Journal of Experimental Pharmacology
Dovepress
open access to scientific and medical research
REVIEW
Open Access Full Text Article
Experimental Pharmacological Management of
Psoriasis
Elena Campione 1
Terenzio Cosio 1
Monia Di Prete 2
Caterina Lanna 1
Annunziata Dattola 1
Luca Bianchi 1
1
Dermatologic Unit, Department of
Systems Medicine, University of Rome
Tor Vergata, Rome, 00133, Italy;
2
Anatomic Pathology, University of Rome
Tor Vergata, Rome, 00133, Italy
Abstract: Psoriasis is a chronic, relapsing, immune-mediated systemic disease. Its pathogenesis is complex and not fully understood yet. Genetic and epigenetic factors interact with
molecular pathways involving TNF-α, IL-23/IL-17 axis, and peculiar cytokines, as IL-36 or
phosphodiesterase 4. This review discusses the mechanisms involved in the development of
the disease, as well as the therapeutic options proposed following the investigation of the
inflammatory psoriatic pathways. We performed a comprehensive search using the words
“psoriasis” and the newest molecules currently under investigation and approval. From these
data, a new scenario in psoriasis is occurring to personalize the therapies - especially
systemic ones and those using small molecules – and avoid topical and injectable drugs.
We reported the newest therapeutic opportunities, including the inhibitors of Janus kinase/
tyrosine kinase 2, phosphodiesterase-4 and IL-36 receptor. Today, more than 20 molecules
are under investigation for the treatment of cutaneous psoriasis. Most of them are constituted
by small molecules or biologic therapies. This underlines how psoriasis needs systemic
therapies, due to its complex pathogenesis and multisystemic involvement.
Keywords: psoriasis, janus kinase inhibitors, tyrosine kinase 2 inhibitors, phosphodiesterase
4 inhibitors, IL-36 receptors inhibitors
Introduction
Correspondence: Elena Campione
Dermatologic Unit, Department of
Systems Medicine, University of Rome
Tor Vergata, Via Montpellier,1, Rome,
00133, Italy
Tel +39.06.20900252
Email elena.campione@uniroma2.it
Psoriasis is a chronic, relapsing, immune-mediated disease, with a prevalence of
2–3% worldwide. It is characterized by well-circumscribed erythematous plaques,
covered by a squamous scale, generally located on the skin of extensor surfaces of
the body. 20% of patients with psoriasis may develop a seronegative polyarthropathy - often associated with nail involvement - with a severe quality of life
impairment.1 There are several clinical variants of psoriasis. Besides the psoriasis
vulgaris, also called plaque-type psoriasis, we classify guttate, erythrodermic,
sebopsoriasis, generalized pustular (GPP) and palm-plantar forms, and, rarely,
psoriasis of the mucous membranes.1 Actually, these clinical variants show
different cytokines involved in their pathogenesis and different response to therapies. As psoriasis is a dynamic process, microscopic features vary along the
evolution of cutaneous lesions. The earliest lesions could be misinterpreted as
they consist in superficial dermis capillary vessels dilatation and mild perivascular
lymphocytic inflammatory infiltration.2 It is not possible to predict the duration of
this phase, but it is inevitably followed by the development of the classic psoriatic
plaque, which corresponds histologically to confluent parakeratosis with neutrophilic exocytosis in the epidermis. These changes are accompanied by attenuation
Journal of Experimental Pharmacology 2021:13 725–737
Received: 19 April 2021
Accepted: 30 June 2021
Published: 26 July 2021
725
© 2021 Campione et al. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/
terms.php and incorporate the Creative Commons Attribution – Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/). By accessing
the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed.
For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms (https://www.dovepress.com/terms.php).
�Campione et al
to complete loss of granular cell layer, expression of the
accelerated keratinocytes migration process, from the
basal to the corneum layer, without complete
maturation.2 Moreover, basal cell mitotic activity is moderately increased with a consequent characteristic form of
epidermal hyperplasia – known as “psoriasiform hyperplasia”. All these changes are associated with dilated and
tortuous capillary vessels in the papillary dermis with
neutrophils content in their lumen and moderate-tosevere lymphocytic perivascular inflammation. With the
progression of the disease, lots of neutrophils migrate in
the epidermis reaching the more superficial layers and
forming intra-corneal collections, known as Munro’s
microabscesses2 (Figure 1). The pathogenesis of psoriasis
is complex and not fully understood yet. Many genes and
Dovepress
environmental factors, such as stress, injuries, infections,
and certain medications, may be responsible for its onset.
Understanding the mechanisms behind psoriasis is crucial
for the development of new therapies and address tailored
approaches for the patients’ conditions.3 Immune system
impairment is considered a key trait. The IL-23/Th17/IL17 axis seems to have a key role in the onset of the
inflammation in psoriasis. Although there is currently
no definitive cure, various treatment strategies allow prolonged control of the disease. The recently approved new
kinase inhibitors act on IL-23/Th17/IL-17 axis in a more
selective way, resulting in a reduction in adverse events
(AEs) and a chance of therapy for patients with difficultto-treat psoriasis.4 Alongside the common disease modifying anti-rheumatic drugs, several classes of biologicals
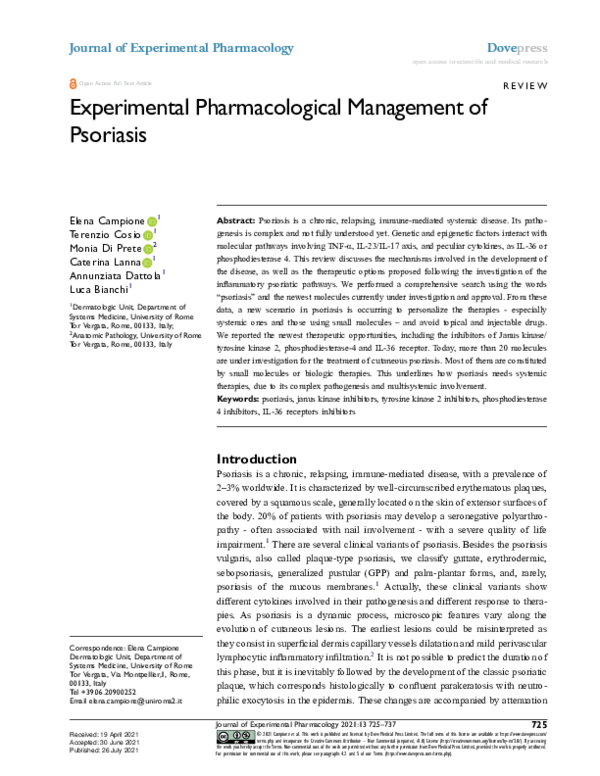
Figure 1 (A) Clinical manifestation of palmar psoriasis. (B) Clinical manifestation of sacral psoriasis. (C) Clinical manifestation of nail psoriasis. All the three clinical images
report the difficult-to-treat areas, recognized as unmet needs by patients and physician. (D) Histopathological features of plaque psoriasis. The classic epidermal psoriasiform
hyperplasia is associated with hyperparakeratosis and loss of granular layer. Collections of neutrophils are observed in the upper stratum spinosum (spongiosiform pustules
of Kogoj). In the dermis, thin capillary vessels reach almost the top of the dermal papillae and are surrounded by a chronic lymphocytic infiltrate with sparse neutrophils
(Haematoxylin-eosin. Original magnification: 100x). (E) Histopathological features of genital psoriasis. The classic features observed in plaque psoriasis are attenuated in the
genital area. The epidermal hyperplasia is associated with less extensive hyperparakeratosis, which is accompanied by mounds of neutrophils in the stratum corneum
(Munro’s microabscesses). In the chorion, thin capillary vessels are surrounded by a chronic lymphocytic infiltrate, with sparse neutrophils (Haematoxylin-eosin. Original
magnification: 200x).
726
Powered by TCPDF (www.tcpdf.org)
https://doi.org/10.2147/JEP.S265632
DovePress
Journal of Experimental Pharmacology 2021:13
�Campione et al
Dovepress
and small molecules are now used in the systemic treatment of psoriasis.5,6 Phosphodiesterase (PDE) 4 inhibitors are largely known to improve both skin and joint
disease, modulating, at the same time, metabolic biomarkers in diabetic psoriatic patients, with the chance to be
employed in psoriatic patients with cardio-metabolic
comorbidities.7,8 Moreover, the small molecules showed
strong efficacy also in nail psoriasis, which is known as
a difficult-to-treat form of the disease. The pathogenetic
mechanisms in this form are not completely overlapping
those of cutaneous psoriasis. For this reason, PDE4 inhibitors, restoring the nail unit IL-10 levels and the immune
privilege site, are particularly effective.9 Advancement in
molecular knowledge leads to understand psoriasis better,
influencing the development of efficient treatment modalities. However, even with the availability of various
therapeutic options, most of the efficient treatment modalities are expensive and are not effective in all subjects.
