Journal of Internal Medicine 2006; 259: 410–417
doi:10.1111/j.1365-2796.2006.01629.x
Rising incidence and persistently high mortality of
hospitalized pneumonia: a 10-year population-based study in
Denmark
R. W. THOMSEN1, A. RIIS1, M. NØRGAARD1, J. JACOBSEN1, S. CHRISTENSEN1,
C. J. MCDONALD2 & H. T. SØRENSEN1,3
From the 1Department of Clinical Epidemiology, Aarhus University Hospital, Aalborg and Aarhus, Denmark, 2The Regenstrief Institute and the
Indiana University School of Medicine, Indianapolis, IN, USA, and 3Department of Epidemiology, School of Public Health, Boston University, Boston,
MA, USA
Abstract. Thomsen RW, Riis A, Nørgaard M,
Jacobsen J, Christensen S, McDonald CJ, Sørensen
HT. Rising incidence and persistently high mortality
of hospitalized pneumonia: a 10-year populationbased study in Denmark. J Intern Med 2006; 259:
410–417.
Background. Little is known about temporal trends
in the incidence and mortality of pneumonia in the
general population.
Methods. We conducted a population-based cohort
study in three Danish counties (population 1.4
million) to examine changes in the incidence and
30- and 90-day mortality associated with
hospitalized pneumonia between 1994 and 2004.
All adults hospitalized with a first-time diagnosis of
pneumonia (n ¼ 41 793) were identified in hospital
discharge registries and followed for mortality
through the Danish Civil Registry System. We
determined age-standardized incidence rates and
adjusted mortality rates associated with calendar
year, gender, age and comorbidity.
Results. Between 1994 and 2003, the incidence
of hospitalized pneumonia amongst adults increased
Introduction
Pneumonia is an important cause of morbidity and
mortality and a heavy economic burden on
healthcare systems, primarily due to hospitalized
cases [1–3]. Some have suggested that the incidence
of pneumonia may rise in Western populations due
to the increased proportion of elderly persons with
410
from 288 per 100 000 person-years to 442
per 100 000 person-years, equivalent to an
age-standardized incidence rate ratio of 1.50. The
cumulative mortality within 30 and 90 days of
admission was 15.2% and 21.9%, respectively,
ranging from a 90-day mortality of 2.5% in patients
aged 15–39 years to 34.7% in those aged 80 and
over. Advanced age was the most important poor
prognostic factor, followed by a high comorbidity
score and male gender. The adjusted mortality rate
ratios amongst patients with hospitalized pneumonia
in 1999–2004, when compared with 1994–1998,
were 0.89 (95% CI 0.85–0.94) after 30 days and
0.91 (95% CI 0.88–0.95) after 90 days.
Conclusions. The incidence of hospitalized pneumonia in Denmark has increased considerably
during the last 10 years and, combined with
persistently high mortality rates, is of clinical and
public health concern.
Keywords: epidemiologic study, incidence, mortality, pneumonia.
multiple morbidities [4, 5]. However, there is little
population-based longitudinal data to evaluate temporal trends in the incidence and mortality of
pneumonia [6, 7]. Reported in-hospital mortality
rates of pneumonia average 5–15% and have
apparently remained at this level for decades [8].
Mortality increases with age and comorbidity and
probably male gender [9, 10], but population-based
� 2006 Blackwell Publishing Ltd
�HOSPITALIZED PNEUMONIA IN DENMARK
studies on the effect of these prognostic factors are
few [6]. We therefore conducted this populationbased study in three Danish counties to examine
changes in the incidence and 30- and 90-day
mortality associated with hospitalized pneumonia
amongst adults between 1994 and 2004 and to
assess the effect of age, gender and comorbidity on
pneumonia survival.
411
pneumonia, we removed hospitalizations for any
recurrent episode of pneumonia during 1994–2003
(n ¼ 19,874), and patients who were hospitalized
for pneumonia during 1989–1993 (ICD-8 codes
480.XX–486.XX, 0.73.XX and 471.XX) (n ¼
2,416). We finally removed paediatric patients
<15 years of age (n ¼ 7,642). This gave us a
population of unique adult patients with a first
episode of pneumonia for analysis.
