Scientific Abstracts
74 patients. 55/74 (74,3%) patients experienced more than one hospitalization. In
the majority of the hospitalizations (119/285, 41,7%), the cause of hospitalization
was directly attributable to the disease itself, while the second cause of hospitalization was the infections (26/285, 9,1%). In 10/103 patients (9,7%), an end stage
renal disease was recorded as event. The presence of at least one positivity for
ANCA antibodies was documented in 76/103 patients (73,8%), mainly in patients
carrying GPA. Globally, the presence of ANCA antibody seems to be associated
with greater likelihood of an event (p=0,07, log-rank test). The first event occurred
in 50% of ANCA-positive patients within 180 days from diagnosis, while in 50%
of ANCA negative patients in 859 days. 6 out of the 7 deaths occurred in ANCA
positive patients.
Conclusion: the rate of hospitalization in AAV is very high confirming the high
health care burden of illness. The disease itself is often the cause of the hospitalization, as well as the infectious complication, highlighting the need for more
effective treatments, and glucocorticoid sparing therapies. ANCA antibody may
represent a biomarker of a more serious disease.
Disclosure of Interests: Luca Quartuccio Consultant of: Abbvie, Bristol, Speakers
bureau: Abbvie, Pfizer, Elena Treppo: None declared, Salvatore De Vita Consultant of:
Roche, GSK, Speakers bureau: Roche, GSK, Novartis, Francesca Valent: None declared
DOI: 10.1136/annrheumdis-2020-eular.2567
AB0521
COST OF ILLNESS OF ANCA-ASSOCIATED
VASCULITIS IN ITALY: DATA LINKAGE ANALYSIS
OF MULTIPLE CLINICAL AND ADMINISTRATIVE
DATABASES IN THE PROVINCE OF UDINE, ITALY
L. Quartuccio1, E. Treppo1, S. De Vita1, F. Valent2. 1Clinic of Rheumatology,
Department of Medicine, Academic Hospital “Santa Maria della Misericordia”,
ASUI, Udine, Italy, Udine, Italy; 2Institute of Epidemiology, Academic Hospital
“Santa Maria della Misericordia”, ASUI, Udine, Italy, Udine, Italy
Background: ANCA-associated vasculitides (AAV) are a group of systemic vasculitis carrying a high risk of hospitalization because the multiorgan involvement,
the acute nature of some clinical manifestations, the chronic but very disabling
course of some other manifestations and finally the risk of severe infections due
to chronic glucocorticoid and immunosuppressor administration. However, data
on cost of illness due to AAV are lacking.
Objectives: to estimate the cost of illness in patients suffering from AAV in the
province of Udine (about 500,000 inhabitants), Friuli Venezia Giulia (FVG), Italy,
from year 2010 to 2018.
Methods: integration of the information coming from many administrative databases were used to this end. The Regional Health Information System of FVG
was used as the source of information for this retrospective cohort study. The
system covers the entire regional population and includes various electronic
health administrative databases that can be linked with one another on an individual basis through a unique encrypted identifier. In particular, the following
databases were matched: the database of the health care beneficiaries (including demographic information and the residential history of all of the subjects
living in FVG), the hospital discharge database, the database of exemptions
from medical charges, the database of the laboratories. The population under
study was selected based on the following inclusion criteria: patients were residents in the province of Udine and they had to carry the exemption code for
AAV, including GPA, or EGPA, or MPA. This population was observed from
2010 to 2018.
Results: 57 patients (201 patient-years) with AAV were identified. They were
ANCA-positive in 44/57 (77%). GPA, EGPA and MPA was diagnosed in 18
(31,6%), 15 (26,3%), 11 (19,3%) patients, respectively. The mean age at
diagnosis was 54,5 (17,5) years. The disease itself was the main cause of
hospitalization in almost half of the hospital discharges (60/126, 47,6%). Four
patients died during the observation period due to vasculitis itself (1), pneumonia (2), or haematological malignancy (1). Time to the first event (death
or hospitalization) was significantly higher in ANCA-negative AAV patients
than in ANCA-positive AAV patients (p=0,03, Log-Rank test), ANCA-positive
AAV patients having a three-times higher risk (HR 3,38 95%CI 1,13-10,08,
p=0,03). Total estimated cost was € 1,215,078, corresponding to € 6,168
patient-year. Costs for ANCA-positive AAV patients were much higher than
those for ANCA-negative AAV patients (€ 1,115,253 vs € 99,825, and € 7058
per person-year vs € 2,559 per person-year, respectively). GPA and MPA
showed the highest costs if compared to EGPA [GPA: € 239,168 (€ 5199 per
person-year) vs MPA: € 281,502 (€ 4771 per person-year) vs EGPA: € 214,287
(2329 per person-year), respectively]. Costs for hospitalization were the highest [€ 734,957 (€ 3731 per person-year) vs other costs € 480,121 (€ 2437 per
person-year)].