Due to the complexity of psoriasis pathogenesis and the
paramount influence of epigenetic factors, new drugs
need to be introduced. This review discusses the newest
therapeutic strategies in the management of psoriasis,
starting from its pathogenesis, highlighting their mechanism of actions - intracellular or on inflammatory factors and current trials. In this view, also tyrosine kinase
(TYK) 2 inhibitors – currently in their approval phase have been presented.10
Materials and Methods
Search Strategy
The authors performed a comprehensive search using the
words “psoriasis” and the newest molecules under investigations or just approved by EMA or FDA, as “piclidenoson/CF101”, “namilumab/AMG203”, “imsidolimab/
ANB019”, “spesolimab/BI655130”, “orismilast/LEO 327
31”, “hemay005”, “GSK2981278”, “vimirogant/AGN 242
428/VTP 43742”, “AUR101”, “ABBV-157”, “SCD-044”,
“ponesimod/ACT-128800”, “ND-2158”, “ND-2110”,
“belumosudil/KD025/SLx-2119”, “tapinarof/benvitimod/
WB-1001/GSK-2894512/DMVT-505”, “deucravacitinib/
BMS-986165”. The following databases were evaluated:
Cochrane Central Register of Controlled Trials;
MEDLINE; Embase; US National Institutes of Health
Ongoing Trials Register; NIHR Clinical Research
Network Portfolio Database; and the World Health
Organization International Clinical Trials Registry
Journal of Experimental Pharmacology 2021:13
Platform. Reference lists and published systematic review
articles, starting from year 2018, were studied.
Inclusion Criteria
Only articles written in English were included in the
search, which was restricted to human studies, with no
restrictions on age, sex, ethnicity, or type of study. For
Phase I molecules, preclinical results have been considered
in the Tables S1-S20, and just the name and the mechanism of actions has been reported. Case reports and case
series were included if they described the role of drugs in
psoriasis, not present in reviews or trials.
Exclusion Criteria
The target intervention excluded pathologies not of dermatologic interest. Phase I trials have not been included in
tables and discussion. Analyses excluded articles not written in English.
Results
We identified 142 manuscripts regarding new therapeutic
options against psoriasis. Twenty-six were excluded following the exclusion criteria, while 43 were excluded after
evaluating the trials. A total of 72 studies have been
included in this comprehensive review, counting clinical
trials, published articles, and congress posters (Figure 1S).
Janus Kinases Inhibitors
In order to obtain a more personalized approach according to
the clinical and immunological characteristics of each
patient, inhibitors of the Janus kinases (JAK) 1, 2,and 3
and TYK2 have emerged as a promising strategy in psoriasis
in recent years. The JAK-signal transducer and activator of
transcription (JAK-STAT) pathway plays a crucial role in the
communication between cytokine signals outside the cell
and the cell nucleus, with activation of specific genes transcription in response.11 Cytokines binding to cell membrane
receptors cause their dimerization. The JAKs associated
with these receptors phosphorylate each other, increasing
their kinase domains activity. The consequence is the creation of a SH2 domain-binding site on the receptors, which
bind STATs.11 At this point, STATs are phosphorylated and
activated by JAKs, dissociate from the receptors and dimerize with other activated STATs. STATs dimers are then
translocated to the nucleus starting the transcription.12
JAKs inhibitors (JAKsI) are currently being tested in clinical
trials for the treatment of psoriasis,13 particularly those
included in the IL-23 mechanism of action. Indeed, IL-23
https://doi.org/10.2147/JEP.S265632
DovePress
Powered by TCPDF (www.tcpdf.org)
727
�Campione et al
Dovepress
Table 1 The Table Shows the Molecules Belonging to the Class of Jak Kinase Inhibitor Under Investigation for Psoriasis
Janus Kinases Inhibitors
Target
Systemic
Oral
Deucravacitinib (BMS-986165)
Pembrocitinib (PF-06700841)
TYK2
TYK2/JAK1
✓
✓
✓
✓
Delgocitinib
JAK1, 2, 3 and TYK2
✓
✓
binding to IL-23 receptor causes phosphorylation and activation of JAK-STAT signaling molecules – JAK2, TYK2,
and STAT1, 3, 4, and 5,14 which directly bind to IL-17 and
IL-17F genes promoters.15 STAT3 also up-regulates the
expression of retinoic acid-related orphan receptor (ROR)γ, a Th17 specific transcriptional regulator that is crucial for
IL-17 and IL-17F expression.16 Among JAKsI, deucravacitinib (BMS-986165) has the unique ability to selectively
bind the pseudo-kinase domain of TYK2, inhibiting its
functions, involving IL-12, IL-23, and type I and III interferons (IFN), through an allosteric mechanism17 (Table 1;
Figure 2; Table S1). Selective TYK2 inhibitors are of great
interest for increasing the target specificity and reducing
AEs observed with other types of JAKsI.10,18
Pembrocitinib (PF-06700841) is an oral, dual selective
Intravenous
Subcutaneous
Topical
✓
TYK2/JAK1 inhibitor, targeting multiple cytokines involved
in the signaling (IFN, IL-6, IL-12, IL-21, IL-22, and IL-23),
tested to treat patients with moderate-to-severe plaque psoriasis. From oral formulation, a topical cream 0.1% has been
produced and tested in a Phase II trial (Table 1; Figure 2;
Table S2). Another JAKsI, delgocitinib, has shown in
in vitro studies to inhibit JAK1, 2, and 3 and TYK2 in an
adenosine triphosphate (ATP)-competitive manner, thus
blocking IL-2, IL-6, IL-23, granulocyte-macrophage colonystimulating factor (GM-CSF) and IFN-α signaling.19
Moreover, delgocitinib inhibits inflammatory cells activation, such as T cells, B cells, monocytes and mast cells,
and Th1-, Th2- and Th17-type cytokines production and
secretion, by both T and non-T cells.20 It improves skin
barrier function and enhances keratinocyte differentiation,
Figure 2 Summary of drugs under investigation or with preliminary efficacy in psoriasis disease (red), and drugs with no data reporting efficacy (orange). A) The JAK
inhibitor blocks the JAK-STAT pathway signaling in Th17 cells. Specifically, deucravacitinib inhibits TYK2. B) Tapinarof, an AhR agonist, reduces IL-17 and IL-22 in both Th17
cells and keratinocytes. C) Spesolimab and imsidolimab inhibit IL-36R. D) Imo-8400 inhibits TLR-7/8/9. E) BAY1834345, ND2110 and ND2158 inhibit IRAK4. F) Piclidenoson
inhibits A3AR in keratinocytes. G) Ponesimod, a selective S1PR1 agonist, induces sequestration of lymphocytes into lymph nodes and decreases peripheral lymphocyte
counts and tracking of lymphocytes to peripheral tissues. H) Namilumab has not shown efficacy in psoriasis. J) PDE4 inhibitors act on lymphocytes. K) Among RORγt, just
ABVV-157 and AUR-101 have shown efficacy in psoriasis. L) KD025, a ROCK2 inhibitor, reduces IL-17 secretion in Th17 cells.
Abbreviations: JAK, Janus kinase; STAT, signal transducer and activator of transcription; S1PR1, sphingosine-1-phosphate receptor 1; ROCK2, Rho-associated kinase 2; IL,
interleukin; AhR, aryl hydrocarbon receptor; TLR, toll-like receptor; IRAK, interleukin 1 receptor-associated kinase.
728
Powered by TCPDF (www.tcpdf.org)
https://doi.org/10.2147/JEP.S265632
DovePress
Journal of Experimental Pharmacology 2021:13
�Campione et al
Dovepress
as indicated by increased levels of profilaggrin, filaggrin and
loricrin.21 On the other hand, as delgocitinib is the agent
with a less specific target on the JAK-STAT pathway, more
AEs are expected (Table 1; Figure 2).