Subjects and methods
Validation of discharge diagnoses of pneumonia
Study population and setting
The study was conducted in the three Danish
counties of North Jutland, Aarhus and Viborg,
within a homogeneous Caucasian, mixed rural and
urban population of 1.4 million inhabitants (26% of
the Danish population). The Danish healthcare
service provided tax-supported healthcare for all
county residents, guaranteeing free access to hospitals and primary medical care. General practitioners
(GPs)/family doctors acted as ‘gate keepers’ with
regard to hospital treatment and treatment by
specialists, and nearly all (97.6%) residents had
registered with a specific GP of their choice throughout the study period [11].
Because the Danish government assigns a unique
civil registry number to every Danish citizen, we
could link patients from our population-based registries and establish a complete hospitalization history
for each individual.
Identification of hospitalized pneumonia
We identified patients with a pneumonia associated
hospitalization by searching the discharge diagnoses codes stored within the ‘Aarhus University
Hospital Research Database’, which carries key
information for all patients discharged from any
hospital in the three counties since 1977 (in Viborg
County since 1972). Diagnoses are coded by
physicians according to the ‘International Classification of Diseases’, 8th revision (ICD-8) until the
end of 1993 and 10th revision (ICD-10) thereafter.
We first identified all discharges between 1 January
1994 and 31 December 2003 associated with
a diagnosis of pneumonia (ICD-10 codes
J12.x–J18.x), ornithosis (ICD-10 code A481.x), or
legionellosis (ICD-10 code A709.x) (n ¼ 71,725).
Because we were interested in the first episode of
To evaluate the diagnoses of pneumonia identified in
the database, we reviewed a random sample of 10 of
the selected hospital records for each of the 10 years
of the study period (1994 through 2003). We
confined the review to North Jutland County, as
data quality is considered uniform in the counties’
hospital discharge registries [12]. We confirmed the
discharge diagnosis of pneumonia when the
patient’s chest radiographic examination showed
an infiltrate, and at least one of the following clinical
or laboratory findings were present: body temperature ‡37.5 �C, cough, dyspnoea, chest pain or rales
coincident with the area of infiltrate, increased
sputum, purulent sputum, microorganism isolated
from blood culture, leucocyte count ‡12 · 109 L)1
or C-reactive protein >100 mg dL)1. We calculated
the predictive value of a pneumonia discharge
diagnosis as the percentage of episodes in the
reviewed hospital record sample that fulfilled our
criteria for confirmed pneumonia. We also assessed
the proportion of community-acquired pneumonia
episodes in the sample, i.e. episodes in which
pneumonia was present or incubating at the time
of hospital admission.
Data on comorbidity
To adjust for comorbidity, we computed the Charlson index score for each study subject on the basis of
the complete hospital discharge history before the
date of admission with pneumonia. The Charlson
index includes 19 major disease categories, and has
been adapted and validated for use with hospital
discharge data in ICD databases for the prediction of
short- and long-term mortality [13]. Three comorbidity index levels were defined, according to the
Charlson index score: score of 0, low; 1–2, medium;
3+, high. As alcohol abuse is not included in the
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 259: 410–417
�412
R . W . T H O M S E N et al.
Charlson index and may influence pneumonia
prognosis, we also collected data on previous alcohol-related disorders (‘yes’ or ‘no’) from the Discharge Registry (ICD-8 codes 291, 303, 979, 980,
577.10; ICD-10 codes F10, K86.0, Z72.1, R78.0,
T51).
Statistical analysis
Incidence. The annual incidence rates of pneumonia
were computed overall and within age- and genderspecific strata as the number of patients with a first
discharge diagnosis of pneumonia divided by the
number of citizens in the counties of North Jutland,
Aarhus, and Viborg in the middle of the year
(obtained from ‘Statistics Denmark’). Incidence rates
were standardized to the population of North
Jutland, Aarhus and Viborg County in 1994, using
1-year age groups.
