Cytokine & Growth Factor Reviews 24 (2013) 1–12
Contents lists available at SciVerse ScienceDirect
Cytokine & Growth Factor Reviews
journal homepage: www.elsevier.com/locate/cytogfr
Survey
The role of ‘‘anti-inflammatory’’ cytokines in axon regeneration
Pı́a M. Vidal, Evi Lemmens, Dearbhaile Dooley, Sven Hendrix *
Dept. of Morphology & Biomedical Research Institute, Hasselt University, Belgium
A R T I C L E I N F O
A B S T R A C T
Article history:
Available online 15 September 2012
The injured central and peripheral nervous system (CNS and PNS) are difficult to regenerate due to the
presence of growth inhibitory molecules which are upregulated around the lesion site. In addition, a
strong inflammatory response triggering the production of so-called ‘‘pro’’- and ‘‘anti-inflammatory’’
cytokines, adds to this dilemma. Both pro- and anti-inflammatory cytokines are involved in the
regulation of diverse signaling pathways. One of the main aims to induce regeneration is to promote
axonal outgrowth and stimulate the formation of new connections. Anti-inflammatory cytokines as
modulators of neurite plasticity and outgrowth are of pivotal importance in neuroregeneration with
different effects reported. Here we summarize the most relevant information about IL-4, IL-10, IL-13, LIF
and TGF-b focusing on their direct and indirect role in axonal outgrowth.
ß 2012 Elsevier Ltd. All rights reserved.
Keywords:
CNS regeneration
PNS regeneration
Spinal cord injury
IL-4
IL-13
IL-10
TGF-b
LIF
Contents
1.
2.
3.
4.
5.
What are anti-inflammatory cytokines? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Are anti-inflammatory cytokines immunosuppressants? . . . . . . . . . . . . . . . . . . . . . . . . . .
1.1.
Axonal growth and the immune system. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Distinct inflammatory phases after injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3.1.
Effects of anti-inflammatory cytokines depend on the immune phase, the compartment
3.2.
Direct and indirect effects of ‘‘anti-inflammatory’’ cytokines . . . . . . . . . . . . . . . . . . . . . . .
Effects of anti-inflammatory cytokines in the peripheral and central nervous system . . . . . . . .
Interleukin-4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.1.
4.2.
Interleukin-10 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Interleukin-13 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.3.
4.4.
Leukemia inhibitory factor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Transforming growth factor-b . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.5.
Concluding remarks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1. What are anti-inflammatory cytokines?
The activity of cytokines was first recognized in the mid 1960s,
when supernatants derived from in vitro cultures of lymphocytes
were found to contain factors that could regulate proliferation,
differentiation, and maturation of allogeneic immune cells, induced
by activation with antigen or with nonspecific mitogens [1].
* Corresponding author at: Dept. of Morphology & Biomedical Research Institute,
Hasselt University, Agoralaan, Building C, B-3590 Diepenbeek, Belgium.
Tel.: +32 11 26 9246; fax: +32 11 26 9299.
E-mail address: sven.hendrix@uhasselt.be (S. Hendrix).
1359-6101/$ – see front matter ß 2012 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.cytogfr.2012.08.008
...............
...............
...............
...............
and the cell type .
...............
...............
...............
...............
...............
...............
...............
...............
...............
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
1
2
2
4
5
5
6
6
6
8
8
9
9
9
The definitions of cytokines available in the literature tend
to be a bit vague and vary among the authors [1–5]. In this
review, we base our concept of cytokines on the definitions
summarized in Table 1. Cytokines are proteins with pleiotropic,
redundant, synergetic and/or antagonistic effects mediated via
several signaling cascades, which permit them to regulate
cellular activity (such as proliferation, differentiation and
maturation) in a coordinated and interactive way over extensive
networks.
The terms ‘‘cytokine’’ and ‘‘growth factor’’ are sometimes—but
not always—used interchangeably. Therefore, in this review we
refer to ‘‘Transforming growth factor-b (TGF-b)’’ as a growth factor
and cytokine although this may seem pleonastic.
�2
P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
Table 1
Cytokine concepts.
Cytokine definition
Reference
Cytokines are small proteins that assist in regulating the development of immune effector cells and/or possess direct effector functions.
They are capable of regulating interactions among lymphoid cells, inflammatory cells and hematopoietic cells, thus mediating
cell–cell communication. They bind to receptors, thereby triggering signal transduction pathways that ultimately alter gene
expression in target cells.
Cytokines are multifunctional pleiotropic proteins that play crucial roles in cell–cell communication and cellular activation.
Functionally, cytokines have been classified as being merely pro-inflammatory (type 1) or anti-inflammatory (type 2).
Cytokines function as intracellular messenger molecules and are defined mainly through their regulatory effects on immune cells.
Cytokines are inflammatory mediators important in the host’s response to pathogens and other (foreign) challenges.
Cytokines are small cell-signaling molecules secreted by different cell types throughout the body. They can be classified as proteins,
glycoproteins or peptides, mainly related to intercellular communication.
[1]
Functionally, cytokines and the cells that secrete them have
been classified as either pro-inflammatory (stimulatory, or T
helper cell type 1 [Th1] or type 1) or anti-inflammatory
(inhibitory or T helper type 2 [Th2] or type 2). In most
publications, the terms pro-inflammatory, stimulatory, T helper
cell type 1 [Th1] or type 1 are used interchangeably, although it
is semantically not correct to use them as synonyms. Similarly,
anti-inflammatory, inhibitory, T helper cell type 2 [Th2] or type
2 are also all common terms used.
Type 1 cells mainly activate macrophages and control
infections; meanwhile type 2 cells activate B cells and eradicate
extracellular parasites (reviewed in [6]). However, most of the
cytokines have an overlap in function, exerting both pro- and
anti-inflammatory effects depending on the tissue milieu, which
often makes it difficult to understand the actual effect they
induce as mediators of the immune response. For example, it has
been suggested that some so-called ‘‘anti-inflammatory’’ cytokines, such as interleukin-4 (IL-4), interleukin-10 (IL-10) and
TGF-b may present pro-inflammatory properties under certain
experimental conditions [7] (see below). It has been suggested
that a T cell subpopulation, called T helper type 2 cells, might be
particularly beneficial following CNS and PNS lesions and after
neuropathic pain following peripheral nerve injury, especially by
producing the anti-inflammatory cytokines IL-4 and IL-10 [8].
To present the message of this review clearly, we consider
‘‘anti-inflammatory’’ cytokines as molecules that control the
‘‘pro-inflammatory cytokine response’’ (see below: ‘‘Are antiinflammatory cytokines immunosuppressants?’’). This limits the
effects of sustained or excessive inflammation which can be
detrimental for the proper functioning of tissues and organs, such
as the regulation of IL-1 and tumor necrosis factor-a (TNF-a)
levels [9]. The ‘‘anti-inflammatory’’ cytokines may be secreted by
immune cells such as activated lymphocytes, macrophages,
microglia and mast cells at or near the site of injury, thus acting
mostly locally.
We have focused in this review on the role of selected socalled anti-inflammatory cytokines, namely IL-4, IL-10, TGF-b,
IL-13 and leukemia inhibitory factor (LIF), in axonal regeneration, in light of a possible new therapeutic application after CNS
damage.
1.1. Are anti-inflammatory cytokines immunosuppressants?
The term ‘‘anti-inflammatory cytokines’’ seems to suggest that
these factors suppress immunity similarly to high doses of
corticosteroids, however, this is a wide-spread misunderstanding
also shared by many immunologists which is—at least in part—a
result of the history of immunology [10]. Historically, the first
original immunological experiments were focussed on Th1dominated immune processes such as the tuberkulin reaction.
Therefore, immunologists may tend to consider factors that
suppress these processes as immunosuppressant. However, quite
[2]
[3]
[4]
[5]
often, simply a different type of immune reaction is replacing the
original process [10]. Classical immunosuppressants such as
corticosteroids only suppress all immune reactions when applied
in high doses, while lower doses are only immunomodulatory.
Furthermore, the canonical type-2 cytokines IL-4 and IL-13 play
key roles during the strong inflammatory responses in allergic
diseases such as asthma and atopic dermatitis and can definitely
not be labeled ‘‘anti-inflammatory’’ in this context. Following this
concept, ‘‘anti-inflammatory’’ cytokines should be considered
immunomodulators that inhibit classical type-1 (Th1) and delayed
type hypersensivity (DTH) responses [10], however they are not
‘‘immunosuppressants’’. Therefore, we consider the label ‘‘antiinflammatory’’ as partially misleading and prefer to use it only
with quotation marks.
2. Axonal growth and the immune system
After axotomy, the ends of lesioned axons possess little
capability to regrow or elongate; they are able to sprout fibers
until they are near to, or in contact with the region of scar tissue
formation, where several classes of growth inhibitory molecules
are being upregulated [11,12]. These dynamic and constantly
moving growth cones contain all the machinery required for
membrane remodeling, thereby inducing expression/degradation
of surface molecules or receptors in response to repulsive guidance
factors. However, unfortunately this does not lead to overt axonal
regeneration over large distances [11]. It is believed that the
protein synthesis occurring inside the growth cones is used
primarily for direction and not for extension [13], and this
direction is dependent on the level of cyclic nucleotides (cAMP and
cGMP) [13]. On the other hand, direction and length of growth are
related, since growth is modulated by the action of attractive and
repulsive cues upon growth cones.
It is important to note, that axon regeneration mostly takes
place in a disturbed immune milieu and that axon growth is
substantially modulated by immune factors [6]. Interestingly,
many factors that are potent attractive or repulsive factors of axon
growth and are influenced by immune factors (Table 2) exert
themselves immunological functions (Table 3).
For instance, positive and negative regulators are involved in
the modulation of cytokine and chemokine levels and activities,
angiogenesis, survival processes as well as modulation of
macrophages and T cell activation (Table 3). On the other hand,
cytokines may influence the expression of axon growth modulators and their receptors as well as their intracellular signaling.
Finally, immune factors may not only directly influence axonal
outgrowth but may also modulate indirectly attractive and
repulsive cues. Therefore, it is no surprise that immunological
responses triggered after central or peripheral nervous system
injury are very complex and some studies have shown that
inflammation has beneficial effects after injury, while others have
shown the opposite (reviewed in [6]).
�Table 2
‘‘Anti-inflammatory’’ cytokines modulate positive and negative regulators of axon growth.
