Jebmh.com
Case Report
PROLONGED PATCHING AN UNCOMMON CAUSE FOR ORBITAL MYIASIS
Vaibhav Yadav1, Yusuf Rizvi2, Mohtasham Tauheed3, Atul Thadani4
13rd
Year Junior Resident, Department of Ophthalmology, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh.
Professor, Department of Ophthalmology, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh.
33rd Year Junior Resident, Department of Ophthalmology, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh.
42nd Year Junior Resident, Department of Ophthalmology, Rohilkhand Medical College and Hospital, Bareilly, Uttar Pradesh.
2Associate
HOW TO CITE THIS ARTICLE: Yadav V, Rizvi Y, Tauheed M, et al. Prolonged patching an uncommon cause for orbital myiasis.
J. Evid. Based Med. Healthc. 2019; 6(1), 61-64. DOI: 10.18410/jebmh/2019/11
PRESENTATION OF CASE
A case of orbital myiasis in a 68-year-old lady with complete
ocular destruction without co-existing systemic disorder,
immune compromise or malignancy is reported. Detailed
history revealed prolonged patching of the same eye to
subvert lagophthalmos as the precipitating factor.
Spontaneous healing & satisfactory cosmesis were observed
following maggot removal, debridement, antisepsis & oral
Ivermectin.
A 68-year-old lady from a suburban background
presented with fleshy brown foul-smelling mass in her right
eye with overlying crawling maggots. History revealed a
haemorrhagic stroke suffered by the patient 3 months back,
with subsequent left sided hemiparesis and right facial palsy.
Patient had since remained bedridden and was advised
prolonged patching of her right eye to circumvent
lagophthalmos. 15 days back, she developed severe pain in
the right eye with total loss of vision. There was a
serosanguinous discharge with a peculiar crawling sensation
in her right eyelids. There was no history of diabetes,
tuberculosis or ocular malignancy.
Figure 2. Removal of Maggots
from Eye Structures Not Identifiable
Figure 3. Live Maggots Removed
and Sent for Entomological Identification
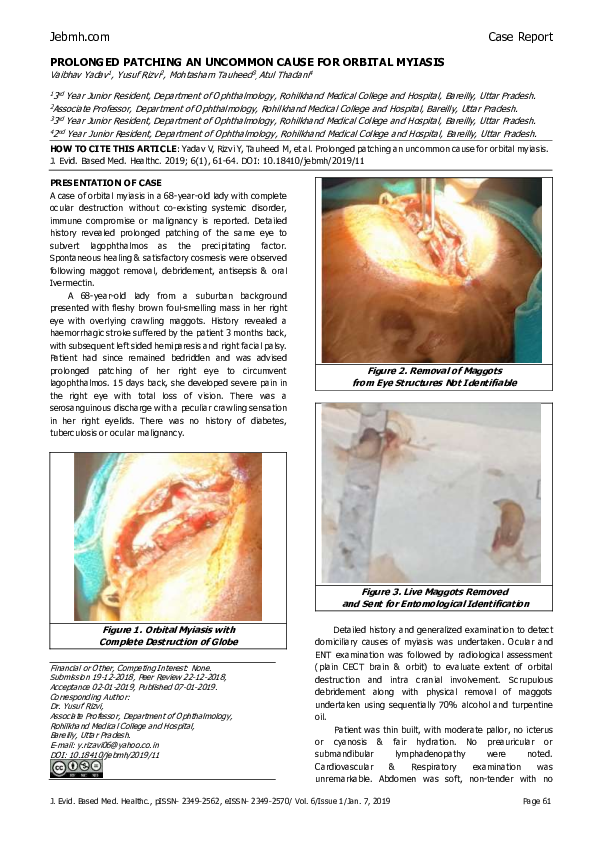
Figure 1. Orbital Myiasis with
Complete Destruction of Globe
Financial or Other, Competing Interest: None.
Submission 19-12-2018, Peer Review 22-12-2018,
Acceptance 02-01-2019, Published 07-01-2019.
Corresponding Author:
Dr. Yusuf Rizvi,
Associate Professor, Department of Ophthalmology,
Rohilkhand Medical College and Hospital,
Bareilly, Uttar Pradesh.
E-mail: y.rizavi06@yahoo.co.in
DOI: 10.18410/jebmh/2019/11
Detailed history and generalized examination to detect
domiciliary causes of myiasis was undertaken. Ocular and
ENT examination was followed by radiological assessment
(plain CECT brain & orbit) to evaluate extent of orbital
destruction and intra cranial involvement. Scrupulous
debridement along with physical removal of maggots
undertaken using sequentially 70% alcohol and turpentine
oil.