Mortality. For the mortality analysis, we linked
patients with discharge diagnoses of pneumonia to
the Danish Civil Registry System, which keeps records of all changes in vital status and migration
and date of death for the entire Danish population.
The follow-up time was computed from the date of
hospital admission until death, migration, or
90 days after the admission date, which ever came
first. We used Cox regression analyses to compute
30- and 90-day mortality rate ratios (MRRs) with
95% CIs comparing the first and second half of the
study period (calendar year bands 1994–1998 and
1999–2003), gender (male/female), age group (15–
39, 40–64, 65–79, ‡80 years), and level of comorbidity (Charlson index score ¼ 0, 1–2, or 3+), whilst
adjusting for all the other factors. We verified the
assumption of proportional hazards in the Cox
model graphically. All statistical analyses were performed with sas software (version 9.1.3, SAS Institute Inc., Cary, NC, USA). The study was approved
by the Aarhus University Hospital Registry Board
and the Danish Data Protection Agency (record no.
2004-41-3854).
Results
We identified 41 793 persons older than 15 years
with a first time hospitalization with pneumonia.
The median age at hospitalization was 73.6 years,
and 53% of the individuals were male.
Validation of discharge diagnoses of pneumonia
In the reviewed sample of 100 episodes of hospitalized pneumonia, 90 episodes fulfilled criteria for
confirmed pneumonia, equivalent to a positive
predictive value of 90% (95% CI 82–95%). Of the
90 confirmed episodes, 78 (87%) were community
acquired.
Incidence
Between 1994 and 2003, the incidence of hospitalized pneumonia increased from 288 per 100 000
person-years to 442 per 100 000 person-years,
corresponding to an age-standardized incidence rate
ratio of 1.50. The incidence increased similarly
amongst young and old people over the decade, i.e.
the incidence increased by 66% in the 15- to 39year-old age group and by 58% in the ‡80-year-old
group. Overall, incidence rates were approximately
20% higher in men than in women throughout the
study period, yet amongst persons aged 65 years or
older, incidence rates in men were 50–100% higher
than in women (Fig. 1). The incidence of hospitalized pneumonia rose more than 30-fold with age, i.e.
from 84 per 100 000 in those aged 15–39 years to
2800 per 100 000 in those aged ‡80 years in
2003.
Between 1994 and 2003, the proportion of
hospitalizations in which pneumonia did not constitute the main diagnosis but rather a secondary
discharge diagnosis increased from 32% to 36%. The
median length of hospital stay for pneumonia
patients decreased from 8 days (interquartile range,
IQR 4–14) in 1994 to 7 days (IQR 3–12) in 2002.
Mortality
The overall cumulative mortality within 30 and
90 days of admission was 15.2% and 21.9%,
respectively. Mortality was higher in patients who
had pneumonia listed as a secondary discharge
diagnosis (20.3% after 30 days) compared with a
main diagnosis (12.6% after 30 days).
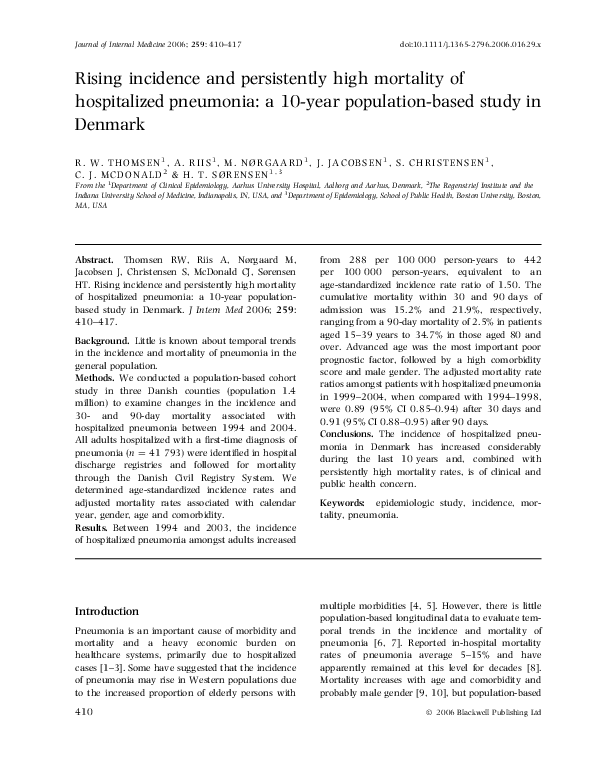
As can bee seen in Fig. 2, mortality rose sharply
with age – from 1.5% (30-day) and 2.5% (90-day)
in patients aged 15–39 years to 24.7% (30-day) and
34.7% (90-day) in patients over age 80 years. This
latter group (‡80 years) accounted for 47% of
deaths after 90 days in our cohort (Table 1).