Positive regulators
Neurotrophic factors
(BDNF, NGF, NT-3, NT-4)
Interleukin-10
Interleukin-13
Tumor growth factor-b
Leukemia inhibitory factor
It stimulates immune cells to
produce NT-3 mRNA [3]
High doses increase NT-4
inducing outgrowth in DRG
neurons [47]
BDNF, IL-10 and TGF-b are
expressed after
transplantation of GAspecific cells in an EAE
model [109]
IL-10 levels increase after
NGF and BDNF treatment in
dendritic cells [110]
NGF stimulates IL-13 secretion
and modulates IgE-mediated
responses in human basophils
[111]
TGF-b increases the
chemotactic action of NGF in
microglia cells [112]. TGF-b3
and NT-3 enhance spiral
ganglion neuronal survival
[113]; similar to TGF-b5 with
NT-3 and TGF-b5 plus BDNF
[114]
Rho regulates TGF-b1
activation of keratocytes
mediating phenotypic [117]
and morphological effects of
TGF-b1 in stress fiber
formation [118]
RhoA regulates
posttranscriptional regulation
of TGF-b in apoptotic cells
[119]
TGF-b induces an increase of
ATP-inducing calcium
mobilization in A59 cells
(human lung cancer cell line)
augmenting cellular migration
[123]
LIF acts synergically with NT-3 and
BDNF to promote neuronal survival
in spiral ganglion cells [114]
Rho-GTPases
IL-4 induces expression of an
activator of Rho-GTPase
proteins, Dock10, in B cells
[115]
Moderate calcium
concentrations (100 nM)
IL-4 inhibits calcium transients
in airway smooth muscle cells
and modulates [Ca2+]i levels
[120]
IL-4 stimulates increase in
calcium activated potassium
channels [121]
IL-4 induces cAMP and cGMP
accumulation in a dose dependent manner in
monocytes [125]
Cyclic nucleotide
("cAMP and cGMP)
IL-13 induces upregulation of
RhoA in human bronchial
smooth muscle cells, which is
inhibited by an inhibitor of
STAT6 [116]
IL-10 suppresses human
osteoclastogenesis by
attenuating calcium
pathways [122]
IL-13 partly inhibits the
calcium activated potassium
channels in response to IL-4
[121]
IL-10 mediates inhibitory
effects of cAMP elevating
agents on bone marrowderived dendritic cells
[126]
IL-13 enhances arginase mRNA
and protein expression in rat
aortic smooth muscle cells,
possible by cAMP [127]
This cytokine induces a
downregulation of NO
production through arginase
induction via cAMP/PKA in
macrophages [128]
Negative regulators
High calcium
concentrations (>200 nM)
Neurotrophic factors
(NGF, NT-3, NT-4)
Fibrotic and glial scar
components (tenascin,
fibronectin, MBP, MAG, MOG)
Low IL-4 concentrations
suppress neurite outgrowth
induced by NGF and NT-4 in
DRG cells [47]
IL-4 increases Tenascin-C
mRNA and secretion on
cultured keratinocytes [133]
IL-13 induces tenascin-C
expression in fibroblasts [134]
In immature airway smooth muscle
cells, acetylcholine-induced [Ca2+]i
response is enhanced after LIF
treatment [124]
TGF-b upregulates CREB levels
in advanced breast cancer cells
[129]
Chronic exposure to TGF-b
decreases cAMP-driven Clsecretion (ion transport) in T84
epithelial cells [130]
TGF-b1 increases intracellular
Ca2+ concentration, leading to
an enhancement of cell
adhesion [131]
TGF-b1 reduces NT3 mRNA
levels in a dose and time dependent manner in Schwann
cells [132]
TGF-b stimulates astrocytic
expression of fibronectin and
tenascin [31] and promotes the
formation of cell clusters that
accumulate extracellular
matrix molecules [107]
P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
Interleukin-4
LIF induces tenascin-C and
fibronectin in myoblast cells [135]
LIF is required for myelination
during development of mouse optic
nerve, because a reduction of MPB
was seen in LIF / mice [136]
Abbreviations: Brain derived neurotrophic factor (BNDF), calcium (Ca2+), cAMP response element-binding (CREB), cyclic adenosine monophosphate (cAMP), cyclic guanoside monophosphate (cGMP), dorsal root ganglion (DRG),
experimental autoimmune encephalomyelitis (EAE), immunoglobulin E (IgE), glatiramer acetate (GA), interleukin 4 (IL-4), interleukin 10 (IL-10), interleukin 13 (IL-13), leukemia inhibitory factor (LIF), nerve growth factor (NGF),
neurotrophin factor 3 (NT-3), neurotrophin factor 4 (NT-4), myelin binding protein (MBP), myelin associated glycoprotein (MAG), myelin oligodendrocyte glycoprotein (MOG), nitric oxide (NO), protein kinase A (PKA), Ras homolog
gene family, member A (RhoA), signal transducer and activator of transcription (STAT6), transforming growth factor-b (TGF-b).
3
�4
P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
Table 3
Axon growth-modulating factors with immunological functions.
Molecules
Examples of functions/effects in the immune system
Reference
Netrin-1
Its administration before or after ischemia-reperfusion injury protects kidneys by suppressing leukocyte
infiltration. The authors suggest that netrin-1 suppresses cytokine and chemokine production in these cells
Netrin-1 administration reduces the levels of inflammatory cytokines within the alveolar space, reducing the
intra-alveolar inflammation during acute lung injury (ALI) in a porcine model
Macrophage migration mediated by TGF-b is regulated by activation/inactivation of RhoA
RhoA and its downstream effector ROK are activated in synovial tissue of rheumatoid arthritis (RA) patients.
The blockage of ROK inhibits pro-inflammatory cytokine production via inhibition of NF-kB activation
Ca2+ dependent signaling pathways mediate gene induction and repression of activated T cells from patients
with severe-combined immunodeficiency
LPS induces HMGB1, a chromatin binding factor that acts as a late mediator of mortality in murine
endotoxemia and sepsis, released by Ca2+-dependent signals
T cell proliferation is inhibited in human T cells expressing cGK1, stimulated with NO and cGMP analogs
Neutrophil retraction is regulated by an increase in intracellular cAMP levels in response to chemoattractants
NGF interacts directly with endothelial cells in vitro and induces an angiogenic response in the chick embryo in vivo
BDNF, NGF, NT-3 or NT-4 increase viability of eosinophils from bronchoalveolar lavage fluid
Tenascin–C expressed in glioblastoma cells inhibits the migration of T cells
Fibronectin induces a more immature phenotype on dendritic cells, leading an increase in their endocytic ability
[137]
Rho-GTPases
Calcium
cAMP/cGMP
Neurotrophins
Glial scar compounds
[138]
[139]
[140]
[141]
[142]
[143]
[144]
[145]
[146]
[147]
[148]
Abbreviations: Brain derived neurotrophic factor (BNDF), calcium (Ca2+), cyclic adenosine monophosphate (cAMP), cyclic guanoside monophosphate (cGMP), cGMP-activated
kinase 1 (cGK1), high-mobility group protein B1 (HMGB1), lipopolysaccharide (LPS), nerve growth factor (NGF), neurotrophin factor 3 (NT-3), neurotrophin factor 4 (NT-4),
nuclear factor kappa B (NF-kB), nitric oxide (NO), Ras homolog gene family A (RhoA), Rho-associated protein kinase (ROK), transforming growth factor–b (TGF-b).
3. Distinct inflammatory phases after injury
Inflammation is part of the initial response injury and is
characterized in the acute phase by increased blood flow and
vascular permeability, with accumulation of fluid (edema formation), leukocytes and inflammatory mediators, such as cytokines.
The immune response also varies according to location, with
differences for instance between the CNS and PNS. It has been
suggested that inflammation in the nervous system might be sitespecific with characteristic immunological molecules involved. For
example, the response of T cells to axonal injury is more limited in
the CNS than in the PNS and T cell apoptosis occurs extensively in
the injured CNS when compared to the PNS [14]. In addition, the
time-course of the injury and its repair is of pivotal importance.
After CNS injury, phase-specific immune responses are starting to
be recognized (Kramer & Hendrix unpublished observations; [15]).
After spinal cord injury (SCI), at least four main stages can be
distinguished: acute, sub-acute, early chronic and chronic phase.
The acute phase, which typically lasts for a few hours, is
characterized by an upregulation of pro-inflammatory cytokines,
such as IL-1b and TNF-a [16,17]. This phase has been defined by an
augmentation in damage, i.e. neuronal and axonal destruction, as
well as demyelination close to the injury site [18]. There is also an
infiltration of neutrophils, reaching the highest level 1 day after
injury [19], and activated B and T cells increase in the spleen and
bone marrow [20]. In the sub-acute phase, between 2 and 7 days
after injury, the levels of some pro-inflammatory cytokines start to
decrease [15,17]. Meanwhile, there is an increase in the number of
monocytes and lymphocytes and the levels of anti-inflammatory
factors (Fig. 1). Examples of molecules involved in the acute
inflammatory phase are the cytokines IL-1b, IL-6, IL-8, IL-11 and
TNF-a as well as the chemokines granulocyte colony-stimulating
factor (G-CSF) and granulocyte-macrophage colony-stimulating
factor (GM-CSF). Together these factors activate macrophages,
neutrophils as well as natural killer cells. During the acute and subacute phases, recovery of locomotor skills in rodents is observed.
CNS
A
Relative mRNA levels
LIF
TGF- β
IL-4
IL-10
24
0
Hours
Time frame
7
Days
6
Weeks
PNS
Relative mRNA levels
B
IL-4
IL-10
24
0
Time frame
Hours
7
Days
6
Weeks
Fig. 1. Temporal expression patterns of ‘‘anti-inflammatory’’ cytokines in SCI and PNI of rodents. (A) Curves represent mRNA levels after SCI for IL-4, IL-10, LIF, and TGF-b. (B).
Curves represent mRNA levels after PNI for IL-4 and IL-10. Curves were adapted and generated using data from the following references: [15,17,46,47,53,106–108] and own
unpublished data.
�P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
Later on, the early chronic and later chronic phases are
characterized by the development of specific humoral and cellular
immune responses directed to facilitate cleaning of the injury site
[15]. This time frame can last weeks or even months. During these
two phases, the levels of T cells, macrophages and neutrophils start
to increase again showing a second peak of these immune factors.
It is not clear whether this is related to changes in functional
recovery. It has been suggested that inflammation may support
regeneration in the chronic phase because a reduction of
macrophage/microglial infiltration lead to a decrease in functional
recovery following SCI [19,20].
3.1. Effects of anti-inflammatory cytokines depend on the immune
phase, the compartment and the cell type
Axonal growth is actively promoted during the development of
the CNS and PNS in mammalian vertebrates. Conversely, in the
adult CNS, axon extension is limited even after axotomy. This is in
part due to a limited expression of proteins that can promote rapid
growth during development and adult peripheral nerve regeneration [21]. The presence of structural barriers (e.g. scar tissue) and
molecules (e.g. myelin inhibitory molecules such as NogoA) [22], as
well as the complex inflammatory response generated after injury,
are also responsible for limiting axonal regeneration.
Cellular types such as microglia, astrocytes and oligodendrocytes play a central role during CNS inflammation, as they can
produce and modulate the secretion of cytokines and growth
factors. Microglia are among the first cells to be activated after CNS
injury, thus initiating the response to brain injury, while the other
cellular types are mainly involved in intermediate or later
responses [2,15,23].
Although the immune response is one of the first reactions to
occur following injury to the nervous system, there is still
controversy in the literature about the role of the immune system,
especially T cells and macrophages, in nervous system repair. The
first inflammatory response in rodents is characterized by
infiltrating neutrophils, macrophages/microglia and T cells;
meanwhile in a later phase, the levels of macrophages and
neutrophils increase again peaking at around day 60 after injury
[19]. They can have either beneficial or detrimental effects after
damage (reviewed in [6]). For instance, after mechanical damage,
such as SCI, traumatic brain injury or crush injury of the optic
nerve, injections or vaccines of active autoimmune T cells specific
to myelin-associated proteins (MBP) or ovalbumin, lead to
improvement in some models and exacerbation in others [24].
This suggests that a specific molecular crosstalk between the
immune and nervous systems, determines the outcome of T cell
actions after damage. For instance, some studies provide convincing evidence that specific inflammatory cascades play a direct role
in axonal outgrowth [25], either by improving the integrity of
neurites [26] or by promoting cellular survival [27,28].
The environment within which a cytokine is produced may also
be responsible for its beneficial or detrimental effect; this means
that in a Th1-dominated immune milieu, a cytokine may have
‘‘suppressive’’ effects while the same cytokine may lead to a
dramatic exacerbation in a Th2-dominated environment [6]. For
example, TGF-b promotes neurite outgrowth from dorsal root
ganglia (DRG) explants, however, it neutralizes outgrowth
promoted by IL-1a or IL-1b [29]. Furthermore, cytokine effects
may dramatically be altered due to a change in the location; thus,
immune cells and their secreted factors may exert distinct effects
in one compartment (e.g. blood vessels or perivascular space)
whilst displaying other effects after invading a certain tissue (e.g.
brain parenchyma) [30].
