Pathol. Oncol. Res. (2011) 17:349–355
DOI 10.1007/s12253-010-9333-z
RESEARCH
Prognostic Significance of p53 Protein Expression in Early
Gastric Cancer
Andrea Rodrigues Gonçalves & Antonio Jose Vasconcellos Carneiro & Ivanir Martins &
Paulo Antonio Silvestre de Faria & Maria Aparecida Ferreira &
Eduardo Linhares Riello de Mello & Homero Soares Fogaça &
Celeste Carvalho Siqueira Elia & Heitor Siffert Pereira de Souza
Received: 9 August 2010 / Accepted: 28 October 2010 / Published online: 30 November 2010
# Arányi Lajos Foundation 2010
Abstract Mutations of the p53 tumor suppressor gene have
been associated with abnormalities in cell cycle regulation,
DNA repair and synthesis, apoptosis, and it has been
implicated in the prognosis of advanced gastric cancer. The
aim of this study was to evaluate the occurrence of p53
gene mutation and its possible prognostic implications in
early gastric cancer. In a retrospective study, we studied 80
patients with early gastric cancer treated surgically between
1982 and 2001. Mutation of p53 gene was investigated in
surgical gastric specimens by immunohistochemistry, and
results were analyzed in relation to gender, age, macroscopic appearance, size and location of tumor, presence of
A. R. Gonçalves : A. J. V. Carneiro : H. S. Fogaça : C. C. S. Elia :
H. S. P. de Souza
Departamento de Clínica Médica, Hospital Universitário
Clementino Fraga Filho,
Universidade Federal do Rio de Janeiro (UFRJ),
Rio de Janeiro, Brazil 21941-913
A. R. Gonçalves : M. A. Ferreira
Seção de Endoscopia Digestiva, Instituto Nacional do Câncer,
Rio de Janeiro, Brazil 20230-130
I. Martins : P. A. S. de Faria
Divisão de Anatomia Patológica, Instituto Nacional do Câncer,
Rio de Janeiro, Brazil 20230-130
E. L. R. de Mello
e Seção de Cirurgia Oncológica Abdomino-pélvica,
Instituto Nacional do Câncer,
Rio de Janeiro, Brazil 20230-130
H. S. P. de Souza (*)
Rodolpho Paulo Rocco 255, Ilha do Fundao,
Rio de Janeiro, RJ 21941-913, Brazil
e-mail: hsouza@hucff.ufrj.br
H. S. P. Souza
e-mail: heitor.souza@gmail.com
lymph nodes, Lauren’s histological type, degree of differentiation, and the 5-year survival. The expression of p53
was more frequent among the intestinal type (p = 0.003),
the differentiated (p = 0.007), and the macroscopically
elevated tumors (p = 0.038). Nevertheless, the isolated
expression of p53 was not associated with the 5-year
survival, or with the frequency of lymph node involvement.
The degree of differentiation was detected as an independent factor related to the outcome of patients (0.044).
Significantly shorter survival time was found in p53negative compared with p53-positive patients, when considering the degree of differentiation of tumors, as assessed
by Cox regression analysis (0.049). The association of p53
with the intestinal type, the degree of differentiation and
morphological characteristics, may reflect the involvement
of chronic inflammatory process underlying early gastric
cancer. In this population sample, the expression of p53
alone has no prognostic value for early gastric cancer.
However, the significant difference in p53 expression
between subgroups of degree of differentiation of tumors
can influence post-operative outcome of patients and may
be related to possible distinct etiopathogenic subtypes.
Keywords Early gastric cancer . p53 . Prognosis
Introduction
Gastric carcinoma is one of the most common visceral
cancers in the world [1, 2]. Despite recent advances in the
understanding of the biology and development of gastric
cancer, therapeutic effectiveness has been limited and the
prognosis for patients is still poor even in developed
countries [3, 4]. Vascular and lymp node invasion are
usually regarded as indicators of recurrence and poor
�350
outcome commonly seen in advanced gastric cancer [5, 6].
In contrast, early gastric cancer defined as a tumor confined
to the mucosa or submucosa is usually associated with a
better prognosis [7].