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 259: 410–417
�HOSPITALIZED PNEUMONIA IN DENMARK
413
Fig. 1 Standardized incidence rates
(SIR) of first-time hospitalized
pneumonia in women and men
according to age group. North Jutland, Aarhus, and Viborg County,
Denmark, 1994–2003. Age standardized to the population of North
Jutland, Aarhus, and Viborg
County in 1994, using 1-year age
groups.
Fig. 2 Survival curves for patients
with first-time hospitalized pneumonia according to age group.
Mortality was also much higher in patients with a
medium or high comorbidity score than in those
with no registered comorbidities (Fig. 3).
Table 1 shows adjusted 30- and 90-day MRRs
according to calendar period, age group, gender and
comorbidity score. A high level of comorbidity, and
in particular advanced age, remained strong predictors of death. Adjusted mortality rates were 15–19%
higher in men than in women. Inclusion of alcoholrelated disorders left the estimates virtually
unchanged (data not shown). When we stratified
analyses by calendar period, the MRRs for male
gender, increased age and comorbidity were
between 2% and 26% higher in 1999–2004 than
in 1994–1998, but none of the differences reached
statistical significance (data not shown).
The overall mortality after hospitalized pneumonia was similar in 1999–2004 compared with
1994–1998. However, the proportion of pneumonia
patients who were 80 years or older, and those with
a high level of comorbidity, increased from 29% to
31% and from 15% to 18%, respectively. After
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 259: 410–417
�MRR, mortality rate ratio. bAdjusted by Cox proportional hazards regression analyses for gender, age, comorbidity and calendar period. cLevel of Charlson index score, see text.
a
1 (ref.)
1.45 (1.38–1.52)
2.07 (1.96–2.19)
1 (ref.)
1.79 (1.71–1.88)
2.62 (2.48–2.77)
1923 (10.5)
1497 (15.8)
2923 (21.0)
18 367
9487
13 939
1 (ref.)
1.69 (1.59–1.79)
2.34 (2.19–2.50)
1 (ref.)
1.37 (1.29–1.45)
1.86 (1.74–1.99)
2678 (14.6)
2104 (22.2)
4372 (31.4)
1 (ref.)
1.19 (1.14–1.24)
1 (ref.)
1.18 (1.13–1.22)
3935 (20.2)
5219 (23.4)
1 (ref.)
1.15 (1.10–1.21)
2765 (14.2)
3578 (16.0)
19 469
22 324
1 (ref.)
1.14 (1.08–1.20)
(ref.)
(3.33–5.21)
(6.07–9.41)
(10.74–16.63)
1
4.17
7.56
13.37
(ref.)
(3.93–6.13)
(7.93–12.25)
(13.58–20.97)
1
4.91
9.86
16.87
(2.5)
(11.6)
(22.1)
(34.7)
83
1114
3619
4338
(ref.)
(3.59–6.41)
(6.55–11.56)
(11.83–20.86)
1
4.80
8.70
15.71
(ref.)
(4.12–7.34)
(8.21–14.45)
(14.40–25.32)
(1.5)
(7.8)
(15.0)
(24.7)
49
749
2452
3093
3331
9576
16 386
12 500
1
5.49
10.89
19.09
1 (ref.)
0.96 (0.92–1.00)
4067 (22.4)
5087 (21.5)
1 (ref.)
0.89 (0.85–0.94)
1 (ref.)