In addition, there is extensive literature outlining that cytokines
exert cell-type-specific effects. For example, IL-4 seems to promote
5
the proliferation of fibroblasts [31] and endothelial cells [32], while
having anti-proliferative effects on other cellular types such as
carcinoma cells [33]. Striking examples of phase-specific effects of
anti-inflammatory cytokines have been described in other disease
contexts such as asthma, experimental autoimmune encephalomyelitis (EAE) as well as wound healing and pregnancy [34–38].
Studies using anti-IL-13 monoclonal antibodies to treat
asthma, have suggested that IL-13 may play a protective role in
acute inflammatory settings, while having a detrimental effect in
chronic inflammatory settings [34]. Similarly, blocking IL-4/IL-13
receptor prevents allergic airway inflammation in asthma, but has
no effect in the established disease, suggesting that both cytokines
play a predominant role in the acute onset of disease [35]. IL-10
may also have different effects depending on the time of application
in EAE, an animal model of multiple sclerosis; there is a delay in
the onset of the disease in IL-10 transgenic mice treated with anti-IL10 antibodies the day of immunization, while in mice treated 8 days
before immunization, this delay is absent [36]. Additionally,
anti-TGF-b1, 2 and 3 monoclonal antibodies also display different
effects on wound healing and hypertrophic scar formation. Early
treatment impairs wound healing and has no effect on scar
formation, while middle and later treatments reduce scar formation
[37]. Finally, it is known that LIF enhances embryonic implantation,
but it has no effect on early embryonic development [38].
Many researchers have achieved a substantial understanding of
the cellular mechanism behind these findings; however, much still
remains unknown due to the enormous complexities in both the
nervous and immune systems. It is also of pivotal importance that
the effects of cytokines may differ depending on the immunological milieu. However, it is safe to assume that the ability to
maximize specific immune elements, while suppressing others
that are aspects of the immune response responsible for further
damage, is critical for repair.
3.2. Direct and indirect effects of ‘‘anti-inflammatory’’ cytokines
In order to understand the contradictory effects reported about
cytokines, it is not only necessary to characterize the phasespecific and compartment-specific effects of the cytokines, but also
the direct and indirect effects on neurite growth. Direct effects of
cytokines are mediated via cytokine receptors on a neuron which is
directly stimulated or inhibited by a factor to regrow an axon. In
addition, cytokines may have indirect effects on axon growth by
influencing other cells and their secreted factors, for example by
stimulating astrocytes to produce neurotrophins [24]. It is known
that IL-13 is capable of modulating the inflammatory response by
suppressing the production of inflammatory mediators such as IL1b, TNF-a and IL-6 from microglia in vitro and in vivo [39,40]. In
Table 2 we have summarized selected examples of positive and
negative neurite growth modulators which are influenced by antiinflammatory cytokines. Another example is seen in EAE, where IL13 elicits an inhibitory function on MBP-directed T cell or B cell
immunoreactivity in vitro and in vivo [41]. The treatment of EAE
animals with RTL401, a peptide construct used to prevent relapses
and reverse EAE switching cytokines profiles, induces a reduction
of infiltrating mononuclear cells into the CNS and inflammatory
lesions in the spinal cord. It also preserves injured axons through a
strong Th2 response and is accompanied by upregulated IL-13
levels in the spleen, blood, spinal cord and brain [42]. These data
suggest that IL-13 is involved in the preservation of injured axons
in the spinal cord and the reversal of clinical signs of EAE via
suppression of the induction of type 1-mediated autoimmune
responses. Studies using vaccination models for the treatment of
CNS injury have shown that type 2-inducing adjuvants prevent the
development of EAE and promote axon regeneration [43]. In
addition, type 2 cells promote neuronal survival better than type 1
�6
P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
cells in vitro [24], while in brain slices, type 2 cells suppress type 1induced inflammatory signals [44]. Thus, the induction of a Th2
milieu may be another important indirect effect of the antiinflammatory cytokines described here.
During CNS and PNS trauma, we consider the cytokine/
neurotrophin axis [45] to be of particular interest. After trauma,
nerve growth factors (such as neurotrophins) and cytokines are
mostly present at the same time. From an evolutionary point of
view, it seems plausible that these two systems are closely
intermingled and display synergistic effects. For example, using
DRG explants we demonstrated that neurotrophin-induced
neurite outgrowth is dose-dependently modulated by pro- and
anti-inflammatory cytokines such as TNF-a, IFN-g, IL-4 and IL-6.
These data suggest a significant relation between neurotrophins
and cytokines in the response after peripheral nerve injury that
may help to modulate outgrowth and axonal regeneration [45].
4. Effects of anti-inflammatory cytokines in the peripheral and
central nervous system
In this part of the review we will focus on the effects of selected
‘‘anti-inflammatory’’ factors on neurite outgrowth and regeneration, namely IL-4, IL-10, IL-13, LIF and TGF-b.
4.1. Interleukin-4
IL-4 is a 30 kDa protein that is produced mainly by mature Th2
cells, mast cells, B cells and stromal cells. It plays a key role in
inducing CD4+ T cells to differentiate into type 2 cells, while
suppressing the development of type 1 cells. It has been shown
that after sciatic nerve injury, there is a downregulation of IL-4
mRNA levels in the ipsilateral DRG within hours after injury, while
on the other hand, pro-inflammatory levels are upregulated
[46,47], suggesting a positive role of IL-4 after peripheral nerve
injury (PNI). Similarly to IL-10, it also has positive effects on axonal
regeneration. In a model of PNI, IL-4 promoted facial motor neuron
survival after axotomy though STAT6 signaling [25], while in
retinal cell cultures, IL-4 enhanced the survival, by regulating the
cholinergic uptake in a dose- and time-dependent manner [48]. It
seems clear that IL-4 is capable of modulating cellular survival via
different signaling pathways depending on the environment. In
addition, IL-4 displays clear cell-type-specific effects. For example,
it promotes the proliferation of fibroblasts [31,33] and endothelial
cells [49], while it exerts anti-proliferative effects on tumor cells
such as renal cell carcinoma cells (RCC) [33] and breast and colon
cancer cell lines [32], possibly by the inhibition of angiogenesis
[50]. IL-4 also has biphasic effects; in vivo, low doses weakly induce
neovascularization, while high doses inhibit angiogenesis by
acting directly on endothelial cells. These biphasic or dual effects
of IL-4 are also seen in the case of migration, where low doses of the
cytokine (between 1 and 100 pg/mL) stimulate migration of
endothelial cells and high doses inhibit migration [50].
In cultured DRG cells, IL-4 has also been seen to modulate
peripheral axon regeneration (Table 4), suggesting even more that
T cells may affect neuroregeneration via local IL-4 secretion, which
in turn stimulates local neurotrophin secretion in a dose
dependent manner [45]. It has been suggested that IL-4 and NT3 have a synergistic relationship since this cytokine is able to
induce an enhancement of NT-3 mRNA expression in human
immune cells [3], while NT-3 enhances IL-4 production by
stimulated type 2 cells [51]. Since NT-3 is known to enhance
the release of neurotransmitters [52], these interactions may well
have an effect on synaptic efficacy and neuronal plasticity.
IL-4 has also been associated with the control of brain
inflammation and neuroprotective effects in the CNS. In this respect,
after SCI, IL-4 and IL-4Ra mRNA levels increased within 24 h after
injury while declining thereafter. IL-4 neutralizing antibodies do not
change the levels of pro-inflammatory cytokines, but lead to an
increase of ED1 immunoreactivity around the lesion site and
augmentation of the cavity 4 weeks after injury. This finding
suggests that IL-4 may endogenously exert protective effects
regulating the acute and chronic macrophage responses [53].
In rod photoreceptors, IL-4 protects against thapsigargin, a
potent inducer of apoptosis, by blocking cell death through the
cAMP/PKA pathway [54]; and, IL-4 also plays an important role in
controlling GABA-ergic and cholinergic phenotypes, where it can
stimulate the uptake of neurotransmitters in rat retina cultures
[48,55]. At the same time, IL-4 is able to enhance the survival of
hippocampal neurons in vitro, in a dose and time dependent
manner, since low concentrations (nM-mM) for less than 48 hours
have protective effects and high concentrations (mM) for a longer
incubation period, seem to be neurotoxic [27,28]. On the other
hand, treatment of hippocampal neuronal cultures with IL-4, leads
to increased proliferation of astrocytes and microglia [27]. In
microglial cells, IL-4 promotes growth, phagocytic functions as
well as proliferation [56], and inhibits the production of nitric
oxide (NO) and of pro-inflammatory cytokines such as TNF-a [57]
thus exerting a neuroprotective effect in the CNS. In astrocytes, IL-4
also has diverse functions, such as the inhibition of LPS-induced NO
synthesis due to blocking of inducible nitric oxide synthase (iNOS)
expression. A similar effect was seen in microglia, and additionally,
the induction of adhesion molecules such as ICAM-1 and the
induction of NGF secretion by cortical and cerebellar astrocytes
have also been observed [58]. Oligodendrocytes, the cells
responsible for myelin synthesis in the CNS, are also a source of
cytokines and NO under inflammatory conditions [59]. Both IL-4
and IL-10 protect against cell death, also by modulating iNOS
expression and NO production following LPS/IFN-g stimulation
[23]. In addition, IL-4 has been shown to increase oligodendrocyte
branching and maturation through microglia interaction [60].
However, analysis of neurites from newly formed neurons in cocultures of neuronal progenitor cells (NPCs) and microglia
previously treated with IL-4, did not significantly differ from the
culturing of NPCs alone [60].
In summary, IL-4 regulates cellular survival, proliferation and
branching in the PNS as well as in the CNS, and promotes
peripheral axon regeneration.
4.2. Interleukin-10
IL-10 is one of the most vastly studied ‘‘anti-inflammatory’’
cytokines and is mainly produced by monocytes/macrophages,
Th2 cells and B cells as an 18kDa protein. It inhibits monocytes/
macrophages and modulates lymphocyte and neutrophil
responses as well as cytokine production. More detailed information about its structure and function has been widely reviewed
previously [9].
Treatment with IL-10 increases both cell survival and axonal
regeneration after PNS injury. For example, after facial nerve
axotomy, flow cytometry analyses showed that the levels of IL-10,
amongst other cytokines, were increased [61], providing a
protective effect from cell death following injury to facial motor
neurons (FMN). It was shown that IL-10 works cooperatively with
CD4+ T cells, with T cells being involved in maintaining glialderived IL-10 levels in the vicinity of injured cell bodies [62]. In a
model of sciatic nerve injury, enhanced axon regeneration and
reduced glial scarring after administration of IL-10 was found [63],
while in retinal ganglion cells (RGCs), active glial cells express
iNOS, synthesizing high levels of NO which is toxic to neuronal
cells. IL-10 was able to increase the survival of axotomized RGCs
and the integrity of the axons of the nerve fiber layer (NFL) in vivo,
via the inhibition of NO synthesis, leading to a decrease in free
�7
P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
Table 4
Selected effects of IL-4, IL-10, IL-13, LIF and TGF-b on neurite outgrowth in PNS and CNS.