Aryl Hydrocarbon Receptor Agonist
Aryl hydrocarbon receptor (AhR) is a cytosolic ligandactivated receptor and transcription factor, which is commonly expressed in the skin cells and binds endogenous and
exogenous molecules and dioxins.22,23 AhR activation
induces oxidative stress through cytochromes P450 and
neutralizes oxidative stress through the nuclear factorerythroid 2-related factor-2 (NRF2) transcription factor.24
Moreover, AhR regulates the Th17/22 axis, which is
involved in psoriasis.24 In addition, AhR in cutaneous vascular endothelial cells (VECs) seems to be involved in the
arising of psoriasis. Zhu et al have discovered that AhR in
cutaneous VECs down-regulates neutrophil recruitment
through adhesion molecule ICAM-1 in psoriasis, using
a AhR knockout mice.25 AhR agonist reduced IL-23 receptor, Th17 master transcription factor, RORC, and the number
of Th17 cells.26 Tapinarof, also known as benvitimod (WB1001, GSK-2894512, and DMVT-505), is a non-steroidal
anti-inflammatory drug in study for the treatment of
psoriasis.27,28 In imiquimod-treated mice, tapinarof demonstrated less inflammation, epidermal thickening, and reduced
pro-inflammatory cytokines, such as IL-17, IL-19, IL-22,
IL-23, and IL-1β. In addition, tapinarof has an antioxidant
activity based on the inhibition of reactive oxygen species
through the NRF2 pathway.27 In ex vivo human skin, tapinarof reduced Th17 cytokines such as IL-17A, IL-17F, and
IL-2227 (Table 2; Figure 2; Table S3).
Retinoic Acid-Related Orphan Receptorγt Inverse Agonists
RORC2 is a crucial transcription factor for Th17 cell
differentiation.29 Inhibiting RORC activity is considered
a promising strategy for the treatment of psoriasis.29 Two
receptor isoforms are produced from the same RORC
gene:30 RORγ (also referred to as RORγ1;31 and RORγt
(also known as RORγ2).32 RORγt is the most studied of
the two isoforms. The transcription factor is essential for
lymph nodes and Peyer’s patches organogenesis.33,34 It
inhibits undifferentiated T cells apoptosis, supporting
their Th17 differentiation, though the regulation of Fas
ligand and IL-2.30 RORγt is a validated drug target for the
treatment of cutaneous inflammatory disorders such as
psoriasis. Among the RORγt inverse agonist, ABBV-157
is a small molecule currently employed in a clinical trial
on the treatment of chronic plaque psoriasis, still in the
recruitment phase (Table 3; Figure 2; Table S4). AUR101
is a potent oral RORγt inverse agonist, with high selectivity among other ROR isoforms, showing IL-17 modulation with an acceptable safety profile, which has
recently completed a phase I human study. AUR-101
has demonstrated inhibition of IL-17A in whole blood
from psoriasis patients and very significant reduction in
histopathology scores in two separate pre-clinical psoriasis models. In addition, AUR-101 has been found to be
safe in preclinical toxicology evaluations, at several fold
of anticipated efficacious doses in humans (Table 3;
Figure 2; Table S5). To data, other two RORγt inverse
agonists have been studied, vimirogant (also known as
AGN 242428 or VTP 43742) and GSK2981278, but no
efficacy in cutaneous psoriasis has been demonstrated
(Tables S6, S18).
Table 2 The Table Shows the Molecules Belonging to the Class of Aryl Hydrocarbon Receptor Agonist Under Investigation for
Psoriasis
Aryl Hydrocarbon Receptor Agonist
Target
Systemic
Tapinarof; Benvitimod (WB-1001; GSK-2894512;
DMVT-505)
Aryl hydrocarbon
receptor
Oral
Intravenous
Subcutaneous
Topical
✓
Table 3 The Table Shows the Molecules Belonging to the Class of Retinoic Acid-Related Orphan Receptor γt Inverse Agonists Under
Investigation for Psoriasis. Vimirogant and GSK2981278 are Reported in the Table S19 Due to Any Efficacy in the Pathology
Retinoic Acid-Related Orphan Receptor γt Inverse Agonists
Target
Systemic
Oral
ABBV-157
AUR101
RORγt
RORγt
✓
✓
✓
✓
Journal of Experimental Pharmacology 2021:13
Intravenous
Subcutaneous
https://doi.org/10.2147/JEP.S265632
DovePress
Powered by TCPDF (www.tcpdf.org)
Topical
729
�Campione et al
Dovepress
Sphingosine-1-Phosphate Receptors
Agonists
activated by Rho GTPases and mediate the phosphorylation
of downstream targets in cells.48,49 ROCK2 down-regulates
autoimmune responses binding phosphorylated-STAT3 and
controlling the formation of ROCK2/STAT3/JAK2 complex
and optimal STAT3 phosphorylation in human CD4+ T cells
during Th17 skewing.50 Thus, ROCK2 seems to be
a promising target in the treatment of immune-mediated
and inflammatory condition, as psoriasis, due to the role on
T cells. Belumosudil (KD025 or SLx-2119) is an oral ROCK
inhibitor Table 5; Figure 2; Table S9). Recent studies have
showed that oral belumosudil administration in healthy subjects, without psoriasis, decreases IL-17 and IL-21 secretion,
induced by ex vivo stimulation.49 Moreover, ROCK2 inhibition shifted the balance between pro-inflammatory and
immunosuppressive T-cell subsets through concurrent regulation of STAT3/STAT5 phosphorylation. In a phase II clinical trial, KD025 significantly reduced both IL-17 and IL-23
levels. Moreover, epidermal thickness, K16 expression, and
T-cell cutaneous infiltration also decreased in skin biopsies of
treated patients.51 In addition, the PASI50 response to
KD025 (200 mg twice daily) at week 12 was 71%.61
Finally, KD025 significantly increased levels of the immunemodulant cytokine IL-10, but tumor necrosis factor (TNF)-α
and IL-6 levels were not changed.51
Sphingosine is an 18-carbon amino alcohol, which forms
a primary part of sphingolipids, a class of cell membrane
lipids created from ceramide, through ceramidase.35 The
Sphingosine-1-phosphate (S1P) is a lipid mediator associated with cellular proliferation, survival, migration,
inflammation, immune cell trafficking, angiogenesis, vascular integrity, and adhesion in the immune and vascular
systems.36 S1P plays on five specific G protein-coupled
receptors named S1P receptors (S1PR) 1–5.36 S1PR1 is
expressed on lymphocytes and controls their way out from
thymus and secondary lymphoid organs.37,38 S1PR1 modulators induce internalization of this receptor and segregation of most circulating lymphocytes in lymph nodes,
decreasing peripheral lymphocytes count and trafficking
to peripheral tissues.39,40 Moreover, it has been described
that S1P hinders the growth of keratinocytes and demonstrates anti-proliferative and anti-inflammatory effects in
mouse models of psoriasis.41–45 It results by keratinocytes
entrance in G0 phase of the cell cycle and is not due to
a cytotoxic effect.45 Moreover, S1P induces calcium intracellular content elevation, and this is a strong signal for
keratinocytes differentiation.35,42 Ponesimod (ACT128800) is an oral selective S1PR1 agonist, which blocks
the egress of T cells from lymphoid organs (Table 4;
Figure 2; Table S7).46,47 SCD-044 is a novel oral S1PR1
agonist that is going to be tested for the treatment of
cutaneous inflammatory diseases such as atopic dermatitis
and psoriasis (Table 4; Figure 2; Table S8).
Interleukin-1 Receptor Associated Kinase
4 Inhibitors
Interleukin-1 receptor associated kinase (IRAK)-4,
a member of serine/threonine kinase family, is a crucial
downstream signaling factor of both toll-like receptors
(TLRs) and IL-1 receptor pathways of innate immune
responses. The main expression of IRAK-4 seems to be on
peripheral blood mononuclear cells and CD8+ cells.52,53
IRAK-4 achieved great attention when results from a poster
Rho-Associated Kinases Inhibitor
Rho family kinases, consisting of Rho-associated coiled-coil
kinase (ROCK) 1 and 2, are serine-threonine kinases
Table 4 The Table Shows the Molecules Belonging to the Class of Sphingosine-1-Phosphate Receptor 1 Agonist Under Investigation
for Psoriasis
Sphingosine-1-Phosphate Receptor 1 Agonist
Target
Systemic
Oral
Ponesimod (ACT-128800)
S1P1R
✓
✓
SCD-044
S1P1R
✓
✓
Intravenous
Subcutaneous
Topical
Table 5 The Table Shows the Molecules Belonging to the Class of Rho-Associated Coiled-Coil Kinase 2 Inhibitor Under Investigation
for Psoriasis
Rho-Associated Coiled-Coil Kinase 2 Inhibitor
Target
Systemic
Oral
Belumosudil (KD025/SLx-2119)
ROCK2
✓
✓
730
Powered by TCPDF (www.tcpdf.org)
https://doi.org/10.2147/JEP.S265632
DovePress
Intravenous
Subcutaneous
Topical
Journal of Experimental Pharmacology 2021:13
�Campione et al
Dovepress
at the Annual Scientific Meeting of American College of
Rheumatology reported the beneficial potentials of selective
and potent IRAK-4 inhibitors in the pre-clinical evaluation
for various inflammatory- and immune-related conditions, as
psoriasis.54 Experimental reports have demonstrated that
IRAK-4 activity reduction stops cytokine production, and
consequently, appear to be promising in inflammatory- and
immune-related disorders.55,56 The oral administration of
IRAK-4 inhibitors (ND-2110, ND-2158) has demonstrated
efficacy in a mouse model of imiquimod-induced psoriasis.55
BAY18344845 is an orally bioavailable small molecule
IRAK-4 inhibitor. It blocks nuclear factor-kappa of B cell
(NF-κB)-mediated secretion of TNF-α, IL-1, and IL-6 in
peripheral blood mononuclear cells. BAY1834845 is currently under investigation for rheumatoid arthritis, other
autoimmune conditions and hematological malignancies.