Potential molecular markers for gastric cancer have been
pursued and insights into genetic alterations have evolved
considerably in the recent years. Currently, it is thought that
gastric carcinogenesis involves multiple genetic alterations
in a gradual process, and it seems that inadequate
functioning of regulatory mechanisms of apoptosis could
result in tumorigenesis [8, 9]. The p53 tumor suppressor
gene appears to play a pivotal role in human carcinogenesis
[10] and p53 mutations have been frequently reported in
human cancer [11, 12]. The p53 gene encodes a nuclear
phosphoprotein, which functions as a transcription factor
implicated in the regulation of the cell cycle, synthesis and
in DNA repair and apoptosis [13]. Mutations of the p53
gene consequently leading to inactivation of p53 protein
tumor-suppressor activity appear to constitute one of the
most common molecular steps in the development of cancer
[14, 15]. There are evidence indicating the existence of
association between point missense mutations in the p53
gene and p53 protein overexpression in tumors [15], which
is believed to result from a prolonged half-life of the mutant
protein compared with the wild-type p53 [11].
Different studies indicate the association of p53overexpression with gastric cancer and the resulting
reduced survival time for the tumor [16–18]. Other studies
fail to support the significance of p53 expression in the
outcome of gastric cancer [19, 20]. Of note, contradicting
data may derive from differences in patient populations, but
also in immunohistochemical methods employed for the
detection of p53.
In advanced gastric cancer, it has been suggested that
tumors containing the wild-type p53 are more sensitive to
chemotherapeutic agents [21]. On the other hand, in early
gastric cancer p53 has been reported to be associated with
the presence of metastases to lymph nodes, with consequent
impact on prognosis [22]. Overall, the clinical significance
and potential applications of p53 in gastric cancer remain
controversial. In the present study, we investigated the
possible association of p53 protein expression with clinical
and pathological variables and its role in the post-operative
outcome of patients with early gastric cancer.
Materials and Methods
Patients and Samples
Eighty consecutive patients with the diagnosis of early
gastric cancer were submitted to potentially curative
surgery at the Department of Surgical Oncology, National
A.R. Gonçalves et al.
Institute of Cancer, during the period from 1982 to 2001.
Patients with early gastric cancer consisted of 42 men
(52.5%), and 38 women (47.5%), with a mean age of
60 years (std. deviation 14.2 years) and median of 61 years
(range 33–86 years). The surgically resected specimens
used for this study consisted of 37 cases in which tumors
were confined to the mucosa, and 43 cases in which tumors
had reached the submucosa. In regard to follow-up, patients
who died within 1 month after surgery, or died of unrelated
causes within 3 months were excluded from this study. The
histological types of tumors were reviewed and classified as
intestinal or diffuse according to Lauren [23]. None of the
patients had received either chemotherapy or radiation
therapy before surgery.
Formalin-fixed paraffin-embedded blocks from surgical
specimens of primary tumors were retrieved from pathological archives. The most representative slide was selected
from each block obtained after careful review of all slides
from each case by the same pathologist (I.M.). Selected
tissue samples were subsequentely cut into 3 μm sections at
the maximum cross-section of the tumor, onto slides pretreated with poly-L-lysine (Sigma Chemical Co., St Louis,
MO, USA), and processed for the imunohistochemical
study.
The study protocol was approved by the Ethical
Committee of the National Institute of Cancer, Rio de
Janeiro, and informed consent was obtained from all
patients.
Immunohistochemistry
For this set of experiments, paraffin sections were used to
characterize the expression of p53 in early gastric cancer,
which was performed by using the indirect immunoperoxidase technique. Immunohistochemical staining for p53 was
carried out using a monoclonal mouse anti-human p53
antibody diluted 1:50 (DO-7; DAKO) as primary antibody.
Briefly, paraffin-embedded gastric samples were dewaxed in xylene twice for 5 min each time and then
rehydrated in graded ethanol (100–70%) three times,
followed by rehydration in phosphate buffered saline
(PBS), and antigen retrieval by pressure cooking. For
antigen retrieval, sections were immersed in a 10 mM
sodium citrate buffer (pH 6.0), and heated in a pressure
cooker two times for 3 min each at a 10-min interval.