Cytokine
Effect
Experimental model
Specie
Reference
IL-4
Promotion of facial motoneuron survival after
axotomy
In the presence of neurotrophins, IL-4
modulates peripheral axon regeneration in a
dose dependent manner
Enhanced survival of axotomized RGCs,
reduction of monocytes in the NFL and
inhibition of NO production
Significantly increased number and length of
cell - bearing processes and increased cellular
survival
No effects on neurite length of newly formed
neurons from NPCs, but increases
oligodendrocyte branching
IL-10 enhances survival of axotomized RGCs
and improves axonal integrity of the nerve fiber
layers by inhibition of NO production
Increases of axonal regeneration and long term
(up to 8 weeks) improvement of locomotor
skills after a single dose of IL-10 (30 min after
injury)
Reduction of inflammation and neuronal
damage after SCI by systemic administration of
IL-10
Reduction of spinal tissue damage at 12 weeks
post injury by IL-10 (30 min before injury), MP,
or a combination of both agents, without
improvement of hindlimb locomotor function
Increase of neuronal survival and improvement
of motor function after IL-10 vector injections
(30 min after injury) up to 6 weeks after injury
LIF induces an increase of phosphorylated
Akt473 but no effect on dendrite growth in
hippocampal neurons
LIF increases diameter, number and conduction
velocity of the regenerated sciatic nerve
LIF augments corticospinal axon growth and
expression of NT-3 after spinal cord injury
LIF is unable to promote neurite arborization
and growth by itself; however, the addition of
LIF to cells treated with NGF increases neurite
length and induces neurite restructuration in
vitro. Furthermore LIF is required for
regeneration of injured sensory neurons in vivo
TGF-b1 reduces neurite extension of cerebellar
neurons
TGF-b has a weak positive effect on neurite
outgrowth in astrocytes
TGF-b1 inhibits the neurite outgrowth of
cortical neurons in vitro via activation of RhoA/
Rho-kinase pathway; while in vivo anti-TGF-b1
treatment promotes growth and preservation
of raphespinal axons caudally to the lesion site
and improves locomotor skills
TGF-b alone does not increase neurite
outgrowth in DRG neurons, but it is involved in
the stimulation of neurite growth by SPARC
Peripheral nerve injury (facial nerve axotomy)
Adult mice
[25]
DRG outgrowth model
E13 mouse
[47]
Transection of the optic nerve
Adult rats
[26]
Retinal cell culture
Postnatal rats
(1 or 2 days)
[50]
Co-culture of IL-4 treated microglia
with NPCs or oligodendrocyte
Adult mice
[62]
Transection of the optic nerve
Adult rats and rat
retinal ganglion cell line
[26,66]
Moderate SCI at T9 and T10 level in
Adult rats
[16]
Quisqualic acid (QUIS), a model of SCI,
between spinal segments T12-L2
Adult rats
[149]
Contusion spinal cord injury at T8 level
Adult rats
[78]
Laminectomy at T11-12 vertebral level
and also lateral hemisection of the
spinal cord at T13 level
Mouse hippocampal neurons from E16
embryos
Adult rats
[76]
E16 mouse
[99]
Transected sciatic nerve model
Adult rats
[93]
Hemisection at T7 level
Adult rats
[97]
Cultures of adult DRG neurons
Crush injury of the sciatic nerve in
LIF +/+ and LIF -/-mice of both sexes
Adult rats
Adult rats
[96]
[96]
Co-culture of cerebral astrocytes and meningeal
fibroblasts with cerebellar neurons
P1 rat DRG explants in 3-dimensional astrocytes
cultures
For the in vitro assay cortical neurons
from E18 were used and for the in vivo
experiments contusion spinal cord injury
at vertebral level T9-T10
Mice lumbar DRG from E13.5 embryos
Postnatal rats (1 or 2 days)
Postnatal rats (1 day)
E18 rats and adult rats
E13.5 mouse
[107]
[31]
[102]
[100]
IL-10
LIF
TGF-b
Abbreviations: Dorsal root ganglia (DRG), embryonic day (E), interleukin-4 (IL-4), interleukin-10 (IL-10), leukemia inhibitory factor (LIF), nerve growth factor (NGF),
neurotrophin factor 3 (NT-3), methylprednisolone (MP), nerve fiber layer (NFL), neuronal progenitor cells (NPCs), nitric oxide (NO), retinal ganglion cells (RGCs), secreted
protein acidic rich in cystein (SPARC), spinal cord injury (SCI), thoracic (T), transforming growth factor-b (TGF-b).
Remark: no published information is available that directly relates IL-13 with axonal/neurite outgrowth; therefore no data on IL-13 are included.
radicals [26]. Finally, IL-10 exerts a dose and time dependent
increase on RGCs survival by inhibiting apoptotic cell death by a
mechanism that involves activation of the STAT3 pathway, without
any effect on cellular proliferation [64]. It also induces a rapid
decrease in caspase-3 activity, but has no effect on intracellular
Ca2+ levels, whose levels are able to modulate caspase-3 induction,
suggesting that IL-10 has an intrinsic ability to inhibit directly or
indirectly, caspase-3 activity. It has also been suggested that cell
death occurs in neurons when NF-kB is permanently activated, for
instance after trauma [7] or toxic concentrations of glutamate [65],
and the inhibition of NF-kB activity results in inactivation of
caspases [66]. IL-10 blocks the glutamate mediated NF-kB DNA
binding activity in neuronal [67] and nonneuronal cells [68],
suggesting that IL-10 reduces or prevents the activity of caspase-3
and NF-kB activity. In neurons of the CA1 hippocampal region, it
has been shown that combined treatment with hypothermia and
IL-10 may induce neuronal survival [69], as well as in astrocytes, in
which IL-10 and IL-13 inhibit apoptosis through the stimulation of
�8
P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
phosphatidylinositol 3-kinase (PI3K) [70]. In microglial cells, IL-10
also serves as a survival factor by inducing STAT3 phosphorylation
while not enhancing proliferation [71].
IL-10 can significantly reduce vulnerability of neurons to CNS
ischemia and trauma [72,73]. For example, in vitro, in spinal cord
neurons, IL-10 induces a number of signaling cascades through
binding to its receptor thereby inducing NF-kB and transcription of
the anti-apoptotic Bcl-2 and Bcl-xL genes, while after exposure to
glutamate, it blocks cytochrome c release and caspase cleavage
[74,75]. Furthermore, these direct neuroprotective effects of IL-10
have been demonstrated in a retinal ganglion cell line [64],
oligodendroglial cells [23] and cerebellar granule cells [67].
Similarly, in vivo, IL-10 overexpression in the spinal cord using a
herpes simplex virus based vector resulted in increased neuronal
survival and improved motor function for up to 6 weeks after injury
[74]. Others showed that also a single dose of IL-10 given
intraperitoneally during the first period after SCI (considered as
the early inflammatory response) may be neuroprotective, by
attenuating TNF-a protein levels between 1 h and 1 day after SCI in
rats. This was also seen to induce an improvement in the hind limb
motor function for up to two months after SCI [16]. IL-10 is also able
to reduce TNF-a and IL-1 levels and improve the outcome after
traumatic brain injury [72]. However, while most studies show
neuroprotective effects of IL-10 after SCI, improved locomotor
recovery was found in some, but not all SCI rodents [16,74,76].
In summary, IL-10 is implicated in cell survival (CNS and PNS)
and may promote recovery after SCI.
4.3. Interleukin-13
IL-13 is a 10 kDa protein which mediates its effects via the IL-13
receptor, expressed on human B cells, basophils, eosinophils, mast
cells, endothelial cells, fibroblasts, monocytes, macrophages,
respiratory epithelial cells, and smooth muscle cells. Two types
of receptors exist, one being a heterodimer of IL-13Ra1 and IL-4Ra
which can bind to IL-4 as well, and a second type consisting of an
IL-13Ra2 chain [77].
Signal transduction via IL-4Ra is known to be responsible for
most of the functional characteristics of IL-4 and IL-13. Both
cytokines activate JAK/STAT signaling, and it is already known that
IL-4 and STAT6 are involved in promotion of axonal regeneration
[25]. It is therefore probable that IL-13 and STAT6 may also
contribute to axonal regeneration. In addition, administration of
recombinant IL-13 leads to the enhancement of macrophage
development and function [41] which in turn can modulate
production of pro-inflammatory cytokines such as IL-6, TNFa, IL12 and the ‘‘anti-inflammatory’’ cytokine IL-10 [78]. This cytokine is
also capable of modulating the inflammatory response by suppressing the production of inflammatory mediators such as IL-1b, TNF-a
and IL-6 from microglia in vitro and in vivo [39,40]. Among these
cytokines, IL-10 and TNF-a have been implicated in axonal
regeneration in both a beneficial and detrimental way [16,76].
In the CNS, IL-13 mRNA levels are upregulated within hours
after CNS trauma (our own unpublished data). The effect of IL-13
on neuronal survival is not clear and both positive [79–81] and
negative effects [82] have been reported. In the brain, neurons and
microglia act cooperatively to downregulate brain inflammation
by inducing IL-13 expression in microglia and enhancing COX-2
expression [80] which has been previously associated with
cytotoxicity in brain diseases [83], thereby causing death of
activated microglia and leading to an increase in neuronal survival
[79,81]. Using thrombin to activate microglia leads to an
upregulation of IL-13 and ROS levels, resulting in a decrease in
neuronal survival. On the other hand, the blockade of IL-13 reduces
inflammatory cytokine expression, thus increasing neuronal
survival in the hippocampus in vivo [82]. One possible reason
given by the authors may be that thrombin and LPS activate
distinct signaling pathways when inducing microglia activation
and IL-13 may influence differentially these distinct pathways. It
has also been shown that IL-13 (in a dose dependent manner) can
influence the morphology of macrophage colonies, B cells and
monocytes; cells growing in the absence of IL-13 first showed a
large round morphology whereas cells cultured in its presence,
were more flattened and formed extensive processes and cellular
aggregates [84], acting as cells in the late stage of macrophage
colony formation. Similarly, it has been shown that IL-13 can
modulate 3 stages of the B cell maturation process: early activation
phase, proliferation and differentiation [85] while others showed
that in human monocytes, IL-13 can modulate the development of
long processes and alter survival [86]. In the CNS, activated
microglia or macrophages seem to create a favorable environment
for regeneration by degrading inhibitory molecules which prevent
axonal growth and reactive neurite sprouting [87]. It is possible
that modulating this microglial response after CNS injury by
factors such as IL-13, could be helpful to either prevent or degrade
depositions of these regeneration-inhibiting factors.
In summary, IL-13 has been implicated in cellular survival, with
both detrimental and beneficial effects reported. However, no
studies have been performed yet to investigate any direct effect of
this cytokine on axonal regeneration.
4.4. Leukemia inhibitory factor
LIF belongs to the IL-6 cytokine family, which transduce their
signals through the gp130 subunit and the low affinity LIF receptor
(LIFR). It has hematopoietic, neuronal and endocrine functions [88].
LIF is transported retrogradely by sensory and sympathetic
neurons; this transport is increased after nerve lesions [89,90]. LIF
is absent from the adult mammalian nervous system but it is
upregulated after injury to the sciatic nerve [90]. This upregulation
seems to enhance the regeneration of the transected sciatic nerve
by improving the conduction velocity of the regenerated nerve and
the number of myelinated fibers [91]. In addition, LIF also inhibits
the transport of ciliary neurotrophic factor (CNTF) in lesioned
sciatic nerve [92].
LIF is also involved in cell viability and supporting survival of
sensory neurons [93], possibly via direct mechanisms, since LIF
binds specifically to DRG neurons in vitro [89]. Moreover it can also
promote survival of sensory and motor neurons after axotomy in
vivo [91]. However in vitro studies have shown that LIF has no
effect on neurite outgrowth in DRG cells, either alone or in
combination with NGF; moreover, LIF initiates arborization of
sensory neurons [94].