Conclusion: costs for AAV are very high, confirming the high health care burden
of this illness. Management of ANCA-positive patients rather than ANCA-negative patients was burdened by the highest costs. GPA and MPA showed the
highest direct costs for hospitalization, which very frequently occurred due to the
vasculitis itself.
Disclosure of Interests: Luca Quartuccio Consultant of: Abbvie, Bristol, Speakers bureau: Abbvie, Pfizer, Elena Treppo: None declared, Salvatore De Vita Consultant of: Roche, GSK, Speakers bureau: Roche, GSK, Novartis, Francesca
Valent: None declared
DOI: 10.1136/annrheumdis-2020-eular.2585
AB0522
GENDER DIFFERENCES IN GIANT CELLS ARTERITIS:
ANALYSIS OF A MONOCENTRIC COHORT OF 100
PATIENTS.
F. Regola1, A. Tincani1, F. Franceschini1, P. Toniati1. 1ASST Spedali Civili
and University of Brescia, Rheumatology and Clinical Immunology Unit,
Brescia, Italy
Background: Giant Cells Arteritis (GCA) is the most common primary vasculitis
in adults and usually occurs in patients older than 50 years. Epidemiological
studies shown a higher prevalence of the disease in women compared to man.
However, differences in clinical presentation between men and women have not
been demonstrated, even if some distinctions have been suggested (1,2).
Objectives: The purpose of the present study is to analyze differences in the
clinical presentation of GCA according to sex.
Methods: We collected retrospectively clinical data of a monocentric cohort of
100 consecutive GCA patients. Mann Whitney test was used to compare continuous variables, while Chi-square test and Fisher’s exact test were applied for
comparison between qualitative variables.
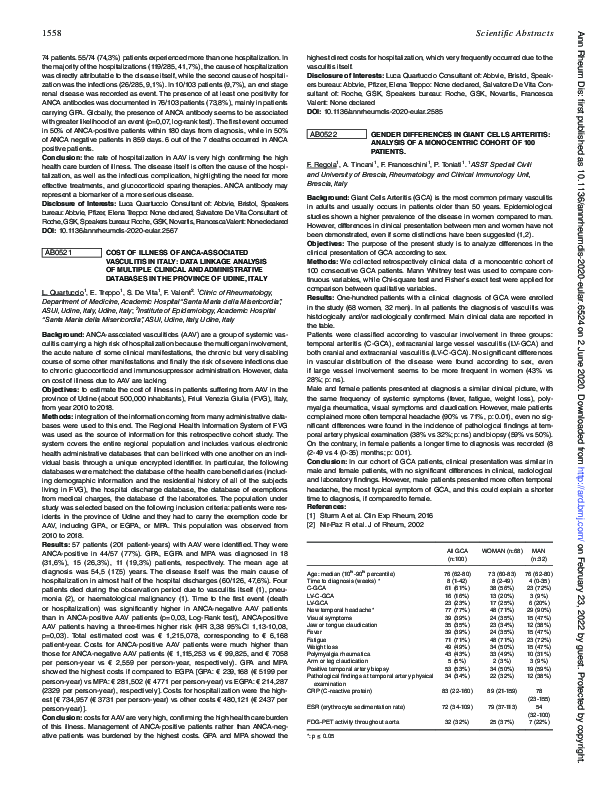
Results: One-hundred patients with a clinical diagnosis of GCA were enrolled
in the study (68 women, 32 men). In all patients the diagnosis of vasculitis was
histologically and/or radiologically confirmed. Main clinical data are reported in
the table.