To data, just one phase I trial is evaluating safety and tolerability of multiple oral doses in healthy male subjects and in
patients with psoriasis (Table 6; Figure 2; Table S17).
Phosphodiesterase-4 Inhibitors
PDE4 is an intracellular non-receptor enzyme modulating
inflammation and epithelial integrity, mainly present in
immune, epithelial, and brain cells.57 Inhibition of PDE4
has several effects via the elevation of the cyclic adenosine
monophosphate (cAMP) levels. It has been identified that
PDE4 is a promising therapeutic target for the treatment of
diverse pulmonary, dermatological, and severe neurological diseases.58 In the skin, PDE4 is primarily expressed in
keratinocytes, neutrophils, Langerhans and T cells, which
contribute to the psoriatic plaque formation.59 Previous
studies demonstrated that PDE4 mRNA level in peripheral
blood was higher in psoriatic patients compared to normal
individuals.59,60 Hemay005 is a novel small molecule
inhibiting PDE4, developed for the treatment of psoriasis
(Table 7; Figure 2; Table S10).61 Oral orismilast (LEO
32731) was developed as a candidate for psoriasis treatment. It has been demonstrated to be superior over placebo
in randomized, double-blinded, placebo-controlled clinical
studies for this indication (Table 7; Figure 2; Table S11).
A3 Adenosine Receptor Agonist
A3 adenosine receptor (A3AR) is expressed on all types of
immune cells with a broad distribution. A direct correlation
has been found between A3AR expression level and disease
progression in inflammatory and cancer diseases, in both
experimental animal models and humans.62 Boukamp et al
demonstrated A3AR over-expression in skin lesions and
peripheral blood of psoriatic patients with moderate-tosevere disease.63 Targeting the receptor with the highly specific agonist piclidenoson (CF101), it was induced the
in vitro inhibition of cell proliferation.63 Moreover, piclidenoson reduces PI3K, p-AKT, NF-κB, TNF-α, IL-17, and IL23 expression, all known to act as potent inflammatory
mediators in psoriasis (Table 8; Figure 2; Table S12).64,65
Toll-Like Receptors Antagonist
TLRs are a class of proteins that plays a key role in the
innate immune system. They are single-pass membranespanning receptors usually expressed on antigen presenting
cells, as macrophages and dendritic cells, that recognize
structurally conserved molecules derived from microbes.
Aberrant TLR-7, 8, and 9 activation by self-nucleic acids
is involved in immune-mediated inflammatory diseases,
such as psoriasis. IMO-8400 is a first-in-class antagonist of
TLR-7, 8, and 9. Balak et al evaluated the short-term safety
and proof-of-concept for efficacy of IMO-8400 in a phase II
trial66 (Table 9; Figure 2; Table S13).
Table 6 The Table Shows the Molecules Belonging to the Class of Interleukin-1 Receptor Associated Kinase 4 Inhibitor Under
Investigation for Psoriasis
Interleukin-1 Receptor Associated Kinase 4 Inhibitor
Target
Systemic
Oral
ND-2110
IRAK4
✓
✓
ND-2158
BAY1834845
IRAK4
IRAK4
✓
✓
✓
✓
Intravenous
Subcutaneous
Topical
Table 7 The Table Shows the Molecules Belonging to the Class of Phosphodiesterase-4 Inhibitors Under Investigation for Psoriasis
Phosphodiesterase-4 Inhibitors
Target
Systemic
Oral
Hemay005
PDE4
✓
✓
Orismilast
PDE4
✓
✓
Journal of Experimental Pharmacology 2021:13
Intravenous
Subcutaneous
https://doi.org/10.2147/JEP.S265632
DovePress
Powered by TCPDF (www.tcpdf.org)
Topical
731
�Campione et al
Dovepress
Table 8 The Table Shows the Molecules Belonging to the Class of A3 Adenosine Receptor Agonist Under Investigation for Psoriasis
A3 Adenosine Receptor Agonist
Target
Systemic
Oral
Piclidenoson
(CF101)
A3AR
✓
✓
Intravenous
Subcutaneous
Topical
Table 9 The Table Shows the Molecules Belonging to the Class of Toll-Like Receptor Antagonist Under Investigation for Psoriasis
Toll-Like Receptor Antagonist
Target
Systemic
IMO-8400
TLR-7, 8, 9
✓
IL-36 Receptor Inhibitors
The IL-36 receptor (IL-36R) axis has been identified as the
involved pathways in GPP and palmo-plantar pustulosis
(PPP). IL-36 is an inflammatory cytokine, member of the IL1 superfamily, secreted by T cells and acting on keratinocytes,
which express IL-36R. IL-36 is composed of three agonists,
IL-36α, IL-36β, and IL-36γ (previously called IL-1F6, IL-1F8,
and IL-1F9) and an antagonist, IL-36 receptor antagonist (IL36Ra, formerly known as IL-1F5).67 Spesolimab (BI 655130),
is a monoclonal antibody that blocks IL-36R, significantly
improving GPP symptoms in moderate and severe disease
flares.68 In vivo studies highlighted the capability of spesolimab to block skin inflammation. Inhibiting the IL-36R pathway results in significant attenuation of skin thickening and
psoriasis-relevant gene expression. These data suggest
a crosstalk between IL-36R and the IL-23/Th17 axis both in
PPP and GPP69 (Table 10; Figure 2; Table S14). Imsidolimab
(ANB019) is an antibody inhibiting the IL-36R function,
which has been initially developed as a therapy in GPP, PPP,
EGFR inhibitors-mediated skin toxicity, and ichthyosis
(Table 10; Figure 2; Table S15).
Granulocyte-Macrophage
Colony-Stimulating Factor
As a major immune modulator, GM-CSF regulation may be
of potential interest in psoriasis treatment. Within the skin,
GM-CSF is produced by activated T lymphocytes, myeloid
cells, endothelial cells, macrophages, fibroblasts and
Oral
Intravenous
Subcutaneous
Topical
✓
keratinocytes. It is detectable in psoriasis related skin blister
fluid and in the serum of patients with psoriasis.70
Namilumab (AMG203) is a human IgG1 monoclonal antibody potently and specifically neutralizing human and
macaque circulating GM-CSF (Table S16). Both in vivo
and in vitro studies supported a hypothetical use of GMCSF inhibitors in psoriasis.71,72 Data from the NEPTUNE
trial have highlighted all benefits from the clinical usage of
namilumab in moderate-to-severe plaque psoriasis (Tables
S14, S20).
Discussion
The involvement of specific cytokine-driven signaling
pathways in the pathogenesis of psoriasis has been the
key observation for the development of target therapies,
some of which are currently used in the clinical setting
with excellent results in terms of induction of disease
remission.13,68,73 Antimicrobial peptides (AMPs) play
important roles in host protection, leading to kill several
microorganisms, including bacteria, protozoa, fungi, and
viruses.74 In psoriasis, certain AMPs, including βdefensins and cathelicidin, are highly expressed and produced by keratinocytes, neutrophils, and macrophages in
response to injury and cytokine secretion.75 They stimulate
TLRs, especially TLR-9 on plasmacytoid dendritic cells,
which, in turn, produce IFN-α and β, promoting myeloid
dendritic cells (mDCs) activation.76 Activated mDCs
migrate to lymph nodes and secrete IL-12 e IL-23, which
modulate the differentiation and proliferation of Th1 and
Table 10 The Table Shows the Molecules Belonging to the Class of Interleukin-36 Receptor Inhibitors Under Investigation for
Psoriasis
Interleukin-36 Receptor Inhibitors
Target
Systemic
Spesolimab
(BI655130)
IL-36R
✓
✓
Imsidolimab (ANB019)
IL-36R
✓
✓
732
Powered by TCPDF (www.tcpdf.org)
https://doi.org/10.2147/JEP.S265632
DovePress
Oral
Intravenous
Subcutaneous
Topical
Journal of Experimental Pharmacology 2021:13
�Dovepress
Th17 lymphocytes subsets respectively.75 Th17 cytokines
(IL-17, IL-21, and IL-22) induce keratinocytes proliferation causing epidermal hyperplasia and thickening.
