack
of commitment to attend subsequent medical appointments or laboratory studies. Therefore, the prevalence in our study could be
underestimated. This lack of interest of patients to reach a diagnosis may reflect the reason why our findings show that although our
survey respondents have medical care, there is a high prevalence
of MSK pain and a low percentage of individuals with a definitive
diagnosis and an optimal treatment.
The fact that the rheumatologist assessed only the inflammatory diseases was also a limitation. The patients with noninflammatory diseases could have needed a follow-up by a
rheumatologist, although such follow-up was given by a general
practitioner. Moreover, RRPS was diagnosed under the clinical
judgment of non-rheumatologist physicians, which could lead to
underestimation or overestimation of this disease.
Our research allowed us to establish a definitive diagnosis in
192 patients previously not diagnosed (74.7% new diagnoses).
Moreover, our study allowed gathering important information
about the diseases of the MSK system in the population benefited
by the Mexican Popular Healthcare System in Chihuahua City.
This medical service provides coverage to much of the national
(15,394,890 families), state (408,892 families), and municipality
(87,342 families) population.16 The data found show a high prevalence of MSK pain and a high rate of functional impairment in
patients reflecting the impact of these diseases in the population.
This information can be used to design goal-oriented prevention
and therapeutic programs for this population. It is clear that there
is a significant room for improvement, and our information may
also be used as a reference to analyze the situation in other cities
of our country in similar scenarios. A critical review of the rheumatology skills in primary practitioners should be coordinated,
and if needed, a corrective plan can be tailored with the combination of this information.
ACKNOWLEDGMENTS
The authors acknowledge the support of the Health Department of Chihuahua’s government to conduct our research in the
community clinics of Chihuahua City. The authors thank the medical students of the Faculty of Medicine at the Autonomous University of Chihuahua for their valuable participation in the
survey administration.
REFERENCES
1. Chopra A. The COPCORD world of musculoskeletal pain and arthritis.
Rheumatol Oxford. 2013;52:1925–1928.
© 2016 Wolters Kluwer Health, Inc. All rights reserved.
COPCORD Chihuahua México
2. Chopra A, Abdel-Nasser A. Epidemiology of rheumatic musculoskeletal
disorders in the developing world. Best Pract Res Clin Rheumatol.
2008;22:583–604.
3. Pelaez-Ballestas I, Sanin LH, Moreno-Montoya J, et al. Epidemiology of
the rheumatic diseases in Mexico. A study of 5 regions based on the
COPCORD methodology. J Rheumatol Suppl. 2011;86:3–8.
4. Ariza-Ariza R, Mestanza-Peralta M, Cardiel MH. Direct costs of medical
attention to Mexican patients with rheumatoid arthritis in a tertiary care
center. Clin Exp Rheumatol. 1997;15:75–78.
5. Cardiel MH. Present and future of rheumatic diseases in Latin America.
Are we prepared to face them? Reumatol Clin. 2011;7:279–280.
6. Torres AC, Knaul FM. Determinantes Del Gasto De Bolsillo En Salud e
Implicaciones Para el Aseguramiento Universal en México: 1992–2000.
Caleidosc Salud. 2003:209–225.
7. Chopra A. COPCORD–an unrecognized fountainhead of community
rheumatology in developing countries. J Rheumatol. 2004;31:2320–2322.
8. Reyes-Llerena GA, Guibert-Toledano M, Penedo-Coello A, et al.
Community-based study to estimate prevalence and burden of illness of
rheumatic diseases in Cuba: a COPCORD study. J Clin Rheumatol.
2009;15:51–55.
9. Muirden KD. Community Oriented Program for the Control of Rheumatic
Diseases: studies of rheumatic diseases in the developing world. Curr Opin
Rheumatol. 2005;17:153–156.
10. Chopra A. The WHO-ILAR COPCORD Bhigwan (India) model:
foundation for a future COPCORD design and data repository. Clin
Rheumatol. 2006;25:443–447.