0.93 (0.89–0.98)
2858 (15.7)
3485 (14.8)
18 187
23 606
Calendar year band
1994–1998
1999–2004
Age (years)
15–39
40–64
65–79
80+
Gender
Female
Male
Comorbidity indexc
Low (0)
Medium (1–2)
High (3+)
Crude MRR (95% CI)
Dead (%)
Predictor
n
Dead (%)
Crude MRRa (95% CI)
Adjustedb MRR (95% CI)
90 day
30 day
Table 1 Crude and adjusted 30- and 90-day mortality in hospitalized pneumonia according to calendar period, gender, age group and level of comorbidity
1 (ref.)
0.91 (0.88–0.95)
R . W . T H O M S E N et al.
Adjusted MRR (95% CI)
414
adjustment for these factors and minor gender
differences, the relative mortality for hospitalized
pneumonia in 1999–2004 compared with that in
1994–1998 decreased by 11% (95% CI 6–15%)
after 30 days and 9% (95% CI 5–12%) after 90 days
(Table 1). When we stratified on pneumonia as a
main or secondary diagnosis, the 30-day mortality
rate decreased by 15% (95% CI 9–21%) for secondary pneumonia and by 10% (95% CI 3–16%) for
primary pneumonia.
Discussion
This large population-based study shows that the
incidence of hospitalized pneumonia in a welldefined North European population has increased
by 50% over the last decade. The increase occurred
in all age groups and in both genders. During this
same time period, 30- and 90-day mortality rates
have improved but only slightly.
The strengths of our study include the uniformly
organized Danish public healthcare system that
allowed a population-based design, with inclusion
of all first time hospitalizations with pneumonia
from all hospitals in the region and complete followup for mortality at 90 days. The Charlson index
enabled us to adjust for most underlying diseases in
the survival analyses, and the large study size
provided good statistical precision of the estimates.
Limitations to this study include the use of routine
hospital discharge data to identify patients with
pneumonia and comorbidities, as some coding errors
may have occurred. Nevertheless, we found that the
positive predictive value of hospitalized pneumonia
was high compared with other discharge diagnoses.
Misclassification of comorbidity may have lead to
residual confounding and could affect our mortality
estimates.
The overall annual incidence of hospitalized
pneumonia in our study of 2.9–4.4 per 1000 is
remarkably similar to estimates from the few population-based studies in other industrialized countries, e.g. United States 1988–94 (3.7 per 1000) [1],
Ohio 1991 (2.7 per 1000) [14], Germany 1998 (2.9
per 1000) [4], and Portugal 1998–2000 (2.7 per
1000) [15]. The age-specific incidence rates in 2003
for those aged 65–79 years (12.5 per 1,000) and
those aged ‡80 years (28.0 per 1,000) also correspond well with the annual incidence rate of 18.3 per
1000 amongst Americans aged ‡65 years reported
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 259: 410–417
�HOSPITALIZED PNEUMONIA IN DENMARK
415
Fig. 3 Survival curves for patients
with first-time hospitalized pneumonia according to level of
Charlson index score.
by Kaplan et al. [6], and with Swedish incidence
rates for hospitalized pneumonia of 14.4 per 1000 in
persons aged 75–84 years and 26.3 per 1000 in
those aged ‡85 years [16]. In contrast, our incidence rates were higher than those reported by
Jackson et al. [7] (11.5 per 1000) in persons aged
‡65 years in Washington State, perhaps due to the
fact that their study excluded nursing home residents. However, these studies were not designed to
study temporal trends in pneumonia incidence.
There are several plausible explanations for the
rising incidence of hospitalized pneumonia. One
might posit that physicians may have lowered their
threshold for admitting pneumonia cases over the
period of observation. If that was the case, we would
expect a reduced mortality rate because a greater
proportion of cases would be mild. However, we did
not observe any substantial change in mortality
over this time period. Alternatively, these results
could come from more aggressive coding due to
increasing economic incentives [17]. Again, the
almost unchanged mortality of pneumonia over
time argues against more meticulous case finding
being the main explanation.