Slides were then immersed in 3% hydrogen peroxide in
methanol for 10 min to block endogenous peroxidase activity.
After being rinsed in PBS containing 0.5% Tween 20 for
10 min, tissue sections were incubated with non-immune
horse serum for 30 min and, subsequently, with the anti-p53
monoclonal antibody in a humidified chamber overnight, at
4oC. Two sections from each sample were incubated with
either PBS alone or mouse monoclonal IgG1 (concentration-
�p53-expression and the Outcome of Early Gastric Cancer
matched) (Dako A/S, Glostrup, Denmark) and served as
negative controls. Positive controls were obtained from
known positive cases of colon cancer. After being rinsed in
PBS for 10 min, all tissue sections were incubated for 30 min
with a goat anti-mouse peroxidase conjugate (1:200) (Zymed
Laboratories, Inc., San Francisco, CA, USA). Additional
rinsing was followed by development with a solution
containing hydrogen peroxide and diaminobenzidine, and
hematoxylin was used for counterstaining. Slides were then
dehydrated and mounted in histological mounting medium.
351
the expression of p53 in the context of various clinical and
pathological variables. Estimation of overall and diseasefree survival rates was calculated using the Kaplan-Meier
method, and differences between curves were assessed with
the log-rank test. Simultaneous multivariate adjustment of
all covariates was performed using the Cox proportional
hazards regression analysis with the forward stepwise
model, to evaluate the independent importance of p53 for
survival after resection. Combinations of potentially confounding variables in regard to p53 alterations were tested.
The level of significance was set at p < 0.05.
Assessment of p53 Expression
A semi-quantitative analysis of tissue sections (under light
microscopy at × 400 magnification) was carried out by
using a computer-assisted image analyser (Image-Pro Plus
Version 4.1 for Windows, Media Cybernetics, LP, Silver
Spring, MD, USA). A distinct nuclear immunoreactivity for
p53 was recorded as positive, and the nuclear staining
pattern was usually diffuse. For tumors that showed
heterogeneous staining, the predominant pattern was taken
into account for scoring. Cases with less than 10%
positively stained cancer cells nuclei were defined as
negative, otherwise they were defined as positive [17].
Statistical Analysis
Statistical analysis was performed using the statistical
software SPSS for Windows (Version 10.0.1, SPSS Inc.,
1989–1999, USA). The Chi-square test was used to analyze
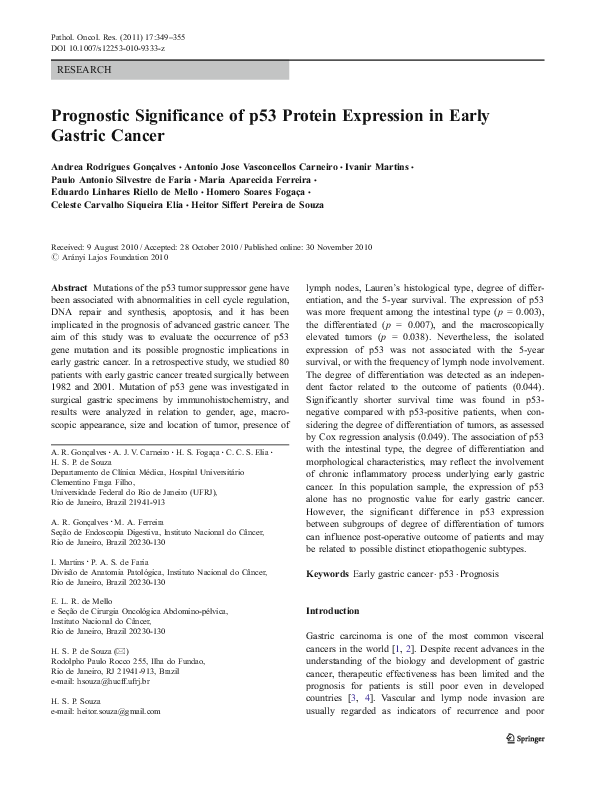
Fig. 1 Immunohistochemical
detection of p53 protein using
anti-p53 monoclonal antibody in
paraffin sections of early gastric
adenocarcinoma. Slides show
the tubular pattern of grade I (A,
B) and grade III (C, D) early
gastric carcinomas, at × 100
magnification, and the characteristic nuclear staining at × 400
magnification, respectively
Results
Of the 80 samples of early gastric cancer studied, 22
(27.5%) overexpressed the p53 protein. The p53 staining
was characteristically nuclear in tumoral tissue and was
completely absent in the normal gastric mucosa in all cases,
as shown in Fig. 1.