Patients were classified according to vascular involvement in three groups:
temporal arteritis (C-GCA), extracranial large vessel vasculitis (LV-GCA) and
both cranial and extracranial vasculitis (LV-C-GCA). No significant differences
in vascular distribution of the disease were found according to sex, even
if large vessel involvement seems to be more frequent in women (43% vs
28%; p: ns).
Male and female patients presented at diagnosis a similar clinical picture, with
the same frequency of systemic symptoms (fever, fatigue, weight loss), polymyalgia rheumatica, visual symptoms and claudication. However, male patients
complained more often temporal headache (90% vs 71%, p: 0.01), even no significant differences were found in the incidence of pathological findings at temporal artery physical examination (38% vs 32%; p: ns) and biopsy (59% vs 50%).
On the contrary, in female patients a longer time to diagnosis was recorded (8
(2-49 vs 4 (0-35) months; p: 0.01).
Conclusion: In our cohort of GCA patients, clinical presentation was similar in
male and female patients, with no significant differences in clinical, radiological
and laboratory findings. However, male patients presented more often temporal
headache, the most typical symptom of GCA, and this could explain a shorter
time to diagnosis, if compared to female.
References:
[1] Sturm A et al. Clin Exp Rheum, 2016
[2] Nir-Paz R et al. J of Rheum, 2002
All GCA
(n:100)
WOMAN (n:68)
MAN
(n:32)
Age: median (10th-90th percentile)
Time to diagnosis (weeks) *
C-GCA
LV-C-GCA
LV-GCA
New temporal headache*
Visual symptoms
Jaw or tongue claudication
Fever
Fatigue
Weight loss
Polymyalgia rheumatica
Arm or leg claudication
Positive temporal artery biopsy
Pathological findings at temporal artery physical
examination
CRP (C-reactive protein)
76 (62-80)
8 (1-42)
61 (61%)
16 (16%)
23 (23%)
77 (77%)
39 (39%)
35 (35%)
39 (39%)
71 (71%)
49 (49%)
43 (43%)
5 (5%)
53 (53%)
34 (34%)
73 (60-83)
8 (2-49)
38 (56%)
13 (20%)
17 (25%)
48 (71%)
24 (35%)
23 (34%)
24 (35%)
48 (71%)
34 (50%)
33 (49%)
2 (3%)
34 (50%)
22 (32%)
76 (62-80)
4 (0-35)
23 (72%)
3 (9%)
6 (20%)
29 (90%)
15 (47%)
12 (38%)
15 (47%)
23 (72%)
15 (47%)
10 (31%)
3 (9%)
19 (59%)
12 (38%)
83 (22-160)
89 (21-159)
ESR (erythrocyte sedimentation rate)
72 (34-109)
79 (37-113)
32 (32%)
25 (37%)
78
(23-155)
54
(32-100)
7 (22%)
FDG-PET activity throughout aorta
*: p ≤ 0.05
Ann Rheum Dis: first published as 10.1136/annrheumdis-2020-eular.6524 on 2 June 2020. Downloaded from http://ard.bmj.com/ on February 23, 2022 by guest. Protected by copyright.
1558
�1559
Disclosure of Interests: None declared
DOI: 10.1136/annrheumdis-2020-eular.6524
TABLE 1. INITIAL CLINICAL MANIFESTATIONS
ALL THE
PATIENTS (n=34)
AB0523
TAKAYASU ARTERITIS AND SACROILIITIS: A CASECONTROL STUDY
1
2
1
1 1
F. Regola , G. Bosio , F. Franceschini , P. Toniati . ASST Spedali Civili
and University of Brescia, Rheumatology and Clinical Immunology Unit,
Brescia, Italy; 2ASST Spedali Civili of Brescia, Nuclear Medicine Unit,
Brescia, Italy
Background: A possible shared immunopathogenesis between Spondyloarthritis (SpA) and Takayasu Arteritis (TA) has been hypothesized and some clinical cases about SpA in TA patients have been reported (1). In clinical practice
the diagnosis of sacroiliitis may be performed by X-ray, Computed Tomography (CT) or Magnetic Resonance Imaging (MRI). In particular, CT findings of
sacroiliitis include contour irregularities, joint space alterations, joint erosion,
subcondral bone changes (osteoporosis or sclerosis), enthesitis, ankylosis.
Meanwhile, TA patients performe routinely FDG-PET/CT scans for monitoring
disease activity.
Objectives: This study aims to understand if there is an increased incidence of
sacroiliitis in TA patients.