Patient was thin built, with moderate pallor, no icterus
or cyanosis & fair hydration. No preauricular or
submandibular
lymphadenopathy
were
noted.
Cardiovascular
&
Respiratory
examination
was
unremarkable. Abdomen was soft, non-tender with no
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 6/Issue 1/Jan. 7, 2019
Page 61
�Jebmh.com
hepato-splenomegaly. CNS examination revealed left sided
hemi-paresis & right sided facial paresis.
Right eye examination revealed a fungating, foul
smelling, ulcerated mass involving the whole orbit that mildly
bled on touch. Ocular structures were unidentifiable with
complete disorganisation of the tissues including eye lids.
Vision was absent.
Left eye examination was within normal limits with early
cataractous changes & an unaided vision of 6/18.
PATHOLOGICAL DISCUSSION
Hb-10.6 gm%, Total RBC count- 3.31 million/cu mm, TLC7630/cumm, BT- 2.20 min, CT- 4.0 min, Prothrombin time
14.1 sec, DLC- N82L11E04M02B1, PCV- 31.4%, Platelet Count 1.77 Lakhs/ cu mm. Urine & stool examination reports were
with in normal limits.
CECT Skull & Orbit with 5 mm axial slices revealed small
pthysical globe in right orbit with disorganized ocular tissue.
Few calcific foci were noted in the right globe. Soft tissue
thickening contiguous with right eyeball & fat stranding in
preseptal and periorbital region were noted. Soft tissue
opacification of right frontal sinus suggested sinusitis. No
infiltration of intra-cranial space or para nasal sinuses were
noted.
Figure 4. Complete Destruction of Right
Globe; No Intra Cranial Involvement Seen
Punch biopsy of orbital margin revealed lymphocytic
infiltration & erythrocytosis suggesting chronic inflammatory
changes. Malignant changes were however not detected.
Absence of fungal hyphae or spores ruled out fungal
pathology.
Myiasis is the term used to describe invasion of living
animal tissue by fly larvae or maggots.1 These larvae by
virtue of their specialized attachment hooks adhere to the
tissue while actively feeding on them. Orbital myiasis as first
reported by Keyt in 1900 describes invasion of the globe and
its adnexal structures by the feeding larvae (maggots) of
flies of various species.2 The common implicating flies are
the sheep nose botfly (Oestrus ovis), the human botfly
(Dermatobia hominis) and the Botfly of Caribou (Hypoderma
tarandi).3 More rarely infestation by Wolphartia magnifica &
Chrysomyma bezziana is reported.1,4 Proximity to these flies
Case Report
as is often observed among livestock handlers, explains
higher incidence of detection of this condition in them.
Larvae of the common housefly (Musca domestica Linnaeus)
causing external or internal ophthalmomyiasis has been
rarely reported. Association of Orbital myiasis with poor
hygiene, debility, immune-compromised status, infection
and ocular malignancy with Basal cell carcinoma in particular
are well established.5,6,7,8
Figure 5. Marked Lymphocytic Infiltration
Noted in the Excised Tissue
Ophthalmomyiasis (orbital myiasis) causes severe
ocular irritation, oedema, and pain. It is known to lead to
uveitis, glaucoma, and retinal detachment.9 Majority of case
reports however describe the condition in an advanced stage
with total destruction of globe. Basal cell carcinoma creating
an open necrotic bed for flies & maggot replication is a
common accompaniment.7,8 The clinical picture of Orbital
myiasis is governed by the causative factors, state of disease
and general health status of the individual. Often the
incursion of maggots in the live orbital tissue is masked by
fungating masses, necrotic crusts, severe oedema and
muco-purulent discharge. Frank detection of maggots is late
and may follow, only after complete destruction of globe.
The taxonomic order of true flies, Diptera is large with
an estimated 240, 000 insect species.4 The usual life cycle
of such insects goes through the stages of eggs, larvae, prepupa, pupa and adult flies, with larvae or maggots being the
feeding stage. The tremendous growth potential of larvae,
(approx. 8-10 times its size) in a matter of 4-5 days accounts
for its potential to destroy host tissue. The larvae of some
Diptera species are obligate parasites, while others are
facultative (survive both inside & outside host animal tissue).