Intracellular pathways implied in the signal transduction
of these molecules include NF-kB overexpression, with
increased TNF-α and IL-6 production, and JAK-STAT
pathway activation.77 In this context, JAKsI may be
employed in the treatment of psoriasis as they oppose to
the immune-mediated mechanisms underlying psoriasis.69
In particular, as JAK-STAT pathway activation, induced
by IL-23, upregulates STAT3,5 JAKsI down-regulate IL17 and IL-17F transcription, which are critical for Th17
lymphocytes development.16 Among JAKsI, daucravacitinib, with its unique ability to selectively inhibit TYK2
promises to target specific cytokine pathways, involving
IL-12, IL-23, and IFN, arousing great interest for increasing target specificity and reducing AEs.10,17,78 An
increased infections occurrence in patients treated with
JAKsI was expected since TYK2, in particular, is required
for antiviral defense controlled by type I IFN.17 However,
from real life data, the incidence of infections was not
significant when compared to placebo or other small molecules groups. The most common infective events reported
were pharyngitis and upper respiratory tract infections, but
they were mild-to-moderate and did not lead to treatment
discontinuation.18 The different clinical subtypes of psoriasis could be related to different cytokines involved in the
pathogenesis. For instance, recessive mutations in the
antagonist of the IL-36R, belonging to the IL-1 proinflammatory cytokine family, have been linked to
GPP.67 This mutation is also found in PPP and acrodermatitis continua of Hallopeau. In patients with pre-existing
plaque-type psoriasis, the gain-of-function mutation in
CARD14, p.Asp176His, was found to be a predisposing
factor for developing GPP.67 In this context, IL-36R inhibitors conquer a central role in the rational treatment of
GPP and PPP. Improvement in understanding psoriasis
pathogenesis reveals that different clinical psoriatic phenotypes underly various involved cytokines and diverse
genetic substrate. Cumulative evidences implicate
a substantial role of genetic factors in psoriasis susceptibility and manifestations. The genetic basis of psoriasis is
supported by family-based investigations, population
based epidemiological studies, association studies with
human leukocyte antigens (HLAs), genome-wide linkage
scans, and candidate gene studies within and outside the
major histocompatibility complex region.79 The genetic
landscape of psoriasis is dominated by mutations in the
Journal of Experimental Pharmacology 2021:13
Campione et al
psoriasis susceptibility locus 1 (PSORS1), which comprises genes in the HLA complex.80 The strongest HLArelated associations in psoriasis is mapped on HLA-C*06,
particularly in patients with early-onset and more severe
disease who have a positive family history.80 However,
regression analyses have identified at least seven independent HLA genetic signatures for psoriasis based on singlenucleotide polymorphism typing, which have been
mapped by imputation to HLA-C, HLA-B, HLA-A, and
HLA-DRA.81 Confirmed associations include mutations in
the PSORS2 region (17q24-q25), hosting the CARD14
gene;82,83 PSORS4 in the epidermal differentiation
complex;84 PSORS6, on chromosome 19p13, spanning
the TYK2 locus;85 and PSORS7 on chromosome 1p, in
which the IL23R locus is located.86 Studies suggested that
CARD14 gene mutations enhance NF-κB activation,
resulting in abnormal inflammation. NF-κB activation in
keratinocytes should be the target in CARD14-related
psoriasis. Following what was explained before, in the
era of small molecules, these patients could benefit of
PDE4 and IL-36R inhibitors.57,67 More than genetics, epigenetics paved the way to understand the interactions
between gene and environment. Epigenetic modifications
are able to induce chromatin changes without modifying
the DNA sequence.87 Epigenetic mechanisms may operate
at transcriptional (methylation and histone modifications)
and post-transcriptional (microRNAs and long non-coding
RNAs) level. Non-genetic factors (including smoking,
alcohol, stress, drugs assumption, pollution, UV radiation,
and diet) can induce epigenetic responses and, ultimately,
modulate individual gene expression profiles and susceptibility to disease trait.88–90 Small molecules, as PDE4
inhibitors, permit to cure those patients with difficult-totreat or moderate-severe disease. They are of particular
help in the clinical practice, as oral administration and
high security profile in fragile and elderly patients are
very appreciated features in a chronically administrated
therapy. In this view, PDE4 inhibitors resolve the unmet
needs not yet under control with the current biologic
therapies. In the scenario of new targeted therapies, finding
other pathogenetic molecular target in a disease as psoriasis - where the pathogenetic mechanism are not yet fully
understood - is a valid therapeutic option. Based on such
paradigm shift, next generation therapeutic targets might
be identified. It is recognized today that psoriatic patients
present a number of important comorbidities, observed
more often than expected, based on their respective prevalence in general population. These include psoriatic
https://doi.org/10.2147/JEP.S265632
DovePress
Powered by TCPDF (www.tcpdf.org)
733
�Campione et al
arthritis, metabolic syndrome, cardiovascular disorders, as
well as numerous other diseases, such as anxiety/depression, non-alcoholic fatty liver disease, Crohn’s disease, or
lymphoma. High prevalence, chronicity, disfiguration, disability, and associated comorbidity make it a challenge for
clinicians of multiple specialties.86
Conclusions
Several clinical trials in experimental phase may provide
new therapeutic options to satisfy the unmet needs of
patients with a resistant psoriatic disease to the last biologic
therapies. Although the concept of “psoriatic disease” comprises extra-cutaneous manifestations also, we had focused
only on cutaneous disease, to a reason of major clarity.
Several new classes of anti-psoriatic drugs are currently
undergoing clinical development. These new therapies promise earlier and higher-level responses that are durable and
more specific, as they target cytokines involved directly in
psoriatic inflammation. Additionally, based on results from
clinical trials evaluating these new agents, it may be possible
to find predictive markers identifying classes of patients who
are treated with better results with certain drug classes,91
those prone to lose response to treatments, and those who
may discontinue treatment maintaining remission. It remains
to be determined whether the promising results seen in early
studies of therapies in development for psoriasis will translate into actual improvements over currently available treatment options. Numerous small molecules are under
development for psoriasis, although their place in the antipsoriatic treatment schemes has not yet been established.
Nevertheless, advantage in oral administration, reducing
subcutaneous or intravenous therapies, lead JAKsI and
PDE4 inhibitors as the more under development molecules.
In terms of future research, randomized trials comparing
directly active agents are necessary once high-quality evidence of benefit against placebo is established, including
head-to-head trials amongst and between conventional systemic therapies, biological agents and the newest small
molecules.
Acknowledgments
We would like to thank Denis Mariano, who kindly
revised the English language.
Disclosure
The authors report no conflicts of interest in this work.
734
Powered by TCPDF (www.tcpdf.org)
https://doi.org/10.2147/JEP.S265632
DovePress
Dovepress
References
1. Lanna C, Mancini M, Gaziano R, et al. Skin Immunity and Its
Dysregulation in Psoriasis. Cell Cycle. 2019;18:2581–2589.
doi:10.1080/15384101.2019.1653099.
2. Picciani BLS, Domingos TA, Teixeira-Souza T, Santos VDCBD.
Geographic Tongue and Psoriasis: clinical, Histopathological,
Immunohistochemical and Genetic Correlation - a Literature
Review. An Bras Dermatol. 2016;91:410–421. doi:10.1590/
abd1806-4841.20164288.
3. Rønholt K, Iversen L. Old and New Biological Therapies for
Psoriasis. Int J Mol Sci. 2017;18(11):2297. doi:10.3390/
ijms18112297.
4. Sun C, Xia J. Treatment of Psoriasis: janus Kinases Inhibitors and
Biologics for the Interleukin-23/Th17 Axis. Minerva Med.
2020;111:254–265. doi:10.23736/S0026-4806.20.06460-5.
5. Balato A, Campione E, Cirillo T, Malara G, Trifirò C, Bianchi L.
Long-Term Efficacy and Safety of Apremilast in Psoriatic Arthritis:
focus on Skin Manifestations and Special Populations. Dermatol
Ther. 2020;33:e13440. doi:10.1111/dth.13440.
6. Lanna C, Cesaroni GM, Mazzilli S, et al. Apremilast as a Target
Therapy for Nail Psoriasis: a Real-Life Observational Study Proving
Its Efficacy in Restoring the Nail Unit. J Dermatolog Treat.
2020;1–5. doi:10.1080/09546634.2020.1801976.