Methods: We collected retrospectively imaging data from FDG-PET/CT scans of
28 TA patients and 28 controls, matched for sex and age. Controls were selected
among patients performing FDG-PET/CT in our Nuclear Medicine Unit, excluding patients with bone tumors, bone metastasis and thyroid cancers. The majority
of controls were affected by lymphoma in complete remission. An expert rheumatologist read the CT-scans of sacroiliac joints.
Results: No patients or controls demonstrated FDG-uptake in sacroiliac joints.
In the control group we detected sacroiliac sclerosis in two cases: one due to
degenerative changes, one to sacroiliitis (1/28, 4%). In the TA group four patients
presented CT alterations suggestive for sacroiliitis: one bilateral erosion, one
bilateral sclerosis, two monolateral sclerosis (4/28, 14%). One of these patients
complained an inflammatory back pain.
Conclusion: In our cohort of TA patients we demonstrated an increased prevalence of sacroiliitis, diagnosed by CT scan. Only one patient reported an
inflammatory back pain, while three patients had radiological signs of previous
sacroiliitis. These findings highlight the importance of looking for spondyloarthropathy in TA patients even if asymptomatic.
References:
[1] Guzel Esen S, Joint Bone Spine, 2019
Disclosure of Interests: None declared
DOI: 10.1136/annrheumdis-2020-eular.3940
AB0524
ANCA ASSOCIATED VASCULITIS IN GRAN CANARIA:
THE IMPORTANCE OF THE INTERSTITIAL LUNG
DISEASE
F. J. Nóvoa Medina1, F. Rubiño2, B. Tejera-Segura1, B. Romero Díaz3, S. Machín
García1, I. Rua-Figueroa2. 1Complejo Hospitalario Universitario Insular Materno
Infantil de Gran Canaria, Rheumatology, Las Palmas de Gran Canaria, Spain;
2
Hospital de Gran Canaria “Dr. Negrín”, Rheumatology, Las Palmas de Gran
Canaria, Spain; 3Complejo Hospitalario Universitario Insular Materno Infantil de
Gran Canaria, Radiology, Las Palmas de Gran Canaria, Spain
Background: ANCA-associated vasculitis (AVV) are a heterogeneous group of
systemic diseases that needs a better knowledge and approach due to the high
mortality it presents.
Objectives: Describe the clinical characteristics of patients with AAV
assessed by the Rheumatology services in two university hospitals in Gran
Canaria in the last decade, as well as clinical differences between the AAV
subtypes.
Methods: Characteristics of 34 patients diagnosed with AAV between January
2011 - December 2018 were collected retrospectively. The patients met ACR classification criteria and consensus criteria from Chapell Hill-2012. Variables are
compared using the χ2 test for dichotomous variables or the t-Student test for
continuos variables. For non-continuous variable, Mann-Whitney U or a logarithmic transformation was used
Results: 21 (61.7%) patients were women. We found 14 granulomatosis with polyangeiitis (GPA 41.2%), 10 microscopic polyangeiitis (MPA) and 10 eosinophilic
granulomatosis with polyangeiitis (EGP) (29.4%). They presented an average
follow-up time (±SD) of 46.3 months (±26.8). Patients with MPA presented an
older age at diagnosis and a higher proportion were diagnosed with age> 65
years (p = 0.003).
The mean (±SD) of the BVAS index of activity at diagnosis was 15,7 (± 7.9).
80,5% of the patients presented positivity against ANCA: 34,4% c-ANCA and
65.5% (Clinical manifestations in Table 1).
Otolaryngological involvement
Interstitial lung disease
Renal involvement
- Reno-pulmonary syndrome
- Renal Involvement
- glomerulonephritis
- Basal proteinuria >1 gr/24 hs
Alveolar pulmonary hemorrhage not
associated with renal involvement
Manifestations Peripheral Nervous
System
Cardiomyopathy
Eye involvement (scleritis/conjunctivitis/
keratitis/uveitis)
GPA
(n=14)
MPA
EGP
p
(n=10) (n=10) value
6 (17,6%)
10 (29.4%)
13(92.9%) 2(20%) 6(60%) 0.001
0
5 (50%)
0
0.027
3 (21.4%) 2 (20%) 1 (10%)
3 (21.4%) 6 (60%) 1 (10%)
13 (38.2%)
2 (5.8%)
4 (28.5%) 7 (70%) 1 (10%)
0
1 (10%) 1 (10%)
10 (29.4%)
2 (14.2%) 4 (40%) 4 (40%)
5 (14.7%)
3 (8.8%)
6 (17.6%)
0
6 (42.8%)
0
0
3 (30%)
0
0.01
21 (61.7%) patients received cyclophosphamide and 3 (8.8%) patients
received rituximab as induction treatment. Azathioprine was the most commonly used maintenance treatment (41,1%). 16 (47%) patients had renal
involvement. An improvement in proteinuria was observed, both in GPA
(p=0.008) and in MPA (p=0,03) (Renal outcomes in Table 2). No patient
received kidney transplant.