It is unlikely that other changes in the Danish
healthcare system accounted for the increase in
pneumonia hospitalization rates. In Denmark as
elsewhere, the vast majority of pneumonia patients
will initially be examined, treated and followed
outside the hospital setting. Patients with severe
pneumonia symptoms, increased risk of complications due to age or comorbidities, or antibiotic
treatment failure will be admitted to a public
hospital in accordance with national guidelines
[18], either by a GP or after direct contact with
the hospital’s emergency room. There have been no
other healthcare facilities than public hospitals for
the treatment of pneumonia in our region during
the study period, and there were only minimal
changes in the number and distribution of available
hospital beds in medical and surgical specialties in
the period 1997–2003, when health statistics were
electronically accessible from the Danish National
Board of Health (available at http://www.sst.dk).
The decreasing median length of hospital stay with
pneumonia in our cohort followed a general trend
for decreasing length of all registered hospitalizations in Denmark between 1994 and 2002 [19].
Demographic changes in our study population did
not explain the rising incidence of hospitalized
pneumonia. However, chronic diseases such as
malignancies, diabetes, stroke sequelae, chronic
obstructive pulmonary disease, and congestive heart
failure have been associated with an increased
pneumonia risk [5, 7, 20], and all of these conditions have become more prevalent in Denmark due
to a number of factors including population ageing,
lifestyle factors, obesity, and a longer disease survival. Other increasingly prevalent factors that might
affect temporal trends in pneumonia prognosis
include the number of surgical procedures performed, particularly in very elderly people, the use of
immunosuppressive treatment including glucocorticoids, and the institutionalization of elderly people
in environments that may promote the transmission
of respiratory tract infections [21]. Only a few of
these putative pneumonia risk factors have been
established from population-based studies, and
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 259: 410–417
�416
R . W . T H O M S E N et al.
properly designed epidemiologic studies are needed
to quantify the effect of these factors on pneumonia
risk and outcome in general populations [7].
Several socio-economic and lifestyle-related factors have been associated with pneumonia, including smoking, crowding and obesity [22, 23].
Smoking appears to be one of the most important
risks factor for pneumonia in both young and elderly
adults [7, 22], but its prevalence has actually
decreased in Denmark during the study period
[24]. This may also hold true for crowding, whereas
the prevalence of obesity has increased [25]. The
results from a study by Baik et al. [22] suggested
that women with a body mass index of 30 or greater
have more than twice the risk of pneumonia than
normal weight women. The higher incidence rate
(and mortality) in men in our study is consistent
with previous findings [7, 10, 14, 26], and
the magnitude of the gender differences amongst
elderly individuals in this study was remarkable. The
specific mechanisms linking male gender with
higher pneumonia risk and mortality have not been
established but may include a higher prevalence of
socio-economic and lifestyle-related risk factors.
The combination of annual influenza vaccination
and pneumococcal vaccination has been suggested
to reduce the risk of subsequent hospitalization with
pneumonia [27]. Exact data for influenza and
pneumococcal vaccination rates in ‘at-risk’ groups
in Denmark are unfortunately lacking, yet by
contrast with many states of the US, annual
influenza vaccination rates in our region probably
have been well below 50% during the study period,
whilst the overall administration of pneumococcal
vaccine has been as low as 2 of 1000 people per year
[28]. In the light of these differences in vaccination
rates, the similarity of pneumonia incidence rates
amongst elderly persons in our Danish region and
the US is interesting.
We found an overall 30-day mortality rate from
hospitalized pneumonia of 15.2% which is higher
than in some previous reports [9, 29] but in
accordance with findings from other populationbased studies [2, 10, 15]. More than one-third of
patients aged ‡80 years with hospitalized pneumonia in our region will not survive 3 months after
admission. The sharply rising mortality rates after
pneumonia with advanced age, and the stepwise
increase in mortality with increasing levels of
comorbidity corroborate previous findings [9, 10].
Nonetheless, it is of clinical concern that the 30-day
mortality for those between 40 and 64 years in
our study reaches about 8%, and this estimate
parallels in-hospital mortality rates from pneumonia
in American seniors between 65 and 69 years in a
similar population-based study by Kaplan et al. [6].