7. Lanna C, Cesaroni GM, Mazzilli S, Bianchi L, Campione E Small
Molecules, Big Promises: improvement of Psoriasis Severity and
Glucidic Markers with Apremilast: a Case Report. Available from:
https://www.dovepress.com/small-molecules-big-promisesimprovement-of-psoriasis-severity-and-glu-peer-reviewed-articleDMSO. Accessed December 31, 2020.
8. Mazzilli S, Lanna C, Chiaramonte C, et al. Real Life Experience of
Apremilast in Psoriasis and Arthritis Psoriatic Patients: preliminary
Results on Metabolic Biomarkers. J Dermatol. 2020. doi:10.1111/
1346-8138.15293.
9. Lanna C, Cesaroni GM, Mazzilli S, et al. Nails as Immune-Privileged
Sites: a Case of Disabling Acrodermatitis Continua of Hallopeau
Successfully Treated with Apremilast. Dermatol Ther. 2019;32:
e12946. doi:10.1111/dth.12946.
10. Nogueira M, Puig L, Torres T. JAK Inhibitors for Treatment of
Psoriasis: focus on Selective TYK2 Inhibitors. Drugs.
2020;80:341–352. doi:10.1007/s40265-020-01261-8.
11. Kan S-H, Mancini G, Gallagher G. Identification and
Characterization of Multiple Splice Forms of the Human
Interleukin-23 Receptor Alpha Chain in Mitogen-Activated
Leukocytes. Genes Immun. 2008;9:631–639. doi:10.1038/
gene.2008.64.
12. Roskoski R. Janus Kinase (JAK) Inhibitors in the Treatment of
Inflammatory and Neoplastic Diseases. Pharmacol Res.
2016;111:784–803. doi:10.1016/j.phrs.2016.07.038.
13. Schwartz DM, Kanno Y, Villarino A, Ward M, Gadina M,
O’Shea JJJAK. Inhibition as a Therapeutic Strategy for Immune
and
Inflammatory
Diseases.
Nat
Rev
Drug
Discov.
2017;16:843–862. doi:10.1038/nrd.2017.201.
14. O’Shea JJ, Schwartz DM, Villarino AV, Gadina M, McInnes IB,
The LA. JAK-STAT Pathway: impact on Human Disease and
Therapeutic Intervention. Annu Rev Med. 2015;66:311–328.
doi:10.1146/annurev-med-051113-024537.
15. Chen Z, Laurence A, Kanno Y, et al. Selective Regulatory Function
of Socs3 in the Formation of IL-17-Secreting T Cells. Proc Natl Acad
Sci U S A. 2006;103:8137–8142. doi:10.1073/pnas.0600666103.
16. Yang XO, Panopoulos AD, Nurieva R, et al. STAT3 Regulates
Cytokine-Mediated Generation of Inflammatory Helper T Cells.
J Biol Chem. 2007;282:9358–9363. doi:10.1074/jbc.C600321200.
17. Papp K, Gordon K, Thaçi D, et al. Phase 2 Trial of Selective Tyrosine
Kinase 2 Inhibition in Psoriasis. N Engl J Med. 2018;379:1313–1321.
doi:10.1056/NEJMoa1806382.
Journal of Experimental Pharmacology 2021:13
�Dovepress
18. Chang Y, Xu S, Ding K. Tyrosine Kinase 2 (TYK2) Allosteric
Inhibitors To Treat Autoimmune Diseases. J Med Chem.
2019;62:8951–8952. doi:10.1021/acs.jmedchem.9b01612.
19. Tanimoto A, Ogawa Y, Oki C, et al. Pharmacological Properties of
JTE-052: a Novel Potent JAK Inhibitor That Suppresses Various
Inflammatory Responses in Vitro and in Vivo. Inflamm Res.
2015;64:41–51. doi:10.1007/s00011-014-0782-9.
20. Tanimoto A, Shinozaki Y, Yamamoto Y, et al. A Novel JAK Inhibitor
JTE-052 Reduces Skin Inflammation and Ameliorates Chronic
Dermatitis in Rodent Models: comparison with Conventional
Therapeutic Agents. Exp Dermatol. 2018;27:22–29. doi:10.1111/
exd.13370.
21. Amano W, Nakajima S, Kunugi H, et al. The Janus Kinase
Inhibitor JTE-052 Improves Skin Barrier Function through
Suppressing Signal Transducer and Activator of Transcription 3
Signaling. J Allergy Clin Immunol. 2015;136:667–677.e7.
doi:10.1016/j.jaci.2015.03.051.
22. Denison MS, Nagy SR. Activation of the Aryl Hydrocarbon Receptor
by Structurally Diverse Exogenous and Endogenous Chemicals. Annu
Rev Pharmacol Toxicol. 2003;43:309–334. doi:10.1146/annurev.
pharmtox.43.100901.135828.
23. Stockinger B, Di Meglio P, Gialitakis M, Duarte JH. The Aryl
Hydrocarbon Receptor: multitasking in the Immune System. Annu
Rev Immunol. 2014;32:403–432. doi:10.1146/annurev-immunol
-032713-120245.
24. Furue M, Hashimoto-Hachiya A, Tsuji G. Aryl Hydrocarbon
Receptor in Atopic Dermatitis and Psoriasis. Int J Mol Sci. 2019;20
(21):5424. doi:10.3390/ijms20215424.
25. Zhu Z, Chen J, Lin Y, et al. Aryl Hydrocarbon Receptor in Cutaneous
Vascular Endothelial Cells Restricts Psoriasis Development by
Negatively Regulating Neutrophil Recruitment. J Invest Dermatol.
2020;140:1233–1243.e9. doi:10.1016/j.jid.2019.11.022.
26. Ramirez J-M, Brembilla NC, Sorg O, et al. Activation of the Aryl
Hydrocarbon Receptor Reveals Distinct Requirements for IL-22 and
IL-17 Production by Human T Helper Cells. Eur J Immunol.
2010;40:2450–2459. doi:10.1002/eji.201040461.
27. Smith SH, Jayawickreme C, Rickard DJ, et al. Tapinarof Is a Natural
AhR Agonist That Resolves Skin Inflammation in Mice and Humans.
J Invest Dermatol. 2017;137:2110–2119. doi:10.1016/j.jid.2017.
05.004.
28. Richardson WH, Schmidt TM, Nealson KH. Identification of an
Anthraquinone Pigment and a Hydroxystilbene Antibiotic from
Xenorhabdus
Luminescens.
Appl
Environ
Microbiol.
1988;54:1602–1605. doi:10.1128/aem.54.6.1602-1605.1988
29. Tang L, Yang X, Liang Y, Xie H, Dai Z, Zheng G. Transcription
Factor Retinoid-Related Orphan Receptor Γt: a Promising Target for
the Treatment of Psoriasis. Front Immunol. 2018;9. doi:10.3389/
fimmu.2018.01210
30. He Y-W, Deftos ML, Ojala EW, Bevan MJ. RORγt, a Novel Isoform
of an Orphan Receptor, Negatively Regulates Fas Ligand Expression
and IL-2 Production in T Cells. Immunity. 1998;9:797–806.
doi:10.1016/S1074-7613(00)80645-7
31. Medvedev A, Chistokhina A, Hirose T, Jetten AM. Genomic
Structure and Chromosomal Mapping of the Nuclear Orphan
Receptor ROR Gamma (RORC) Gene. Genomics. 1997;46:93–102.
doi:10.1006/geno.1997.4980.
32. Villey I, de Chasseval R, de Villartay JP. RORgammaT, a
Thymus-Specific Isoform of the Orphan Nuclear Receptor
RORgamma/TOR, Is up-Regulated by Signaling through the
Pre-T Cell Receptor and Binds to the TEA Promoter. Eur
J Immunol. 1999;29:4072–4080. doi:10.1002/(SICI)1521-4141(199912)29:12<4072::aid-immu4072>3.0.CO;2-E.
33. Eberl G, Littman DR. The Role of the Nuclear Hormone Receptor
RORgammat in the Development of Lymph Nodes and Peyer’s
Patches. Immunol Rev. 2003;195:81–90. doi:10.1034/j.1600065x.2003.00074.x.
Journal of Experimental Pharmacology 2021:13
Campione et al
34. Ivanov II, McKenzie BS, Zhou L, et al. The Orphan Nuclear
Receptor RORgammat Directs the Differentiation Program of
Proinflammatory IL-17+ T Helper Cells. Cell. 2006;126:1121–1133.
doi:10.1016/j.cell.2006.07.035.
35. Borodzicz S, Rudnicka L, Mirowska-Guzel D, CudnochJedrzejewska A. The Role of Epidermal Sphingolipids in
Dermatologic Diseases. Lipids Health Dis. 2016;15:13. doi:10.1186/
s12944-016-0178-7.