TABLE 2. RENAL OUTCOMES
Basal serum creatinine, mean (SD), mg/dl
Basal proteinuria, mean (SD), mg/dl
Last serum Creatinine, mean (SD), mg/dl
Last proteinuria, mean (SD), mg/dl
GPA (n= 6)
MPA (n=8)
p VALUE
2.07 (1.1)
2264 (1391.5)
2,2 (1.4)
485 (457.9)
3.08 (2.06)
2731.2 (1334.7)
2,1 (1.5)
326 (110.4)
0.3934
0.8348
0.5577
0.4704
Interestingly, 5 patients (14.7%), all of them MPA, presented interstitial lung
disease (ILD), 3 of them (60%) prior to systemic involvement (9, 10 and 82
months). 3 patients had an usual interstitial pneumonitis (UIP) pattern, none
had a non-specific interstitial pneumonia (NSIP) pattern and two had other
patterns.
15 patients had 17 relapses. Five (14.7%) patients had serious infections.
Eight (23.5%) patients died: 4 due to progression of ILD, 2 due to vasculitis
manifestations.
Conclusion: ILD can be considered a relatively frequent manifestation of this
group of diseases. A high percentage of patients had recurrences. Mortality
remains high in AAV and in our series ILD is a frequent cause of death.
Disclosure of Interests: Francisco Javier Nóvoa Medina Speakers bureau: I
have been paid as a speaker for a few medical talks, Francisco Rubiño: None
declared, Beatriz Tejera-Segura Speakers bureau: I have been paid as a speaker
for a few medical talks, Beatriz Romero Díaz: None declared, Sergio Machín
García: None declared, Iñigo Rua-Figueroa: None declared
DOI: 10.1136/annrheumdis-2020-eular.3268
AB0525
NATURAL HISTORY OF CRYOGLOBULINEMIA
FROM 2000 TO 2018 FROM THE LABORATORY
POINT OF VIEW: AN ANALYSIS OF CRYOGLOBULIN
CHARACTERISTICS IN A SINGLE CENTER.
G. Sandri1, A. Spinella1, P. Natali2, D. Debbia2, D. Campioli2, A. Bari3,
G. Amati1, G. Galassi4, M. Mazzoli4, G. Alfano5, F. Fontana5, T. Trenti2,
M. T. Mascia1. 1Chair and Complex Operational Unit of Rheumatology,
University of Modena and Reggio Emilia, Modena, Italy; 2Department of
Laboratory Medicine and Anatomical Pathology, AOU and AUSL of Modena,
Modena, Italy; 3Complex Structure of Oncology and Hematology, AOU of
Modena, Modena, Italy; 4Department of Neuroscience, AOU of Modena,
Modena, Italy; 5Complex Structure of Nephrology and Dialysis, AOU of
Modena, Modena, Italy
Background: Big data refers to large amounts of information. With today’s
ever-improving technologies created by the automation and digitization, it
becomes easier to convert data into relevant information, which can be used to
provide better patient management, especially when it occurs a rare condition
such as cryoglobulinemia (CRG).
CRG is due to an immunoglobulins (Ig) that precipitate at low temperatures.
There are 3 types of CRG: type I: monoclonal Ig; type II: monoclonal Ig + polyclonal Ig; type III: 2 polyclonal Ig.
Ann Rheum Dis: first published as 10.1136/annrheumdis-2020-eular.6524 on 2 June 2020. Downloaded from http://ard.bmj.com/ on February 23, 2022 by guest. Protected by copyright.
Scientific Abstracts
�
 Franco Franceschini
Franco Franceschini