Clinicopathological Features
The clinicopathological data of both p53-positive and p53negative patients are shown in Table 1.
The expression of p53 was significantly more frequent in
intestinal than in diffuse Lauren’s histological type (p =
0.003). The degree of differentiation, was also significantly
associated with p53 expression which was found more
often in cases presenting grades I and II (differentiated),
�352
Table 1 Clinicopathological
features and p53 status in
patients with early gastric cancer
NS no significant difference;
figures in parentheses are percentages; a mean ± standard
deviation; b unknown and specific cases were excluded from
statistical analysis.
A.R. Gonçalves et al.
Variable
p53 negative (n = 58)
p53 positive (n = 22)
p-value
Age (years)
Gender
male
Female
Tumor diameter (cm)
Tumor location
Upper
Middle
Lower
Macroscopic type
Elevated
Depressed
Differentiation
Grade I + II
Grade III
64.3 ± 13.6
58.4 ± 14.2
0.890
29
29
4.88 ± 2.44
9
13
3.58 ± 1.51
0.467
11
19
28
7
4
11
0.289
7
51
7
15
0.038
25
33
18
4
0.004
32
26
18
4
0.003
38
20
16
6
0.539
11
47
4
18
0.936
Histological type
Intestinal
Diffuse
Tumor depth
Mucosa
Submucosa
Lymph node
Positive
Negative
0.095
rather than grade III (poorly differentiated) tumor type (p =
0.007). In respect of the macroscopic appearance of tumors,
overexpression of p53 was found more frequently in the
elevated compared to the depressed forms (p = 0.038). The
expression of p53 was not significantly associated with age,
gender, tumor location, tumor diameter, depth of tumor
invasion, and lymph node involvement.
Survival Analysis
The overall 5-year post-operative survival rate was 86.2%
for patients with p53-negative tumors and 86.3% for p53positive tumors (p = 0.985). Deaths which were not
attributed to gastric cancer were regarded as censored data
in the statistical analysis. Of all the other clinicopathological factors analyzed in this study, only the degree of
differentiation was found to significantly affect the survival
of patients (p = 0.044). The survival curve for patients with
p53-negative or p53-positive early gastric cancers was
determined for each grades I and II (differentiated) and
grade III (undifferentiated) type of tumor group. Significantly shorter survival time was noted in p53-negative
patients compared with p53-positive patients, when considering the degree of tumor differentiation (Fig. 2).
Fig. 2 Kaplan-Meier survival curve for patients after surgical
resection of primary early gastric adenocarcinoma categorized
according to p53 status and the degree of tumor differentiation
(a, p53-positive/grade III; b p53-negative/grade III; c p53-positive/
grades I+II; d p53-negative/grades I+II). Significantly improved
overall survival was seen for patients with p53 overexpression, and
for grade III tumors (p = 0.049)
�p53-expression and the Outcome of Early Gastric Cancer
353
Multivariate Analysis of p53 Protein Expression
but following diverse cellular signals, the p53 protein
stabilizes to activate downstream targets [13, 30]. Here,
we utilized immunohistochemistry to assess possible
associations between the expression of p53 with diverse
clinical and pathological variables, and survival, in surgical
samples from 80 patients with the diagnosis of the early
type of gastric cancer. The antibody DO-7, utilized in this
study, recognizes both the wild-type and mutant forms of
p53 [31]. The extended half-life of the mutated p53 protein
makes it more likely to be detected by immunohistochemistry than the wild-type protein [32, 33].