After CNS injury, such as SCI and cortical lesioning, there is also
an increase of LIF mRNA levels (Fig. 1). In contrast, mRNA levels of
the LIFR decrease slightly after cortical injury. Using in situ
hybridization, it was possible to identity that LIF is mainly
expressed by astrocytes and to some extent also by microglia cells
after cortical injury and SCI [17]. This upregulation seems to have a
positive effect after SCI. Fibroblasts genetically modified to
produce LIF were embedded in a collagen matrix and grafted to
the lesioned spinal cord, promoting corticospinal axon growth and
resulting in an increase of NT-3 [95]. These findings support the
hypothesis that ‘‘anti-inflammatory’’ factors not only directly
mediate regeneration, but can also indirectly regulate the nervous
system response to injury by increasing the production of trophic
factors via the cytokine/neurotrophin axis [45]. Using LIF knockout mice, it was shown that LIF plays an important role in the initial
infiltration of inflammatory cells after cortical and sciatic nerve
injury, acting as a chemotactic factor for macrophages and
activation of microglia and astrocytes [96]. In hippocampal
neurons, LIF induces activation of signaling pathways associated
�P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
with neuroprotection and regeneration, increasing STAT3 levels
and phosphorylation of Akt473. However, it has no effect on
dendrite morphology and outgrowth, compared to other hematopoietic cytokines, such as erythropoietin [97]. In summary, LIF
increases regeneration after PNS and CNS injury (directly or
indirectly) and modulates cell survival.
4.5. Transforming growth factor-b
TGF-b is synthesized as an inactive precursor with three
isoforms: TGF-b1, b2 and b3. The active molecule is a 25 kDa
protein which is constitutively expressed in many cell types, such
as platelets, monocytes and T cells. It is mainly involved in
inhibition of monocytes/macrophages and pro-inflammatory
cytokine synthesis [9]. We will focus more on the effects of
TGF-b1, since this ‘‘anti-inflammatory’’ factor has been studied in a
greater depth than the other isoforms.
In the PNS, TGF-b1 has different effects depending of the
cellular target. Using DRG explants in three-dimensional cultures
of astrocytes, TGF-b was found to promote neurite outgrowth.
However, when these explants were treated with IL-1a or b, TGF-b
neutralized the outgrowth promoted by IL-1a or IL-1b [29]. In
Schwann cells, secreted protein acidic and rich in cysteine (SPARC),
a matricellular protein, mediates outgrowth via TGF-b and
laminin-1 mechanisms [98].
The addition of TGF-b1 to pre-treated astrocyte cultures has no
effect on cellular migration, but suppresses the migrationpromoting action of IL-1 and basic fibroblast growth factor (bFGF)
on primary oligodendrocyte precursors and astrocytes [29]. TGFb1 also suppresses the proliferation of astrocytes [99] and inhibits
neurite outgrowth via activation of RhoA/Rho kinase signaling in
cortical neurons in vitro [100].
As for the other ‘‘anti-inflammatory’’ factors mentioned
previously, TGF-b levels are increased after SCI, but later than
the other factors (Fig. 1), and also after brain injury, specifically
TGF-b1 [99].
TGF-b was also seen to be involved in glial scar formation. For
example, after brain injury TGF-b, via TGF-b receptor/Smad
signaling, induces an increase in the expression of neurocan, one of
the inhibitory molecules which mediates glial scar formation in
astrocytes [101]. Similarly, fibrinogen, a growth inhibitory factor
known to be involved in the glial scar formation, acts as a carrier of
latent TGF-b to the injury sites, facilitating the interaction of TGF-b
with astrocytes and the subsequent activation of TGF-b [102].
Thus, TGF-b is known to enhance the production of abundant
factors after CNS injury, which may limit spontaneous axon
regeneration and mediate neuronal survival after axonal injury
[103]. Nevertheless, treatment with TGF-b1 and b2 antibodies in a
unilateral nigrostriatal transection model, leads to a reduction of
astrocyte response and reduction of gliosis. However, this
combination did not enhance the regeneration of dopaminergic
axons [104]. Similar results were obtained after SCI, where
treatment with TGF-b1 neutralizing antibodies after injury lead
to an enhancement of locomotor skills and reduction of glial scar
formation. However, this improvement did not lead to an increase
in outgrowth of the corticospinal tract fibers, but presumably may
be responsible for restoring the injured serotonergic fibers [100].
Finally, in vitro, TGF-b1 enhances proliferation and the
formation of clusters using a meningeal fibroblast and astrocyte
in vitro model of the scar. The cellular clusters of extracellular
matrix molecules and axonal growth inhibitory factors accumulate
similarly to that in the glial scar following CNS injury. In clusters of
cerebellar neurons, neurite extension is inhibited in the presence
of TGF-b1 on flat meningeal fibroblasts [105].
In summary, TGF-b may either promote or inhibit neurite
outgrowth and may modulate cellular proliferation and migration.
9
5. Concluding remarks
Many ‘‘anti-inflammatory’’ factors are down- or upregulated
after CNS and PNS injury, either immediately or at a later stage.
Their expression at one particular time point after injury appears to
be crucial in defining whether or not regeneration is going to take
place.
Most of the ‘‘anti-inflammatory’’ factors reviewed here
participate in the regulation of cell survival, proliferation and
migration (IL-4, IL-10, IL-13, LIF and TGF-b), promoting in this way
regeneration after injury. Others have a more direct effect on
neurite regeneration (IL-4, LIF and TGF-b). The understanding in
vitro and also in vivo of how cytokines interact with other cytokines
as well as with the injured environment could bring to light their
role after injury. Such information would also help in determining
the most effective ways to utilize their properties in order to
stimulate and enhance regeneration. Today the number of new
therapies involving a combination of different molecules, all
aiming to promote axonal regeneration, has increased considerably. Thus, the modulation of the inflammatory phases, possibly
through cytokine modulation, could play a key role in regenerative
therapies.
In conclusion, the therapeutic use of the cytokines discussed
here is still extremely limited due to their phase-specific and
compartment-specific effects. Instructive ‘‘interactomics’’ models
are still a major necessity to develop complex neuro-immunomodulatory therapies.
References
[1] Goldsby R, Kindt R, Psborne B. Kuby Immunology 2000.
[2] Sholl-Franco A, da Silva AG, Adao-Novaes J. Interleukin-4 as a neuromodulatory cytokine: roles and signaling in the nervous system. Annals of the New
York Academy of Sciences 2009;1153:65–75.
[3] Besser M, Wank R. Cutting edge: clonally restricted production of the neurotrophins brain-derived neurotrophic factor and neurotrophin-3 mRNA by
human immune cells and Th1/Th2-polarized expression of their receptors.
Journal of Immunology 1999;162:6303–6.
[4] Kelly-Welch AE, Hanson EM, Boothby MR, Keegan AD. Interleukin-4 and
interleukin-13 signaling connections maps. Science 2003;300:1527–8.
[5] Gilman A, Goodman L, Hardman J, Limbird L. Goodman & Gilman’s the
Pharmacological Basis of Therapeutics 2001.
[6] Hendrix S, Nitsch R. The role of T helper cells in neuroprotection and
regeneration. Journal of Neuroimmunology 2007;184:100–12.
[7] Bethea JR, Castro M, Keane RW, Lee TT, Dietrich WD, Yezierski RP. Traumatic
spinal cord injury induces nuclear factor-kappaB activation. Journal of Neuroscience 1998;18:3251–60.
[8] Maini RN, Taylor PC. Anti-cytokine therapy for rheumatoid arthritis. Annual
Review of Medicine 2000;51:207–29.
[9] Opal SM, DePalo VA. Anti-inflammatory cytokines. Chest 2000;117:1162–72.
[10] Matzinger P. Friendly and dangerous signals: is the tissue in control? Nature
Immunology 2007;8:11–3.
[11] Yiu G, He Z. Glial inhibition of CNS axon regeneration. Nature Reviews
Neuroscience 2006;7:617–27.
[12] Tom VJ, Steinmetz MP, Miller JH, Doller CM, Silver J. Studies on the development and behavior of the dystrophic growth cone, the hallmark of regeneration failure, in an in vitro model of the glial scar and after spinal cord injury.
Journal of Neuroscience 2004;24:6531–9.
[13] Ming GL, Wong ST, Henley J, Yuan XV, Song HJ, Spitzer NC, Poo MM. Adaptation
in the chemotactic guidance of nerve growth cones. Nature 2002;417:411–8.
[14] Moalem G, Monsonego A, Shani Y, Cohen IR, Schwartz M. Differential T cell
response in central and peripheral nerve injury: connection with immune
privilege. FASEB Journal 1999;13:1207–17.
[15] Donnelly DJ, Popovich PG. Inflammation and its role in neuroprotection,
axonal regeneration and functional recovery after spinal cord injury. Experimental Neurology 2008;209:378–88.
[16] Bethea JR, Nagasima H, Acosta MC, Briceno C, Gomez F, Marcillo AE, Loor K,
Green J, Dietrich WD. Systemically administered interleukin-10 reduces
tumor necrosis factor-alpha production and significantly improves functional recovery following traumatic spinal cord injury in rats. Journal of Neurotrauma 1999;16:851–63.
[17] Pineau I, Lacroix S. Proinflammatory cytokine synthesis in the injured mouse
spinal cord: multiphasic expression pattern and identification of the cell
types involved. Journal of Comparative Neurology 2007;500:267–85.
[18] Schwab JM, Brechtel K, Mueller CA, Failli V, Kraps HP, Tuli SK, Schluesener HJ.
Experimental strategies to promote spinal cord regeneration—an integrative
perspective. Progress in Neurobiology 2006;78:91–116.
�10
P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
[19] Beck KD, Nguyen HX, Galvan MD, Salazar DL, Woodruff TM, Anderson AJ.
Quantitative analysis of cellular inflammation after traumatic spinal cord
injury: evidence for a multiphasic inflammatory response in the acute to
chronic environment. Brain 2010;133:433–47.
[20] Ankeny DP, Lucin KM, Sanders VM, McGaughy VM, Popovich PG. Spinal cord
injury triggers systemic autoimmunity: evidence for chronic B lymphocyte
activation and lupus-like autoantibody synthesis. Journal of Neurochemistry
2006;99:1073–87.
[21] Bonilla IE, Tanabe K, Strittmatter SM. Small proline-rich repeat protein 1A is
expressed by axotomized neurons and promotes axonal outgrowth. Journal
of Neuroscience 2002;22:1303–15.
[22] Schwab JM, Failli V, Chedotal A. Injury-related dynamic myelin/oligodendrocyte axon-outgrowth inhibition in the central nervous system. Lancet
2005;365:2055–7.
[23] Molina-Holgado E, Vela JM, Arevalo-Martin A, Guaza C. LPS/IFN-gamma
cytotoxicity in oligodendroglial cells: role of nitric oxide and protection by
the anti-inflammatory cytokine IL-10. European Journal of Neuroscience
2001;13:493–502.
[24] Wolf SA, Fisher J, Bechmann I, Steiner B, Kwidzinski E, Nitsch R. Neuroprotection by T-cells depends on their subtype and activation state. Journal of
Neuroimmunology 2002;133:72–80.
[25] Deboy CA, Xin J, Byram SC, Serpe CJ, Sanders VM, Jones KJ. Immune-mediated
neuroprotection of axotomized mouse facial motoneurons is dependent on
the IL-4/STAT6 signaling pathway in CD4(+) T cells. Experimental Neurology
2006;201:212–24.
[26] Koeberle PD, Gauldie J, Ball AK. Effects of adenoviral-mediated gene transfer of
interleukin-10, interleukin-4, and transforming growth factor-beta on the
survival of axotomized retinal ganglion cells. Neuroscience 2004;125:903–20.
[27] Araujo DM, Cotman CW. Trophic effects of interleukin-4-7 and -8 on hippocampal neuronal cultures: potential involvement of glial-derived factors.
Brain Research 1993;600:49–55.