11. Alvarez-Nemegyei J, Peláez-Ballestas I, Sanin LH, et al. Prevalence of
musculoskeletal pain and rheumatic diseases in the southeastern region of
Mexico. A COPCORD-based community survey. J Rheumatol Suppl.
2011;86:21–25.
12. Rodriguez-Amado J, Peláez-Ballestas I, Sanin LH, et al. Epidemiology
of rheumatic diseases. A community-based study in urban and rural
populations in the state of Nuevo Leon, Mexico. J Rheumatol Suppl.
2011;86:9–14.
13. Cardiel MH, Rojas-Serrano J. Community based study to estimate
prevalence, burden of illness and help seeking behavior in rheumatic
diseases in Mexico City. A COPCORD study. Clin Exp Rheumatol. 2002;
20:617–624.
14. México en Cifras: Aldama, Chihuahua. Available at: http://www3.inegi.
org.mx/sistemas/mexicocifras/default.aspx?e=08. Accessed May 22, 2015.
15. Instituto Nacional de Estadística y Geografía (2010) Censo de Población
y Vivienda 2010. Available at: http://www3.inegi.org.mx/sistemas/
TabuladosBasicos/Default.aspx?c=27303&s=est. Accessed
November 13, 2014.
16. México en Cifras: Chihuahua, Chihuahua. Available at: http://www3.inegi.
org.mx/sistemas/mexicocifras/. Accessed May 22, 2015.
17. Goycochea-Robles M-V, Sanin LH, Moreno-Montoya J, et al. Validity of
the COPCORD Core Questionnaire as a classification tool for rheumatic
diseases. J Rheumatol Suppl. 2011;86:31–35.
18. Altman R, Alarcón G, Appelrouth D, et al. The American College of
Rheumatology criteria for the classification and reporting of osteoarthritis
of the hand. Arthritis Rheum. 1990;33:1601–1610.
19. Altman R, Alarcón G, Appelrouth D, et al. The American College of
Rheumatology criteria for the classification and reporting of osteoarthritis
of the hip. Arthritis Rheum. 1991;34:505–514.
20. Peat G, Thomas E, Duncan R, et al. Clinical classification criteria for knee
osteoarthritis: performance in the general population and primary care.
Ann Rheum Dis. 2006;65:1363–1367.
21. Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis
classification criteria: an American College of Rheumatology/European
League Against Rheumatism collaborative initiative. Arthritis Rheum.
2010;62:2569–2581.
www.jclinrheum.com
5
�Del Río Nájera et al
JCR: Journal of Clinical Rheumatology • Volume 00, Number 00, Month 2016
22. Pelaez-Ballestas I, Flores-Camacho R, Rodriguez-Amado J, et al.
Prevalence of Back Pain in the Community. A COPCORD-based study
in the Mexican population. J Rheumatol Suppl. 2011;86:26–30.
25. Bjarnason I, Hayllar J, MacPherson AJ. Russell AS (1993) Side effects
of nonsteroidal anti-inflammatory drugs on the small and large intestine
in humans. Gastroenterology. 1993;104:1832–1847.
23. Alvarez-Nemegyei J, Peláez-Ballestas I, Rodríguez-Amado J, et al.
Prevalence of rheumatic regional pain syndromes in adults from Mexico:
a community survey using COPCORD for screening and
syndrome-specific diagnostic criteria. J Rheumatol Suppl. 2011;86:15–20.
26. Pirmohamed M, James S, Meakin S. Adverse drug reactions as cause of
admission to hospital: prospective analysis of 18 820 patients. BMJ.
2004;329:15–19.
24. Brater DC. Anti-inflammatory agents and renal function. Semin Arthritis
Rheum. 2002;32:33–42.
6
www.jclinrheum.com
27. Cross M, Smith E, Hoy D, et al. The global burden of rheumatoid arthritis:
estimates from the Global Burden of Disease 2010 study. Ann Rheum
Dis. 2014;73:1316–1322.
© 2016 Wolters Kluwer Health, Inc. All rights reserved.
�
 Ingris Peláez-Ballestas
Ingris Peláez-Ballestas