In this study, no p53 staining was observed in any
normal gastric mucosa adjacent to the tumor tissue and the
short half-life of the wild-type protein supports the
suggestion that the immunoreactivity to p53 may reflect
the presence of mutant forms. However, in contrast to
previous studies [17, 20], we did not find any relationship
between p53 expression and a possible more aggressive
biological behaviour of tumors and enhanced proliferating
activity of cancer cells. Differently from studies aiming at
advanced gastric cancer, the p53 abnormal staining in this
study was not related to the depth of tumor invasion, lymph
node metastasis, and to survival of patients [34, 35, 36].
The occurrence of p53 mutation in our series was shown
to be related to Lauren’s histological type and the degree of
differentiation, being more frequent in grade I and II tumors
of the intestinal type. This is in accordance with a previous
study on gastric cancer that reported the association of p53
mutation with the histological intestinal type [37]. In fact, it
has also been proposed that p53 mutation could constitute a
common genetic modification found in the progression of
both histological types of tumor, possibly appearing at
different time-points [38]. The eventual finding of p53
mutation in both histological types has been hypothesized
as an early event in intestinal type and a later event in the
diffuse type [39, 40].
Another possible explanation for the association between
p53 and gastric tumorigenesis derives from the current
knowledge on the developmental process of gastric cancer
of the intestinal type. Gastric cancer of the intestinal type
appears to result from a multi-step process, including
atrophic gastritis, intestinal metaplasia, and dysplasia, all
of them associated with the existence of a chronic
inflammatory process [41]. In the context of chronic
gastritis, H. pylori infection emerges as another factor
capable of inducing the expression of the mutant-type p53
[42, 43], which was shown to be closely associated with the
more severe atrophic and metaplastic changes [44], and also
in gastric cancer [45].
The prognostic implications of p53 mutation in human
malignacies remain controversial. While some investigators
support the relationship of p53 with cancer prognosis [46,
47], others reported that p53 overexpression is actually not
The relationship between p53 expression and other possibly
prognostic variables, such as age, sex, tumor size, lymph
node involvement, was studied using the Cox multivariate
analysis (Table 1). Next, we sought to determine survival
rates for patients in regard to the macroscopic type of
tumor, the degree of differentiation, and the Lauren’s
histologic type, identified as factors related to p53
expression. Variables were eliminated from the model
stepwise in a backward fashion being reincluded whenever
p < 0.05. With this analysis we identified the degree of
differentiation as the only significant variable, with a
relative risk of 4.63 (95% confidence interval, 0.93–
23.02), consisting of an independent factor related to the
outcome of patients and for p53 expression.
Discussion
In order to explore potential clinical applications for the
p53 tumor suppressor gene, this retrospective study was
carried out to characterize p53 alterations in a well-defined
series of surgically resected early gastric adenocarcinomas.
We studied 80 early gastric tumors, documenting p53positive staining in 27.5% of cases. In regard to clinicopathological findings, p53-positive staining was significantly associated with the macroscopically elevated tumors, the
Lauren’s intestinal histological type, and grades I and II
tumors. The 5-year post-operative survival analysis showed
that p53 alone does not represent a prognostic factor.
However, with a multivariate analysis, the histologic degree
of differentiation of tumors was found to represent an
independent factor related to the outcome of patients and
also for p53 expression.
The loss of p53 function is thought to play a critical role
in the development of tumors since point mutations of the
p53 tumor suppressor gene constitute one of the most
frequent molecular alterations implicated in human malignancies [12, 24, 25]. Loss of p53 function would change
the phenotype of neoplastic cells, making them more
sensitive to DNA damage, and accelerating the process of
tumorigenesis [26, 27]. In gastric carcinogenesis, p53
mutation is regarded as a common event, appearing from
the early stage of gastric adenocarcinoma with its specific
mutation spectrum, and also in lesions regarded as tumor
precursors [28, 29].