36. Kunkel GT, Maceyka M, Milstien S, Spiegel S. Targeting the
Sphingosine-1-Phosphate Axis in Cancer, Inflammation and
Beyond. Nat Rev Drug Discov. 2013;12:688–702. doi:10.1038/
nrd4099.
37. Krause A, D’Ambrosio D, Dingemanse J. Modeling Clinical Efficacy
of the S1P Receptor Modulator Ponesimod in Psoriasis. J Dermatol
Sci. 2018;89:136–145. doi:10.1016/j.jdermsci.2017.11.003.
38. Cyster JG, Schwab SR. Sphingosine-1-Phosphate and Lymphocyte
Egress from Lymphoid Organs. Annu Rev Immunol. 2012;30:69–94.
doi:10.1146/annurev-immunol-020711-075011.
39. Chew WS, Wang W, Herr DR. To Fingolimod and beyond: the Rich
Pipeline of Drug Candidates That Target S1P Signaling. Pharmacol
Res. 2016;113:521–532. doi:10.1016/j.phrs.2016.09.025.
40. Piali L, Froidevaux S, Hess P, et al. The Selective Sphingosine
1-Phosphate Receptor 1 Agonist Ponesimod Protects against
Lymphocyte-Mediated Tissue Inflammation. J Pharmacol Exp Ther.
2011;337:547–556. doi:10.1124/jpet.110.176487.
41. Ji M, Xue N, Lai F, et al. Validating a Selective S1P1 Receptor
Modulator Syl930 for Psoriasis Treatment. Biol Pharm Bull.
2018;41:592–596. doi:10.1248/bpb.b17-00939.
42. Vogler R, Sauer B, Kim D-S, Schäfer-Korting M, Kleuser B.
Sphingosine-1-Phosphate and Its Potentially Paradoxical Effects on
Critical Parameters of Cutaneous Wound Healing. J Invest Dermatol.
2003;120:693–700. doi:10.1046/j.1523-1747.2003.12096.x.
43. Schüppel M, Kürschner U, Kleuser U, Schäfer-Korting M. Sphingosine
1-Phosphate Restrains Insulin-Mediated Keratinocyte Proliferation via
Inhibition of Akt through the S1P2 Receptor Subtype. J Invest
Dermatol. 2008;128:1747–1756. doi:10.1038/sj.jid.5701259.
44. Schaper K, Dickhaut J, Japtok L, et al. Sphingosine-1-Phosphate
Exhibits Anti-Proliferative and Anti-Inflammatory Effects in Mouse
Models of Psoriasis. J Dermatol Sci. 2013;71:29–36. doi:10.1016/j.
jdermsci.2013.03.006.
45. Manggau M, Kim DS, Ruwisch L, et al. 1Alpha,25-Dihydroxyvitamin
D3 Protects Human Keratinocytes from Apoptosis by the Formation of
Sphingosine-1-Phosphate. J Invest Dermatol. 2001;117:1241–1249.
doi:10.1046/j.0022-202x.2001.01496.x.
46. Park S-J, Im D-S. Sphingosine 1-Phosphate Receptor Modulators and
Drug Discovery. Biomol Ther (Seoul). 2017;25:80–90. doi:10.4062/
biomolther.2016.160.
47. Bolli MH, Abele S, Binkert C, et al. 2-Imino-Thiazolidin-4-One
Derivatives as Potent, Orally Active S1P1 Receptor Agonists.
J Med Chem. 2010;53:4198–4211. doi:10.1021/jm100181s.
48. Riento K, Ridley AJ. Rocks: multifunctional Kinases in Cell Behaviour.
Nat Rev Mol Cell Biol. 2003;4:446–456. doi:10.1038/nrm1128.
49. Zanin-Zhorov A, Weiss JM, Nyuydzefe MS, et al. Selective Oral
ROCK2 Inhibitor Down-Regulates IL-21 and IL-17 Secretion in
Human T Cells via STAT3-Dependent Mechanism. Proc Natl Acad
Sci U S A. 2014;111:16814–16819. doi:10.1073/pnas.1414189111.
50. Chen W, Nyuydzefe MS, Weiss JM, Zhang J, Waksal SD, ZaninZhorov A. ROCK2, but Not ROCK1 Interacts with Phosphorylated
STAT3 and Co-Occupies TH17/TFH Gene Promoters in
TH17-Activated Human T Cells. Sci Rep. 2018;8:16636.
doi:10.1038/s41598-018-35109-9.
51. Zanin-Zhorov A, Weiss JM, Trzeciak A, et al. Cutting Edge: selective
Oral ROCK2 Inhibitor Reduces Clinical Scores in Patients with
Psoriasis Vulgaris and Normalizes Skin Pathology via Concurrent
Regulation of IL-17 and IL-10. J Immunol. 2017;198:3809–3814.
doi:10.4049/jimmunol.1602142.
https://doi.org/10.2147/JEP.S265632
DovePress
Powered by TCPDF (www.tcpdf.org)
735
�Campione et al
52. Li S, Strelow A, Fontana EJ, Wesche H. IRAK-4: a Novel Member of
the IRAK Family with the Properties of an IRAK-Kinase. Proc Natl
Acad Sci U S A. 2002;99:5567–5572. doi:10.1073/pnas.082100399.
53. Kim TW, Staschke K, Bulek K, et al. A Critical Role for IRAK4
Kinase Activity in Toll-like Receptor–Mediated Innate Immunity.
J Exp Med. 2007;204:1025–1036. doi:10.1084/jem.20061825.
54. Croasdell G. A Report from the American College of Rheumatology/
Association of Rheumatology Health Professionals (ACR/ARHP) 2012 Annual Meeting (November 9–14, 2012 - Washington, D.C.,
USA). Drugs Today (Barc). 2013;49:153–155. doi:10.1358/
dot.2013.49.2.1937427.
55. Koziczak-Holbro M, Littlewood-Evans A, Pöllinger B, et al. The
Critical
Role
of
Kinase
Activity
of
Interleukin-1
Receptor-Associated Kinase 4 in Animal Models of Joint
Inflammation. Arthritis Rheum. 2009;60:1661–1671. doi:10.1002/
art.24552.
56. Staschke KA, Dong S, Saha J, et al. IRAK4 Kinase Activity Is
Required for Th17 Differentiation and Th17-Mediated Disease.
J Immunol. 2009;183:568–577. doi:10.4049/jimmunol.0802361.
57. Sanz MJ, Cortijo J, Morcillo EJ. PDE4 Inhibitors as New
Anti-Inflammatory Drugs: effects on Cell Trafficking and Cell
Adhesion
Molecules
Expression.
Pharmacol
Ther.
2005;106:269–297. doi:10.1016/j.pharmthera.2004.12.001.
58. Li H, Zuo J, Tang W. Phosphodiesterase-4 Inhibitors for the
Treatment of Inflammatory Diseases. Front Pharmacol.
2018;9:1048. doi:10.3389/fphar.2018.01048.
59. Chiricozzi A, Caposiena D, Garofalo V, et al. Therapeutic for the
Treatment of Moderate-to-Severe Plaque Psoriasis: apremilast.
Expert Rev Clin Immunol. 2016;12:237–249. doi:10.1586/
1744666X.2016.1134319.
60. Schafer PH, Adams M, Horan G, Truzzi F, Marconi A, Pincelli C.
Apremilast Normalizes Gene Expression of Inflammatory Mediators
in Human Keratinocytes and Reduces Antigen-Induced Atopic
Dermatitis in Mice. Drugs R D. 2019;19:329–338. doi:10.1007/
s40268-019-00284-1.
61. Liu X, Chen R, Zeng G, et al. Determination of a PDE4 Inhibitor
Hemay005 in Human Plasma and Urine by UPLC-MS/ MS and Its
Application to a PK Study. Bioanalysis. 2018;10:863–875.
doi:10.4155/bio-2018-0004.
62. Fishman P, Bar-Yehuda S, Liang BT, Jacobson KA. Pharmacological
and Therapeutic Effects of A3 Adenosine Receptor Agonists. Drug
Discov Today. 2012;17:359–366. doi:10.1016/j.drudis.2011.10.007.
63. Boukamp P, Petrussevska RT, Breitkreutz D, Hornung J, Markham A,
Fusenig NE. Normal Keratinization in a Spontaneously Immortalized
Aneuploid Human Keratinocyte Cell Line. J Cell Biol.
1988;106:761–771. doi:10.1083/jcb.106.3.761.