[28] Araujo DM, Cotman CW. Differential effects of interleukin-1 beta and interleukin-2 on glia and hippocampal neurons in culture. International Journal of
Developmental Neuroscience 1995;13:201–12.
[29] Fok-Seang J, DiProspero NA, Meiners S, Muir E, Fawcett JW. Cytokine-induced
changes in the ability of astrocytes to support migration of oligodendrocyte
precursors and axon growth. European Journal of Neuroscience
1998;10:2400–15.
[30] Dhabhar FS. Enhancing versus suppressive effects of stress on immune
function: implications for immunoprotection and immunopathology. Neuroimmunomodulation 2009;16:300–17.
[31] Sempowski GD, Beckmann MP, Derdak S, Phipps RP. Subsets of murine lung
fibroblasts express membrane-bound and soluble IL-4 receptors, role of IL-4
in enhancing fibroblast proliferation and collagen synthesis. Journal of Immunology 1994;152:3606–14.
[32] Toi M, Bicknell R, Harris AL. Inhibition of colon and breast carcinoma cell
growth by interleukin-4. Cancer Research 1992;52:275–9.
[33] Obiri NI, Puri RK. Characterization of interleukin-4 receptors expressed on
human renal cell carcinoma cells. Oncology Research 1994;6:419–27.
[34] Yang G, Li L, Volk A, Emmell E, Petley T, Giles-Komar J, Rafferty P. Therapeutic
dosing with anti-interleukin-13 monoclonal antibody inhibits asthma progression in mice. Journal of Pharmacology and Experimental Therapeutics
2005;313:8–15.
[35] Hahn C, Teufel M, Herz U, Renz H, Erb KJ, Wohlleben G, Bröcker EB, Duschl A,
Sebald W, Grunewald SM. Inhibition of the IL-4/IL-13 receptor system prevents allergic sensitization without affecting established allergy in a mouse
model for allergic asthma. Journal of Allergy and Clinical Immunology
2003;111:1361–9.
[36] Cua DJ, Groux H, Hinton DR, Stohlman SA, Coffman RL. Transgenic interleukin
10 prevents induction of experimental autoimmune encephalomyelitis.
Journal of Experimental Medicine 1999;189:1005–10.
[37] Lu L, Saulis AS, Liu WR, Roy NK, Chao JD, Ledbetter S, Mustoe TA. The temporal
effects of anti-TGF-beta1 2, and 3 monoclonal antibody on wound healing
and hypertrophic scar formation. Journal of the American College of Surgeons
2005;201:391–7.
[38] Cai LQ, Cao YJ, Duan EK. Effects of leukaemia inhibitory factor on embryo
implantation in the mouse. Cytokine 2000;12:1676–82.
[39] Paludan SR, Lovmand J, Ellermann-Eriksen S, Mogensen SC. Effect of IL-4 and IL13 on IFN-gamma-induced production of nitric oxide in mouse macrophages
infected with herpes simplex virus type 2. FEBS Letters 1997;414:61–4.
[40] Szczepanik AM, Funes S, Petko W, Ringheim GE. IL-4, IL-10 and IL-13 modulate
A beta(1–42)-induced cytokine and chemokine production in primary murine
microglia and a human monocyte cell line. Neuroimmunol 2001;113:49–62.
[41] Cash E, Minty A, Ferrara P, Caput D, Fradelizi D, Rott O. Macrophage-inactivating IL-13 suppresses experimental autoimmune encephalomyelitis in
rats. Journal of Immunology 1994;153:4258–67.
[42] Wang C, Gold BG, Kaler LJ, Yu X, Afentoulis ME, Burrows GG, Vandenbark AA,
Bourdette DN, Offner H. Antigen-specific therapy promotes repair of myelin
and axonal damage in established EAE. Neurochem 2006;98:1817–27.
[43] Sicotte M, Tsatas O, Jeong SY, Cai CQ, He Z, David S. Immunization with myelin
or recombinant Nogo-66/MAG in alum promotes axon regeneration and
sprouting after corticospinal tract lesions in the spinal cord. Molecular
and Cellular Neurosciences 2003;23:251–63.
[44] Gimsa U, Wolf SA, Haas D, Bechmann I, Nitsch R. Th2 cells support intrinsic
anti-inflammatory properties of the brain. Journal of Neuroimmunology
2001;119:73–80.
[45] Golz G, Uhlmann L, Ludecke D, Markgraf N, Nitsch R, Hendrix S. The cytokine/
neurotrophin axis in peripheral axon outgrowth. European Journal of Neuroscience 2006;24:2721–30.
[46] Uceyler N, Tscharke A, Sommer C. Early cytokine expression in mouse sciatic
nerve after chronic constriction nerve injury depends on calpain. Brain
Behavior and Immunity 2007;21:553–60.
[47] Uceyler N, Tscharke A, Sommer C. Early cytokine gene expression in mouse
CNS after peripheral nerve lesion. Neuroscience Letters 2008;436:259–64.
[48] Sholl-Franco A, Figueiredo KG, de Araujo EG. Interleukin-2 and interleukin-4
increase the survival of retinal ganglion cells in culture. Neuroreport
2001;12:109–12.
[49] Toi M, Harris AL, Bicknell R. Interleukin-4 is a potent mitogen for capillary
endothelium. Biochemical and Biophysical Research Communications
1991;174:1287–93.
[50] Volpert OV, Fong T, Koch AE, Peterson JD, Waltenbaugh C, Tepper RI, Bouck
NP. Inhibition of angiogenesis by interleukin 4. Exp Med 1998;188:1039–46.
[51] Sekimoto M, Tsuji T, Matsuzaki J, Chamoto K, Koda T, Nemoto K, Degawa M,
Nishimura S, Nishimura T. Functional expression of the TrkC gene, encoding a
high affinity receptor for NT-3, in antigen-specific T helper type 2 (Th2) cells.
Immunology Letters 2003;88:221–6.
[52] Figurov A, Pozzo-Miller LD, Olafsson P, Wang T, Lu B. Regulation of synaptic
responses to high-frequency stimulation and LTP by neurotrophins in the
hippocampus. Nature 1996;381:706–9.
[53] Lee SI, Jeong SR, Kang YM, Han DH, Jin BK, Namgung U, Kim BG. Endogenous
expression of interleukin-4 regulates macrophage activation and confines
cavity formation after traumatic spinal cord injury. Journal of Neuroscience
Research 2010;88:2409–19.
[54] Adao-Novaes J, Guterres Cde C, da Silva AG, Campello-Costa P, Linden R, ShollFranco A. Interleukin-4 blocks thapsigargin-induced cell death in rat rod
photoreceptors: involvement of cAMP/PKA pathway. Journal of Neuroscience
Research 2009;87:2167–74.
[55] Sholl-Franco A, Marques PM, Ferreira CM, de Araujo EG. IL-4 increases
GABAergic phenotype in rat retinal cell cultures: involvement of muscarinic
receptors and protein kinase C. Journal of Neuroimmunology 2002;133:20–9.
[56] Sawada M, Suzumura A, Marunouchi T. Cytokine network in the central
nervous system and its roles in growth and differentiation of glial and
neuronal cells. International Journal of Developmental Neuroscience
1995;13:253–64.
[57] Chao CC, Molitor TW, Hu S. Neuroprotective role of IL-4 against activated
microglia. Journal of Immunology 1993;151:1473–81.
[58] Brodie C, Goldreich N, Haiman T, Kazimirsky G. Functional IL-4 receptors on
mouse astrocytes: IL-4 inhibits astrocyte activation and induces NGF secretion. Journal of Neuroimmunology 1998;81:20–30.
[59] Merril JE, Murphy SP, Mitrovic B, Mackenzie-Graham A, Dopp JC, Griscavage J,
Ognarro LJ, Lowenstein CJ. Inducible nitric oxide synthase and nitric oxide
production by oligodendrocytes. Journal of Neuroscience Research
1997;48:372–84.
[60] Butovsky O, Ziv Y, Schwartz A, Landa G, Talpalar AE, Pluchino S, Marino G,
Schwartz M. Microglia activated by IL-4 or IFN-gamma differentially induce
neurogenesis and oligodendrogenesis from adult stem/progenitor cells. Molecular and Cellular Neurosciences 2006;31:149–60.
[61] Xin J, Wainwright DA, Serpe CJ, Sanders VM, Jones KJ. Phenotype of CD4+ T
cell subsets that develop following mouse facial nerve axotomy. Brain
Behavior and Immunity 2008;22:528–37.
[62] Xin J, Wainwright DA, Mesnard NA, Serpe CJ, Sanders VM, Jones KJ. IL-10
within the CNS is necessary for CD4+ T cells to mediate neuroprotection.
Brain Behavior and Immunity 2011;25:820–9.
[63] Atkins S, Loescher AR, Boissonade FM, Smith KG, Occleston N, O’Kane S,
Ferguson MW, Robinson PP. Interleukin-10 reduces scarring and enhances
regeneration at a site of sciatic nerve repair. Journal of the Peripheral Nervous
System 2007;12:269–76.
[64] Boyd ZS, Kriatchko A, Yang J, Agarwal N, Wax MB, Patil RV. Interleukin-10
receptor signaling through STAT-3 regulates the apoptosis of retinal ganglion
cells in response to stress. Investigative Ophthalmology and Visual Science
2003;44:5206–11.
[65] Kaltschmidt C, Kaltschmidt B, Baeuerle PA. Stimulation of ionotropic glutamate receptors activates transcription factor NF-kappa B in primary neurons.
Proceedings of the National Academy of Sciences of the United States of
America 1995;92:9618–22.
[66] Gill JS, Windebank AJ. Ceramide initiates NFkappaB-mediated caspase activation in neuronal apoptosis. Neurobiology of Disease 2000;7:448–61.
[67] Bachis A, Colangelo AM, Vicini S, Doe PP, De Bernardi MA, Brooker G,
MOcchetti I. Interleukin-10 prevents glutamate-mediated cerebellar granule
cell death by blocking caspase-3-like activity. Journal of Neuroscience
2001;21:3104–12.
[68] Schottelius AJ, Mayo MW, Sartor RB, Baldwin Jr AS. Interleukin-10 signaling
blocks inhibitor of kappaB kinase activity and nuclear factor kappaB DNA
binding. Journal of Biological Chemistry 1999;274:31868–74.
[69] Dietrich WD, Busto R, Bethea JR. Postischemic hypothermia and IL-10
treatment provide long-lasting neuroprotection of CA1 hippocampus
following transient global ischemia in rats. Experimental Neurology
1999;158:444–50.
[70] Pahan K, Khan M, Singh I. Interleukin-10 and interleukin-13 inhibit proinflammatory cytokine-induced ceramide production through the activation
of phosphatidylinositol 3-kinase. Journal of Neurochemistry 2000;75:
576–82.
�P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
[71] Strle K, Zhou JH, Broussard SR, Venters HD, Johnson RW, Freund GG, Dantzer
R, Kelley KW. IL-10 promotes survival of microglia without activating Akt.
Journal of Neuroimmunology 2002;122:9–19.
[72] Knoblach SM, Faden AI. Interleukin-10 improves outcome and alters proinflammatory cytokine expression after experimental traumatic brain injury.
Experimental Neurology 1998;153:143–51.
[73] Grilli M, Barbieri I, Basudev H, Brusa R, Casati C, Lozza G, Ongini E. Interleukin-10 modulates neuronal threshold of vulnerability to ischaemic damage.
European Journal of Neuroscience 2000;12:2265–72.
[74] Zhou Z, Peng X, Insolera R, Fink DJ, Mata M. IL-10 promotes neuronal survival
following spinal cord injury. Experimental Neurology 2009;220:183–90.