Our findings suggest that hospitalized pneumonia
is a very severe clinical condition even in middleaged adults with mortality rates paralleling those
after acute myocardial infarction or stroke [30, 31].
The mortality after pneumonia improved slightly
during the 10-year period of study. Changes in
prognosis may be due to changes in diagnostic delay
and treatment. Few aspects of pneumonia treatment
are evidence based, but early and appropriate
antibiotic therapy remains the mainstay in treatment [32]. Community-acquired pneumonia treatment guidelines have been virtually unchanged
during the last decade in Denmark and include
penicillin as first choice antimicrobial agent, as
levels of penicillin resistance in the most frequently
detected microbial agent, Streptococcus pneumoniae,
remain uniquely low in Denmark [18].
In conclusion, the incidence of hospitalized pneumonia has increased considerably during the last
decade in Denmark and, combined with persistently
high mortality rates, is of great clinical and public
health concern.
Conflicts of interest statement
No conflict of interest was declared.
Acknowledgements
This work was made possible through financial
support from the ‘Klinisk Epidemiologisk Forskningsfond’, Denmark.
References
1 Niederman MS, McCombs JS, Unger AN, Kumar A, Popovian
R. The cost of treating community-acquired pneumonia. Clin
Ther 1998; 20: 820–37.
2 Carriere KC, Jin Y, Marrie TJ, Predy G, Johnson DH. Outcomes
and costs amongst seniors requiring hospitalization for community-acquired pneumonia in Alberta. J Am Geriatr Soc
2004; 52: 31–8.
3 Scott G, Scott H, Turley M, Baker M. Economic cost of
community-acquired pneumonia in New Zealand adults.
U933. N Z Med J 2004; 117: U933.
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 259: 410–417
�HOSPITALIZED PNEUMONIA IN DENMARK
4 Welte T, Suttorp N, Marre R. CAPNETZ-community-acquired
pneumonia competence network. Infection 2004; 32: 234–8.
5 Oosterheert JJ, Bonten MJ, Hak E, Lammers JW, Schneider
MM, Hoepelman IM. The increase in pneumonia-related
morbidity and mortality among adults in the Netherlands and
possible explanations for it. Ned Tijdschr Geneeskd 2004; 148:
1765–9.
6 Kaplan V, Angus DC, Griffin MF, Clermont G, Scott WR,
Linde-Zwirble WT. Hospitalized community-acquired pneumonia in the elderly: age- and sex-related patterns of care and
outcome in the United States. Am J Respir Crit Care Med 2002;
165: 766–72.
7 Jackson ML, Neuzil KM, Thompson WW et al. The burden of
community-acquired pneumonia in seniors: results of a population-based study. Clin Infect Dis 2004; 39: 1642–50.
8 Fine MJ, Smith MA, Carson CA et al. Prognosis and outcomes
of patients with community-acquired pneumonia. A metaanalysis. JAMA 1996; 275: 134–41.
9 Mortensen EM, Kapoor WN, Chang CC, Fine MJ. Assessment of
mortality after long-term follow-up of patients with community-acquired pneumonia. Clin Infect Dis 2003; 37: 1617–24.
10 Kaplan V, Clermont G, Griffin MF et al. Pneumonia: still the
old man’s friend? Arch Intern Med 2003; 163: 317–23.
11 AnonymousHealth Care in Denmark. Copenhagen: Ministry of
the Interior and Health, 2003. Available at: http://
www.im.dk/publikationer/healthcare_in_dk/index.htm
12 Nickelsen TN. Data validity and coverage in the Danish National Health Registry. A literature review. Ugeskr Laeger
2001; 164: 33–7.
13 de Groot V, Beckerman H, Lankhorst GJ, Bouter LM. How to
measure comorbidity. A critical review of available methods.
J Clin Epidemiol 2003; 56: 221–9.
14 Marston BJ, Plouffe JF, File TM et al. Incidence of communityacquired pneumonia requiring hospitalization. Results of a
population-based active surveillance Study in Ohio. The
Community-Based Pneumonia Incidence Study Group. Arch
Intern Med 1997; 157: 1709–18.