In normal conditions, the p53 gene is believed to
function as a transcription factor having a variety of
biologic actions, including the regulation of cell cycle,
apoptosis, and maintenance of genomic integrity [10]. In
virtue of its rapid turnover, the phosphoprotein encoded by
the p53 gene usually does not accumulate in normal cells,
�354
related to the prognosis of neoplastic diseases, including
gastric cancer [19, 20]. In this study, the overexpression of
p53 showed no significant relationship with the outcome of
patients. Indeed, it is possible that an association of p53
with cancer prognosis could eventually appear if longer
follow-up periods have been applied, in particular for early
gastric cancer patients, whose recurrence rates are already
expected to be low. However, when analyzing p53 together
with different variables in a model of multivariate analysis
we demonstrated the association of p53 with the histologic
degree of differentiation of tumors, which was shown to
independently impact the outcome of patients. It is possible
that p53 may play an importat role in the initiation of a
variety of tumors, whereas the specific oncogene involved
initially would be probably irrelevant once a tumor has
evolved [48]. In addition, some reports support the
suggestion that a combined assessment of expressions of
p53 with other factors, such as cyclin E and vascular
endothelial growth factor could help in the evaluation of
tumor aggressiveness and prognosis for various cancers
[49], and also with molecules such as HER2 and survivin,
being significantly implicated in the prognosis of patients
with breast [50] and gastric cancers (51), respectively.
In conclusion, in this study, the isolated expression of
p53 has no prognostic impact in early gastric cancer. The
association of p53 with the intestinal type, the degree of
differentiation and morphological characteristics, may
reflect the involvement of specific pathological processes
underlying probable distinct subtypes of early gastric
cancer. Further studies with more patients and a longer
follow-up, and including different molecular biomarkers in
addition to p53, will help in the understanding of disease
pathogenesis and possibly in inidentifying prognostic
factors to guide novel therapeutic approaches.
Acknowledgements The authors wish to thank the Brazilian
foundations CNPq and FAPERJ for financial support.
References
1. Botterweck AA, Schouten LJ, Volovics A, Dorant E, van Den
Brandt PA (2000) Trends in incidence of adenocarcinoma of the
oesophagus and gastric cardia in ten European countries. Int J
Epidemiol 29:645–654
2. Boussioutas A, Taupin D (2001) Towards a molecular approach to
gastric cancer management. Intern Med J 31:296–303
3. Shah MA (2006) Gastric cancer: an update. Curr Oncol Rep
8:183–191
4. Field K, Michael M, Leong T (2008) Locally advanced and
metastatic gastric cancer: current management and new treatment
developments. Drugs 68:299–317
5. Kaibara N, Sumi K, Yonekawa M, Ohta M, Makino M, Kimura
O, Nishidoi H, Koga S (1990) Does extensive dissection of lymph
nodes improve the results of surgical treatment of gastric cancer?
Am J Surg 159:218–221
A.R. Gonçalves et al.
6. Maehara Y, Kabashima A, Koga T, Tokunaga E, Takeuchi H,
Kakeji Y, Sugimachi K (2000) Vascular invasion and potential for
tumor angiogenesis and metastasis in gastric carcinoma. Surgery
128:408–416
7. Forman D, Burley VJ (2006) Gastric cancer: global pattern of the
disease and an overview of environmental risk factors. Best Pract
Res Clin Gastroenterol 20:633–649
8. Anderson C, Nijagal A, Kim J (2006) Molecular markers for
gastric adenocarcinoma: an update. Mol Diagn Ther 10:345–352
9. Smith MG, Hold GL, Tahara E, El-Omar EM (2006) Cellular and
molecular aspects of gastric cancer. World J Gastroenterol
12:2979–2990
10. Prives C, Hall PA (1999) The p53 pathway. J Pathol 187:112–126
11. Greenblatt MS, Bennett WP, Hollstein M, Harris CC (1994)
Mutations in the p53 tumor suppressor gene: clues to cancer
etiology and molecular pathogenesis. Cancer Res 54:4855–4878
12. Hainaut P, Hernandez T, Robinson A, Rodriguez-Tome P, Flores T,