[75] Zhou Z, Peng X, Insolera R, Fink DJ, Mata M. Interleukin-10 provides direct
trophic support to neurons. Journal of Neurochemistry 2009;110:1617–27.
[76] Takami T, Oudega M, Bethea JR, Wood PM, Kleitman N, Bunge MB. Methylprednisolone and interleukin-10 reduce gray matter damage in the contused
Fischer rat thoracic spinal cord but do not improve functional outcome.
Journal of Neurotrauma 2002;19:653–66.
[77] Hershey GK. IL-13 receptors and signaling pathways: an evolving web.
Journal of Allergy and Clinical Immunology 2003;111:677–90. quiz 691.
[78] Doherty TM, Kastelein R, Menon S, Andrade S, Coffman RL. Modulation of
murine macrophage function by IL-13. Journal of Immunology 1993;151:
7151–60.
[79] Shin WH, Lee DY, Park KW, Kim SU, Yang MS, Joe EH, Jin BK. Microglia
expressing interleukin-13 undergo cell death and contribute to neuronal
survival in vivo. Glia 2004;46:142–52.
[80] Yang MS, Ji KA, Jeon SB, Jin BK, Kim SU, Jou I, Joe E. Interleukin-13 enhances
cyclooxygenase-2 expression in activated rat brain microglia: implications
for death of activated microglia. Journal of Immunology 2006;177:1323–9.
[81] Yang MS, Park EJ, Sohn S, Kwon HJ, Shin WH, Pyo HK, Jin B, Choi KS, Jou I, Joe
EH. Interleukin-13 and -4 induce death of activated microglia. Glia 2002;38:
273–80.
[82] Park KW, Baik HH, Jin BK. IL-13-induced oxidative stress via microglial
NADPH oxidase contributes to death of hippocampal neurons in vivo. Journal
of Immunology 2009;183:4666–74.
[83] Iadecola C, Niwa K, Nogowa S, Zhao X, Nagayama M, Araki E, Mortham S, Ross
ME. Reduced susceptibility to ischemic brain injury and N-methyl-D-aspartate-mediated neurotoxicity in cyclooxygenase-2-deficient mice. Proceedings of the National Academy of Sciences of the United States of America
2001;98:1294–9.
[84] Sakamoto O, Hashiyama M, Minty A, Ando M, Suda T. Interleukin-13 selectively suppresses the growth of human macrophage progenitors at the late
stage. Blood 1995;85:3487–93.
[85] Defrance T, Carayon P, Billian G, Guillemot JC, Minty A, Caput D, Ferrara P.
Interleukin 13 is a B cell stimulating factor. Journal of Experimental Medicine
1994;179:135–43.
[86] Zurawski G, de Vries JE. Interleukin 13 elicits a subset of the activities of its
close relative interleukin 4. Stem Cells 1994;12:169–74.
[87] Avellino AM, Hart D, Dailey AT, MacKinnon M, Ellegala D, Kliot M. Differential
macrophage responses in the peripheral and central nervous system during
wallerian degeneration of axons. Experimental Neurology 1995;136:183–98.
[88] Slaets H, Hendriks JJ, Stinissen P, Kilpatrick TJ, Hellings N. Therapeutic
potential of LIF in multiple sclerosis. Trends in Molecular Medicine
2010;16:493–500.
[89] Hendry IA, Murphy M, Hilton DJ, Nicola NA, Bartlett PF. Binding and retrograde transport of leukemia inhibitory factor by the sensory nervous system.
Journal of Neuroscience 1992;12:3427–34.
[90] Curtis R, Scherer SS, Somogyi R, Adryan KM, Ip NY, Zhu Y, Lindsay RM,
SiStefano PS. Retrograde axonal transport of LIF is increased by peripheral
nerve injury: correlation with increased LIF expression in distal nerve.
Neuron 1994;12:191–204.
[91] Tham S, Dowsing B, Finkelstein D, Donato R, Cheema SS, Bartlett PF, Morrison
WA. Leukemia inhibitory factor enhances the regeneration of transected rat
sciatic nerve and the function of reinnervated muscle. Journal of Neuroscience Research 1997;47:208–15.
[92] Curtis R, Adryan KM, Zhu Y, Harkness PJ, Lindsay RM, DiStefano PS. Retrograde axonal transport of ciliary neurotrophic factor is increased by peripheral nerve injury. Nature 1993;365:253–5.
[93] Murphy M, Reid K, Hilton DJ, Bartlett PF. Generation of sensory neurons is
stimulated by leukemia inhibitory factor. Proceedings of the National Academy of Sciences of the United States of America 1991;88:3498–501.
[94] Cafferty WB, Gardiner NJ, Gavazzi I, Powell J, McMahon SB, Health JK, Munson
J, Cohen J, Thompson SW. Leukemia inhibitory factor determines the growth
status of injured adult sensory neurons. Journal of Neuroscience 2001;21:
7161–70.
[95] Blesch A, Uy HS, Grill RJ, Cheng JG, Patterson PH, Tuszynski MH.
Leukemia inhibitory factor augments neurotrophin expression and corticospinal axon growth after adult CNS injury. Journal of Neuroscience
1999;19:3556–66.
[96] Sugiura S, Lahav R, Han J, Kou SY, Banner LR, de Pablo F, Patterson PH.
Leukaemia inhibitory factor is required for normal inflammatory responses
to injury in the peripheral and central nervous systems in vivo and is
chemotactic for macrophages in vitro. European Journal of Neuroscience
2000;12:457–66.
[97] Ransome MI, Turnley AM. Erythropoietin promotes axonal growth in a model
of neuronal polarization. Molecular and Cellular Neurosciences 2008;38:
537–47.
11
[98] Au E, Richter MW, Vincent AJ, Tetzlaff W, Aebersold R, Sage EH, Roskams AJ.
SPARC from olfactory ensheathing cells stimulates Schwann cells to promote
neurite outgrowth and enhances spinal cord repair. Journal of Neuroscience
2007;27:7208–21.
[99] Lindholm D, Castren E, Kiefer R, Zafra F, Thoenen H. Transforming growth
factor-beta 1 in the rat brain: increase after injury and inhibition of astrocyte
proliferation. Journal of Cell Biology 1992;117:395–400.
[100] Kohta M, Kohmura E, Yamashita T. Inhibition of TGF-beta1 promotes functional recovery after spinal cord injury. Neuroscience Research 2009;65:
393–401.
[101] Asher RA, Morgenstern DA, Fidler PS, Adcock KH, Oohira A, Braistead JE,
Levine JM, Margolis RU, ROgers JH, Fawcett JW. Neurocan is upregulated in
injured brain and in cytokine-treated astrocytes. Journal of Neuroscience
2000;20:2427–38.
[102] Schachtrup C, Ryu JK, Helmrick MJ, Vagena E, Galanakis DK, Degen JL,
Margolis RU, Akassoglou K. Fibrinogen triggers astrocyte scar formation
by promoting the availability of active TGF-beta after vascular damage.
Journal of Neuroscience 2010;30:5843–54.
[103] Makwana M, Jones LL, Cuthill D, Heuer H, Bohatschek M, Hristove M,
Friedrichsen S, Ormsby I, Bueringer D, Koppius A, Bauer K, Doetschmann
T, Raivich G. Endogenous transforming growth factor beta 1 suppresses
inflammation and promotes survival in adult CNS. Journal of Neuroscience
2007;27:11201–13.
[104] Moon LD, Fawcett JW. Reduction in CNS scar formation without concomitant
increase in axon regeneration following treatment of adult rat brain with a
combination of antibodies to TGFbeta1 and beta2. European Journal of
Neuroscience 2001;14:1667–77.
[105] Kimura-Kuroda J, Teng X, Komuta Y, Yoshioka N, Sango K, Kawamura K,
Raisman G, Kawano H. An in vitro model of the inhibition of axon growth in
the lesion scar formed after central nervous system injury. Molecular and
Cellular Neurosciences 2010;43:177–87.
[106] McTigue DM, Popovich PG, Morgan TE, Stokes BT. Localization of transforming growth factor-beta1 and receptor mRNA after experimental spinal cord
injury. Experimental Neurology 2000;163:220–30.
[107] Jones TB, Basso DM, Sodhi A, Pan JZ, Hart RP, MasCallum RC, Lee S, Whitacre
CC, Popovich PG. Pathological CNS autoimmune disease triggered by traumatic spinal cord injury: implications for autoimmune vaccine therapy.
Journal of Neuroscience 2002;22:2690–700.
[108] Rotshenker S. Wallerian degeneration: the innate-immune response to
traumatic nerve injury. J Neuroinflammation 2011;8:109.
[109] Aharoni R, Kayhan B, Eilam R, Sela M, Arnon R. Glatiramer acetate-specific T
cells in the brain express T helper 2/3 cytokines and brain-derived neurotrophic factor in situ. Proceedings of the National Academy of Sciences of the
United States of America 2003;100:14157–62.
[110] Noga O, peiser M, Althenähr M, Knieling H, Wanner R, Hanf G, Grosse R,
Suttorp N. Differential activation of dendritic cells by nerve growth facto
and brain-derived neurotrophic factor. Clinical and Experimental Allergy
2007;37:1701–8.
[111] Sin AZ, Roche EM, Togias A, Lichtenstein LM, Schroeder JT. Nerve growth
factor or IL-3 induces more IL-13 production from basophils of allergic
subjects than from basophils of nonallergic subjects. Journal of Allergy
and Clinical Immunology 2001;108:387–93.
[112] De Simone R, Ambrosini E, Carnevale D, Ajmone-Cat MA, Minghetti L. NGF
promotes microglial migration through the activation of its high affinity
receptor: modulation by TGF-beta. Journal of Neuroimmunology 2007;190:
53–60.
[113] Marzella PL, Clark GM, Shepherd RK, Bartlett PF, Kilpatrick TJ. Synergy
between TGF-beta 3 and NT-3 to promote the survival of spiral ganglia
neurones in vitro. Neuroscience Letters 1998;240:77–80.
[114] Marzella PL, Gillespie LN, Clark GM, Bartlett PF, Kilpatrick TJ. The neurotrophins act synergistically with LIF and members of the TGF-beta superfamily
to promote the survival of spiral ganglia neurons in vitro. Hearing Research
1999;138:73–80.
[115] Yelo E, Bernardo MV, Gimeno L, Alcaraz-Garcia MJ, Majado MJ, Parrado A.
Dock10, a novel CZH protein selectively induced by interleukin-4 in human B
lymphocytes. Molecular Immunology 2008;45:3411–8.
[116] Chiba Y, Nakazawa S, Todoroki M, Shinozaki K, Sakai H, Misawa M. Interleukin-13 augments bronchial smooth muscle contractility with an up-regulation of RhoA protein. American Journal of Respiratory Cell and Molecular
Biology 2009;40:159–67.
[117] Chen J, Guerriero E, Sado Y, SundarRaj N. Rho-mediated regulation of TGFbeta1- and FGF-2-induced activation of corneal stromal keratocytes. Investigative Ophthalmology and Visual Science 2009;50:3662–70.
[118] Lee J, Ko M, Joo CK. Rho plays a key role in TGF-beta1-induced cytoskeletal
rearrangement in human retinal pigment epithelium. Journal of Cellular
Physiology 2008;216:520–6.
[119] Xiao YQ, Freire-de-Lima CG, Schiemann WP, Bratton DL, Vandivier RW, Henson
PM. Transcriptional and translational regulation of TGF-beta production in
response to apoptotic cells. Journal of Immunology 2008;181:3575–85.
[120] Ethier MF, Cappelluti E, Madison JM. Mechanisms of interleukin-4 effects on
calcium signaling in airway smooth muscle cells. Journal of Pharmacology
and Experimental Therapeutics 2005;313:127–33.