64. Cohen S, Barer F, Itzhak I, Silverman MH, Fishman P. Inhibition of
IL-17 and IL-23 in Human Keratinocytes by the A3 Adenosine
Receptor
Agonist
Piclidenoson.
J
Immunol
Res.
2018;2018:2310970. doi:10.1155/2018/2310970.
65. David M, Gospodinov DK, Gheorghe N, et al. Treatment of
Plaque-Type Psoriasis With Oral CF101: data from a Phase II/III
Multicenter, Randomized, Controlled Trial. J Drugs Dermatol.
2016;15:931–938.
66. Balak DMW, van Doorn MBA, Arbeit RD, et al. IMO-8400, a
Toll-like Receptor 7, 8, and 9 Antagonist, Demonstrates Clinical
Activity in a Phase 2a, Randomized, Placebo-Controlled Trial in
Patients with Moderate-to-Severe Plaque Psoriasis. Clin Immunol.
2017;174:63–72. doi:10.1016/j.clim.2016.09.015.
67. Yuan Z-C, Xu W-D, Liu X-Y, Liu X-Y, Huang A-F, Su L-C. Biology
of IL-36 Signaling and Its Role in Systemic Inflammatory Diseases.
Front Immunol. 2019;10. doi:10.3389/fimmu.2019.02532
68. Bachelez H, Choon S-E, Marrakchi S, et al. Inhibition of the
Interleukin-36 Pathway for the Treatment of Generalized Pustular
Psoriasis. N Engl J Med. 2019;380:981–983. doi:10.1056/
NEJMc1811317.
736
Powered by TCPDF (www.tcpdf.org)
https://doi.org/10.2147/JEP.S265632
DovePress
Dovepress
69. Su Z, Paulsboe S, Wetter J, et al. IL-36 Receptor Antagonistic
Antibodies Inhibit Inflammatory Responses in Preclinical Models of
Psoriasiform Dermatitis. Exp Dermatol. 2019;28:113–120.
doi:10.1111/exd.13841.
70. Bonifati C, Carducci M, Fei PC, et al. Correlated Increases of
Tumour Necrosis Factor-α, Interleukin-6 and Granulocyte
Monocyte-Colony Stimulating Factor Levels in Suction Blister
Fluids and Sera of Psoriatic Patients Relationships with Disease
Severity. Clin Exp Dermatol. 1994;19:383–387. doi:10.1111/
j.1365-2230.1994.tb02687.x.
71. Alvarez-Ruiz S, Peñas PF, Fernández-Herrera J, Sánchez-Pérez J,
Fraga J. Maculopapular Eruption with Enlarged Macrophages in
Eight Patients Receiving G-CSF or GM-CSF. J Eur Acad Dermatol
Venereol. 2004;18:310–313. doi:10.1111/j.1468-3083.2004.00872.x.
72. Kelly R, Marsden RA, Bevan D. Exacerbation of Psoriasis with
GM-CSF Therapy. Br J Dermatol. 1993;128:468–469. doi:10.1111/
j.1365-2133.1993.tb00218.x.
73. Koziczak-Holbro M, Joyce C, Glück A, et al. IRAK-4 Kinase
Activity Is Required for Interleukin-1 (IL-1) Receptor- and
Toll-like Receptor 7-Mediated Signaling and Gene Expression.
J
Biol
Chem.
2007;282:13552–13560.
doi:10.1074/jbc.
M700548200.
74. Lai Y, Gallo RL. AMPed Up Immunity: how Antimicrobial Peptides
Have Multiple Roles in Immune Defense. Trends Immunol.
2009;30:131–141. doi:10.1016/j.it.2008.12.003.
75. Rendon A, Schäkel K. Psoriasis Pathogenesis and Treatment.
Int J Mol Sci. 2019;20. doi:10.3390/ijms20061475
76. Mylonas A, Conrad C. Psoriasis: classical vs. Paradoxical. The
Yin-Yang of TNF and Type I Interferon. Front Immunol.
2018;9:2746. doi:10.3389/fimmu.2018.02746.
77. Lowes MA, Suárez-Fariñas M, Krueger JG. Immunology of
Psoriasis. Annu Rev Immunol. 2014;32:227–255. doi:10.1146/
annurev-immunol-032713-120225.
78. Liu C, Lin J, Langevine C, et al. Discovery of BMS-986202:
a Clinical Tyk2 Inhibitor That Binds to Tyk2 JH2. J Med Chem.
2021;64:677–694. doi:10.1021/acs.jmedchem.0c01698.
79. AlShobaili HA, Shahzad M, Al-Marshood A, Khalil A, Settin A,
Barrimah I. Genetic Background of Psoriasis. Int J Health Sci
(Qassim). 2010;4:23–29.
80. Greb JE, Goldminz AM, Elder JT, et al. Psoriasis. Nat Rev Dis
Primers. 2016;2:16082. doi:10.1038/nrdp.2016.82.
81. Baran W, Szepietowski JC, Mazur G, Baran EA. 308 Promoter
Polymorphism of Tumor Necrosis Factor Alpha Gene Does Not
Associate with the Susceptibility to Psoriasis Vulgaris. No
Difference Either between Psoriasis Type I and Type II Patients.
Acta Dermatovenerol Alp Pannonica Adriat. 2006;15:113–118.
82. Carroll JM, Romero MR, Watt FM. Suprabasal Integrin Expression in
the Epidermis of Transgenic Mice Results in Developmental Defects
and a Phenotype Resembling Psoriasis. Cell. 1995;83:957–968.
doi:10.1016/0092-8674(95)90211-2.
83. Signa S, Campione E, Rusmini M, et al. Whole Exome Sequencing
Approach to Childhood Onset Familial Erythrodermic Psoriasis
Unravels a Novel Mutation of CARD14 Requiring Unusual High
Doses of Ustekinumab. Pediatr Rheumatol Online J. 2019;17:38.
doi:10.1186/s12969-019-0336-3.
84. Hammer RE, Maika SD, Richardson JA, Tang JP, Taurog JD.
Spontaneous Inflammatory Disease in Transgenic Rats Expressing
HLA-B27 and Human Beta 2m: an Animal Model of HLA-B27Associated
Human
Disorders.
Cell.
1990;63:1099–1112.
doi:10.1016/0092-8674(90)90512-d.
85. Stern RS. Psoriasis. Lancet. 1997;350:349–353. doi:10.1016/S01406736(97)05257-4.
86. Boehncke WH, Sterry W, Hainzl A, Scheffold W, Kaufmann R.
Psoriasiform Architecture of Murine Epidermis Overlying Human
Psoriatic Dermis Transplanted onto SCID Mice. Arch Dermatol
Res. 1994;286:325–330. doi:10.1007/BF00402223.
Journal of Experimental Pharmacology 2021:13
�Campione et al
Dovepress
87. Furrow RE, Christiansen FB, Feldman MW. Environment-Sensitive
Epigenetics and the Heritability of Complex Diseases. Genetics.
2011;189:1377–1387. doi:10.1534/genetics.111.131912.
88. Fogel O, Richard-Miceli C, Tost J. Epigenetic Changes in Chronic
Inflammatory Diseases. Adv Protein Chem Struct Biol.
2017;106:139–189. doi:10.1016/bs.apcsb.2016.09.003.
89. Mervis JS, McGee JS. Epigenetic Therapy and Dermatologic
Disease: moving beyond CTCL. J Dermatolog Treat.
2019;30:68–73. doi:10.1080/09546634.2018.1473550.
90. Caputo V, Strafella C, Termine A, et al. Overview of the Molecular
Determinants Contributing to the Expression of Psoriasis and
Psoriatic
Arthritis
Phenotypes.
J
Cell
Mol
Med.
2020;24:13554–13563. doi:10.1111/jcmm.15742.
91. Campione E, Cosio T, Lanna C, et al. Predictive Role of Vitamin
A Serum Concentration in Psoriatic Patients Treated with IL-17
Inhibitors to Prevent Skin and Systemic Fungal Infections.
J Pharmacol Sci. 2020;144:52–56. doi:10.1016/j.jphs.2020.06.003.
Dovepress
Journal of Experimental Pharmacology
Publish your work in this journal
The Journal of Experimental Pharmacology is an international, peerreviewed, open access journal publishing original research, reports,
reviews and commentaries on all areas of laboratory and experimental pharmacology. The manuscript management system is completely
online and includes a very quick and fair peer-review system. Visit
http://www.dovepress.com/testimonials.php to read real quotes from
published authors.
Submit your manuscript here: https://www.dovepress.com/journal-of-experimental-pharmacology-journal
Journal of Experimental Pharmacology 2021:13
Powered by TCPDF (www.tcpdf.org)
DovePress
737
�
 Terenzio Cosio
Terenzio Cosio