Hollstein M et al (1998) IARC database of p53 gene mutations in
human tumors and cell lines: updated compilation, revised formats
and new visualization tools. Nucleic Acids Res 26:205–213
13. Kastan MB, Onyekwere O, Sidransky D, Vogelstein B, Craig RW
(1991) Participation of p53 protein in the cellular response to
DNA damage. Cancer Res 51:6304–6311
14. Hollstein M, Sidransky D, Vogelstein B, Harris C (1991) p53
mutations in human cancers. Science 253:49–53
15. Lane DP (1994) The regulation of p53 function: Steiner award
lecture. Int J Cancer 57:623–627
16. Starzynska T, Bromley M, Ghosh A, Stern PL (1992) Prognostic
significance of p53 overexpression in gastric and colorectal
carcinoma. Br J Cancer 66:558–562
17. Kakeji Y, Korenaga D, Tsujitani S, Baba H, Anai H, Maehara Y,
Sugimachi K (1993) Gastric cancer with p53 overexpression has
high potential for metastasising to lymph nodes. Br J Cancer
67:589–593
18. Joypaul BV, Hopwood D, Newman EL, Qureshi S, Grant A,
Ogston SA, Lane DP, Cuschieri A (1994) The prognostic
significance of the accumulation of p53 tumour-suppressor gene
protein in gastric adenocarcinoma. Br J Cancer 69:943–946
19. Motojima K, Furui J, Kohara N, Ito T, Kanematsu T (1994)
Expression of p53 protein in gastric carcinomas is not independently prognostic. Surgery 116:890–895
20. Gabbert HE, Muller W, Schneiders A, Meier S, Hommel G (1995)
The relationship of p53 expression to the prognosis of 418
patients with gastric carcinoma. Cancer 76:720–726
21. Bataille F, Rümmele P, Dietmaier W, Gaag D, Klebl F, Reichle A,
Wild P, Hofstädter F, Hartmann A (2003) Alterations in p53
predict response to preoperative high dose chemotherapy in
patients with gastric cancer. Mol Pathol 56:286–92
22. Xiangming C, Hokita S, Natsugoe S, Tanabe G, Baba M, Takao S,
Kuroshima K, Aikou T (1999) Cooccurrence of reduced expression
of alpha-catenin and overexpression of p53 is a predictor of lymph
node metastasis in early gastric cancer. Oncology 57:131–137
23. Lauren P (1965) The two histological main types of gastric
carcinoma: diffuse and so-called intestinal-type carcinoma. An
attempt at a histo-clinical classification. Acta Pathol Microbiol
Scand 64:31–49
24. Montesano R, Hollstein M, Hainaut P (1996) Genetic alterations
in esophageal cancer and their relevance to etiology and
pathogenesis: a review. Int J Cancer 69:225–235
25. Soussi T, Beroud C (2001) Assessing TP53 status in human
tumours to evaluate clinical outcome. Nat Rev Cancer 1:233–240
26. Carson DA, Lois A (1995) Cancer progression and p53. Lancet
346:1009–1011
27. Chang F, Syrjänen S, Syrjänen K (1995) Implications of the p53
tumorsuppressor gene in clinical oncology. J Clin Oncol 13:1009–
1022
�p53-expression and the Outcome of Early Gastric Cancer
28. Yokozaki H, Kuniyasu H, Kitadai Y, Nishimura K, Todo H, Ayhan A,
Yasui W, Ito H, Tahara E (1992) p53 point mutations in primary human
gastric carcinomas. J Cancer Res Clin Oncol 119:67–70
29. Uchino S, Noguchi M, Ochiai A, Saito T, Kobayashi M,
Hirohashi S (1993) p53 mutation in gastric cancer: a genetic
model for carcinogenesis is common to gastric and colorectal
cancer. Int J Cancer 54:759–764
30. Agarwal ML, Taylor WR, Chernov MV, Chernova OB, Stark GR
(1998) The p53 network. J Biol Chem 273:1–4
31. Hall PA, Lane DP (1994) p53 in tumor pathology: can we trust
immunohistochemistry?-Revisited! J Pathol 72:1–4
32. Gannon JV, Greaves R, Iggo R, Lane DP (1990) Activating
mutations in p53 produce a common conformational effect. A
monoclonal antibody specific for the mutant form. EMBO J
9:1595–1602
33. Levine AJ, Momand J, Finlay CA (1991) The p53 tumour
suppressor gene. Nature 351:453–456
34. Maehara Y, Tomoda M, Hasuda S, Kabashima A, Tokunaga E,
Kakeji Y, Sugimachi K (1999) Prognostic value of p53 protein
expression for patients with gastric cancer—a multivariate
analysis. Br J Cancer 79:1255–1261
35. Ming SC (1998) Cellular and molecular pathology of gastric
carcinoma and precursor lesions: A critical review. Gastric Cancer
1:31–50
36. Wang JY, Lin SR, Hsieh JS, Hsu CH, Huang YS, Huang TJ
(2001) Mutations of p53 gene in gastric carcinoma in Taiwan.