15 Froes F. Pneumonia in the adult population in continental
Portugal – incidence and mortality in hospitalized patients
from 1998 to 2000. Rev Port Pneumol 2003; 9: 187–94.
16 Örtkvist Å. Pneumococcal disease in Sweden: experiences and
current situation. Am J Med 1999; 107: 44S–9S.
17 Hsia DC, Krushat WM, Fagan AB, Tebbutt JA, Kusserow RP.
Accuracy of diagnostic coding for Medicare patients under the
prospective-payment system. N Engl J Med 1988; 318: 352–5.
18 Vestbo J, Benfield T. Pneumonibehandling. Rationel Farmakoterapi 2003; 12: 1–3. Available at: http://www.irf.dk.
19 Nye tal fra Sundhedsstyrelsen nr. 21, 2003. Landspatientregisteret gennem 25 år 1977–2002. Copenhagen: National
Board of Health, 2003.
417
20 LaCroix AZ, Lipson S, Miles TP, White L. Prospective study of
pneumonia hospitalizations and mortality of U.S. older people:
the role of chronic conditions, health behaviours, and nutritional status. Public Health Rep 1989; 104: 350–60.
21 Marrie TJ. Community-acquired pneumonia in the elderly.
Clin Infect Dis 2000; 31: 1066–78.
22 Baik I, Curhan GC, Rimm EB, Bendich A, Willett WC, Fawzi
WW. A prospective study of age and lifestyle factors in relation to community-acquired pneumonia in US men and women. Arch Intern Med 2000; 160: 3082–8.
23 Nuorti JP, Butler JC, Farley MM et al. Cigarette smoking and
invasive pneumococcal disease. Active Bacterial Core Surveillance Team. N Engl J Med 2000; 342: 681–9.
24 Anonymous. The Danish Health and Morbidity Survey 2000.
Copenhagen: National Institute of Public Health, 2000.
25 Sørensen HT, Sabroe S, Gillman M et al. Continued increase in
prevalence of obesity in Danish young men. Int J Obes Relat
Metab Disord 1997; 21: 712–4.
26 Jokinen C, Heiskanen L, Juvonen H et al. Incidence of community-acquired pneumonia in the population of four
municipalities in eastern Finland. Am J Epidemiol 1993; 137:
977–88.
27 Christenson B, Hedlund J, Lundbergh P, Örtqvist Å. Additive
preventive effect of influenza and pneumococcal vaccines in
elderly persons. Eur Respir J 2004; 23: 363–8.
28 Thomsen RW, Hundborg HH, Lervang HH, Johnsen SP,
Schønheyder HC, Sørensen HT. Risk of community-acquired
pneumococcal bacteremia in patients with diabetes: a population-based case-control study. Diabetes Care 2004; 27:
1143–7.
29 Torres OH, Munoz J, Ruiz D et al. Outcome predictors of
pneumonia in elderly patients: importance of functional
assessment. J Am Geriatr Soc 2004; 52: 1603–9.
30 Abildstrøm SZ, Rasmussen S, Rosen M, Madsen M. Trends in
incidence and case fatality rates of acute myocardial infarction in Denmark and Sweden. Heart 2003; 89: 507–11.
31 Moon L, Moise P, Jacobzone S and the ARD-Stroke Experts
Group. Stroke Care in OECD Countries: a Comparison of Treatment, Costs and Outcomes in 17 Countries. Paris: OECD, 2003.
32 Mandell LA, Bartlett JG, Dowell SF, File TM, Jr, Musher DM,
Whitney C. Update of practice guidelines for the management
of community-acquired pneumonia in immunocompetent
adults. Clin Infect Dis 2003; 37: 1405–33.
Correspondence: Reimar Wernich Thomsen MD, PhD, Department
of Clinical Epidemiology, Aarhus University Hospital, Forskningens Hus, Sdr. Skovvej 15, Postbox 365, DK-9100 Aalborg,
Denmark.
(fax: +45 8942 4801; e-mail: uxreth@aas.nja.dk).
� 2006 Blackwell Publishing Ltd Journal of Internal Medicine 259: 410–417
�
 Steffen Christensen
Steffen Christensen