[121] Martin G, O’Connell RJ, Pietrzykowski AZ, Treistman SN, Ethier MF, Madison
JM. Interleukin-4 activates large-conductance, calcium-activated potassium
(BKCa) channels in human airway smooth muscle cells. Experimental Physiology 2008;93:908–18.
�12
P.M. Vidal et al. / Cytokine & Growth Factor Reviews 24 (2013) 1–12
[122] Park-Min KH, Ji JD, Antoniv T, Reid AC, Silver RB, Humphrey MB, Nakamura M,
Ivashkiv LB. IL-10 suppresses calcium-mediated costimulation of receptor
activator NF-kappa B signaling during human osteoclast differentiation
by inhibiting TREM-2 expression. Journal of Immunology 2009;183:2444–
55.
[123] Miki K, Tanaka H, Nagai Y, Kimura C, Oike M. Transforming growth factor
beta1 alters calcium mobilizing properties and endogenous ATP release in
A549 cells: possible implications for cell migration. Journal of Pharmacological Sciences 2010;113:387–94.
[124] Faon M, Rebola M, Berger P, Daburon S, Ousova O, Labrand F, Moukaila B,
Pujol W, Taupin JL, Labbe A, Molimard M, Marthan R. Increased secretion of
leukemia inhibitory factor by immature airway smooth muscle cells
enhances intracellular signaling and airway contractility. American Journal
of Physiology Lung Cellular and Molecular Physiology 2006;291:L244–51.
[125] Dugas B, Paul-Eugene N, Yamaoka K, Amirand C, Damais C, Kolb JP. IL-4
induces cAMP and cGMP in human monocytic cells. Mediators of Inflammation 1995;4:298–305.
[126] Kambayashi T, Wallin RP, Ljunggren HG. cAMP-elevating agents suppress
dendritic cell function. Journal of Leukocyte Biology 2001;70:903–10.
[127] Wei LH, Jacobs AT, Morris Jr SM, Ignarro LJ. IL-4 and IL-13 upregulate arginase
I expression by cAMP and JAK/STAT6 pathways in vascular smooth muscle
cells. American Journal of Physiology Cell Physiology 2000;279:C248–56.
[128] Chang CI, Zoghi B, Liao JC, Kuo L. The involvement of tyrosine kinases,
cyclic AMP/protein kinase A, and p38 mitogen-activated protein kinase in
IL-13-mediated arginase I induction in macrophages: its implications in
IL-13-inhibited nitric oxide production. Journal of Immunology 2000;165:
2134–41.
[129] Son J, Lee JH, Kim HN, Ha H, Lee ZH. cAMP-response-element-binding protein
positively regulates breast cancer metastasis and subsequent bone destruction.
Biochemical and Biophysical Research Communications 2010;398:309–14.
[130] Howe K, Gauldie J, McKay DM. TGF-beta effects on epithelial ion transport
and barrier: reduced Cl- secretion blocked by a p38 MAPK inhibitor. American Journal of Physiology Cell Physiology 2002;283:C1667–74.
[131] Nesti LJ, Caterson EJ, Li WJ, Chang R, McCann TD, Hoek JB, Tuan RS. TGF-beta1
calcium signaling in osteoblasts. Journal of Cellular Biochemistry 2007;101:
348–59.
[132] Cai F, Campana WM, Tomlinson DR, Fernyhough P. Transforming growth
factor-beta1 and glial growth factor 2 reduce neurotrophin-3 mRNA expression in cultured Schwann cells via a cAMP-dependent pathway. Brain Research Molecular Brain Research 1999;71:256–64.
[133] Latijnhouwers MA, Pfundt R, de Jongh GJ, Schalkwijk J. Tenascin-C expression
in human epidermal keratinocytes is regulated by inflammatory cytokines
and a stress response pathway. Matrix Biology 1998;17:305–16.
[134] Jinnin M, Ihn H, Asano Y, Yamane K, Trojanowska M, Tamaki K. Upregulation
of tenascin-C expression by IL-13 in human dermal fibroblasts via the
phosphoinositide 3-kinase/Akt and the protein kinase C signaling pathways.
Journal of Investigative Dermatology 2006;126:551–60.
[135] White JD, Davies M, Grounds MD. Leukaemia inhibitory factor increases
myoblast replication and survival and affects extracellular matrix production: combined in vivo and in vitro studies in post-natal skeletal muscle. Cell
and Tissue Research 2001;306:129–41.
[136] Ishibashi T, Lee PR, Baba H, Fields RD. Leukemia inhibitory factor regulates
the timing of oligodendrocyte development and myelination in the postnatal
optic nerve. Journal of Neuroscience Research 2009;87:3343–55.
[137] Tadagavadi RK, Wang W, Ramesh G. Netrin-1 regulates Th1/Th2/Th17
cytokine production and inflammation through UNC5B receptor and
protects kidney against ischemia-reperfusion injury. Journal of Immunology
2010;185:3750–8.
[138] Mutz C, Mirakaj V, Vagts DA, Westermann P, Waibler K, König K, Iber T,
Nöldge-Schomburg G, Rosenberger P. The neuronal guidance protein netrin1 reduces alveolar inflammation in a porcine model of acute lung injury.
Critical Care 2010;14:R189.
[139] Kim JS, Kim JG, Moon MY, Jeon CY, Won HY, Kim HJ, Jeon YJ, Seo JY, Kim JI, Jim
J, Lee JY, Kim PH, Park JB. Transforming growth factor-beta1 regulates
macrophage migration via RhoA. Blood 2006;108:1821–9.
[140] He Y, Xu H, Liang L, Zhan Z, Yang X, Yu X, Ye Y, Sun L. Antiinflammatory effect
of Rho kinase blockade via inhibition of NF-kappaB activation in rheumatoid
arthritis. Arthritis and Rheumatism 2008;58:3366–76.
[141] Feske S, Giltnane J, Dolmetsch R, Staudt LM, Rao A. Gene regulation mediated
by calcium signals in T lymphocytes. Nature Immunology 2001;2:316–24.
[142] Zhang X, Wheeler D, Tang Guo L, Shapiro RA, Ribar TJ, Means AR, Billiar TR,
Angus DC, Rosengart MR. Calcium/calmodulin-dependent protein kinase
(CaMK) IV mediates nucleocytoplasmic shuttling and release of HMGB1
during lipopolysaccharide stimulation of macrophages. Journal of Immunology 2008;181:5015–23.
[143] Fisher TA, Palmetshofer A, Gambaryan S, Butt E, Jassoy C, Walter U, Sopper S,
Lohmann SM. Activation of cGMP-dependent protein kinase Ibeta inhibits
[144]
[145]
[146]
[147]
[148]
[149]
interleukin 2 release and proliferation of T cell receptor-stimulated human
peripheral T cells. Journal of Biological Chemistry 2001;276:5967–74.
Liu L, Das S, Losert W, Parent CA. mTORC2 regulates neutrophil chemotaxis in
a cAMP- and RhoA-dependent fashion. Developmental Cell 2010;19:845–57.
Cantarella G, Mepereur L, Presta M, Ribatti D, Lombardo G, Lazarovici P,
Zappala G, Pafumi C, Bernardini R. Nerve growth factor-endothelial cell
interaction leads to angiogenesis in vitro and in vivo. FASEB Journal
2002;16:1307–9.
Nassenstein C, Braun A, Erpenbeck VJ, Lommatzsch M, Schmidt S, Krug N,
Luttmann W, Renz H, Virchow Jr JC. The neurotrophins nerve growth factor,
brain-derived neurotrophic factor, neurotrophin-3, and neurotrophin-4 are
survival and activation factors for eosinophils in patients with allergic
bronchial asthma. Journal of Experimental Medicine 2003;198:455–67.
Huang JY, Cheng YJ, Lin YP, Lin HC, Su CC, Juliano R, Yang BC. Extracellular
matrix of glioblastoma inhibits polarization and transmigration of T cells: the
role of tenascin-C in immune suppression. Journal of Immunology 2010;185:
1450–9.
Garci-Nieto S, Johal RK, Shakesheff KM, Emara M, Royer PJ, Chau DY, Shakib F,
Ghaemmaghami AM. Laminin and fibronectin treatment leads to generation
of dendritic cells with superior endocytic capacity. PLoS One 2010;5:e10123.
Brewer KL, Bethea JR, Yezierski RP. Neuroprotective effects of interleukin-10
following excitotoxic spinal cord injury. Experimental Neurology 1999;159:
484–93.
Pı́a M. Vidal graduated in Bioengineering with specialization in Cellular and Molecular Biology at the University of Concepción, Chile. Currently she is a Ph.D. student
in the Dept. of Morphology at Hasselt University,
Belgium. Her research interests include the role of anti
and pro- inflammatory cytokines in spinal cord regeneration, as well as the effect/modulation of the immune
system in central nervous system diseases.
Evi Lemmens studied Biomedical Sciences at Hasselt
University, Belgium (1999–2003), and obtained her
Ph.D. at Maastricht University, the Netherlands, in
2008. During her doctoral studies, she investigated
the long-term effects of early-life febrile seizures on
brain development and behavioral outcome. She currently works at Hasselt University as a postdoctoral
fellow of the Flanders Research Foundation (FWO).
Her research focuses on neuro-immune interactions
to promote regeneration after nervous system trauma
such as spinal cord injury and traumatic brain injury.
Dearbhaile Dooley obtained her B.Sc. (Hons) from the
Discipline of Anatomy at the National University of
Ireland, Galway in 2010. She is currently a Ph.D. student
in the Dept. of Morphology at the Biomedical Research
Institute at Hasselt University, Belgium. Her research
focuses on the immunomodulatory role of stem cells in
spinal cord injury and how the combination of stem
cells with pro- and anti-inflammatory cytokines, alters
the surrounding microenvironment.
Sven Hendrix M.D. is a full professor for anatomy and
director of the Doctoral School for Medicine & Life
Sciences at Hasselt University, Belgium. He obtained
his M.D. degree at the Charité Berlin, Germany. His
research group studies neuroinflammation with a special focus on CNS trauma and axonal regeneration.
�
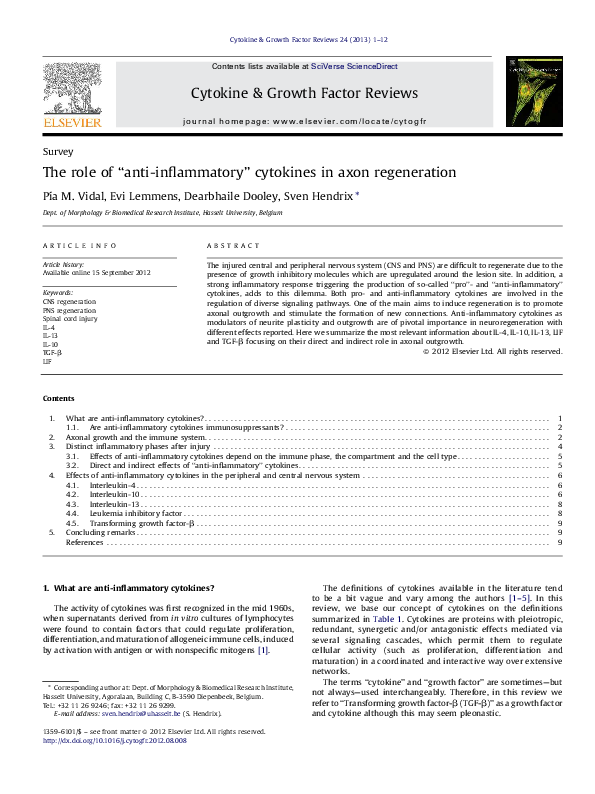
 Dearbhaile Dooley
Dearbhaile Dooley