Anticancer Res 21:513–520
37. Tahara E, Semba S, Tahara H (1996) Molecular biological
observations in gastric cancer. Semin Oncol 23:307–315
38. Wu MS, Shun CT, Lee WC, Chen CJ, Wang HP, Lee WJ, Sheu
JC, Lin JT (1998) Overexpression of p53 in different subtypes of
intestinal metaplasia and gastric cancer. Br J Cancer 78:971–973
39. Wu MS, Shun CT, Wu CC, Hsu TY, Lin MT, Chang MC, Wang
HP, Lin JT (2000) Epstein-Barr virus-associated gastric carcinomas: relation to H. pylori infection and genetic alterations.
Gastroenterology 118:1031–1038
40. Correa P (1992) Human gastric carcinogenesis: a multistep and
multifactorial process–First American Cancer Society Award
355
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
Lecture on Cancer Epidemiology and Prevention. Cancer Res
52:6735–6740
Kodama M, Fujioka T, Murakami K, Okimoto T, Sato R,
Watanabe K, Nasu M (2005) Eradication of Helicobacter pylori
reduced the immunohistochemical detection of p53 and MDM2 in
gastric mucosa. J Gastroenterol Hepatol 20:941–946
Morgan C, Jenkins GJS, Ashton T, Griffiths AP, Baxter JN, Parry
EM, Parry JM (2003) Detection of p53 mutations in precancerous
gastric tissue. Br J Cancer 89:1314–1319
Kodama M, Murakami K, Okimoto T, Sato R, Watanabe K,
Fujioka T (2007) Expression of mutant type-p53 products in H
pylori-associated chronic gastritis. World J Gastroenterol
13:1541–1546
Li JH, Shi XZ, Lv S, Liu M, Xu GW (2005) Effect of helicobacter
pylori infection on p53 expression of gastric mucosa and
adenocarcinoma with microsatellite instability. World J Gastroenterol 11:4363–4366
Maehara Y, Kakeji Y, Oda S, Baba H, Sugimachi K (2001) Tumor
growth patterns and biological characteristics of early gastric
carcinoma. Oncology 61:102–112
Noda H, Maehara Y, Irie K, Kakeji Y, Yonemura T, Sugimachi K
(2001) Growth pattern and expressions of cell cycle regulator
proteins p53 and p21 WAF1/CIP1 in early gastric carcinoma.
Cancer 92:1828–1835
McLaren R, Kuzu I, Dunnill M, Harris A, Lane D, Gatter KC
(1992) The relationship of p53 immunostaining to survival in
carcinoma of the lung. Br J Cancer 66:735–738
Hamilton JP, Meltzer SJ (2006) A Review of the Genomics of
Gastric Cancer. Clin Gastroenterol Hepatol 4:416–425
Yamashita H, Nishio M, Toyama T, Sugiura H, Zhang Z,
Kobayashi S, Iwase H (2004) Coexistence of HER2 overexpression and p53 protein accumulation is a strong prognostic molecular marker in breast cancer. Breast Cancer Res
6:R24–30
Lu C-D, Altieri DC, Tanigawa N (1998) Expression of A Novel
Antiapoptosis Gene, Survivin, Correlated with Tumor Cell
Apoptosis and p53 Accumulation in Gastric Carcinomas. Cancer
Res 58:1808–1812
�
 Andrea Gonçalves
Andrea Gonçalves