Some species (sheep botfly or Oestrus ovis) are larviparous,
injecting larvae directly into exposed tissues such as nostril,
nasopharynx & eyes. Others are oviparous that lay eggs on
exposed necrotic tissues where the larvae hatch and migrate
inside the tissue. The housefly Musca domestica, is a fly of
the suborder Cyclorrhapha. The female housefly usually
mates once & stores the sperm for later use. Each female fly
can lay up to 500 eggs in a lifetime, in several batches of
about 75 to 150 on decaying organic matter. These soon
hatch into legless white maggots which after 2 to 5 days of
development transform into reddish-brown pupae, about 8
mm (0.3 in) long.
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 6/Issue 1/Jan. 7, 2019
Page 62
�Jebmh.com
Case Report
Figure 6. Life Cycle of Common House Fly
Compromise of periorbital tissue predisposes eye to
ocular myiasis. Such loss of vitality can be precipitated by
malignancy, ischemia, infections or surgeries.5 Orbital
myiasis has a sporadic incidence accounting for less than 5%
cases of human myiasis. Most case reports of orbital myiasis
are associated with malignant condition like basal cell
carcinoma & squamous cell carcinoma.6,10 Extreme debility,
poor hygiene, & apathy lead to destruction of orbital tissues
even in absence of malignancy.11 Prolonged patching by
causing pressure necrosis may devitalize the involved tissue.
It may also mask the early detection of maggots, hence
facilitating rapid destruction of orbital tissues and vision loss.
Broad spectrum anti parasitic drug Ivermectin facilitates in
the easy removal of maggots as has been substantiated by
other case reports.12,13 Physical dislodgement of maggots by
asphyxiating agents such as turpentine oil, alcohol, ether,
hydrogen peroxide or liquid paraffin are the mainstay of
management. Surgical debridement can be aided by
injecting 2% lidocaine into the base of the maggot eaten
cavity.
CLINICAL DIAGNOSIS
Ophthalmomyiasis?, Underlying Malignancy.
DIFFERENTIAL DIAGNOSIS
Mucormycosis
Unattended Orbital Cellulitis
Cavernous Sinus Thrombosis
Basal Cell Carcinoma
Squamous Cell Carcinoma of Eyelids
Sebaceous Gland Carcinoma
Keratoacanthoma
Lacrimal Gland Tumours
Squamous Cell Carcinoma of Maxillary Antrum
Rhinosporidiosis
DISCUSSION OF MANAGEMENT
Scrupulous debridement along with physical removal of
maggots was undertaken using 70% alcohol and turpentine
oil.
Figure 7. Debridement of Orbital
Tissue Following Maggot Removal
A single dose of Ivermectin (200 mcg/Kg) was given to
aid removal of maggots, along with a 10-day course of
systemic antibiotics & anti-inflammatory drugs. Parenteral
nutritional supplementation was added to enhance recovery.
Entomological assessment of maggots identified the larvae
as that of common housefly, ‘Musca domestica Linnaeus’.
Punch biopsy of orbital margins ruled out malignancy.
Antiseptic dressing with 5% povidone iodine & paraffin
gauze continued for a period of 3 weeks. Antibiotic powder
(neosporin) sprinkling over wound was advised on
discharge. Despite globe destruction and underlying
necrosis, fairly good healing as signalled by healthy
granulation tissue formation were noted. Satisfactory natural
cosmesis obviated need for reconstructive procedure.
Extreme debility, poor hygiene, low socioeconomic
status, proximity of domesticated animals and personal
apathy of the patient and attendants were noted as
contributory factors to orbital myiasis. An episode of partial
stroke with closure of eyelids for around a month reported 3
months back seemed as the triggering factor. The practice
of prolonged patching in old, neurologically challenged
patients with metabolic disorders increases the risk of nonhealing wounds, making such patients prone to
Ophthalmomyiasis. Orbital myiasis generally reported in
immunocompromised patients & ocular malignancy, may
present in non-pathological eyes when subjected to extreme
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 6/Issue 1/Jan. 7, 2019
Page 63
�Jebmh.com
debility & prolonged lid closure. Destructive potential of
common housefly larva is at par with other parasitic flies.
Maggot extermination, antisepsis & Ivermectin achieve fast
recovery with salvage of viable tissue and possibly vision if
detected in time.
FINAL DIAGNOSIS
Orbital Myiasis.
Figure 8. Satisfactory Cosmesis a Week Later
REFERENCES
[1] Maurya RP, Mishra D, Bhushan P, Singh VP, Singh MK.
Orbital myiasis due to invasion of larvae of flesh fly
(Wohlfartia magnifica) in a child; a rare presentation.
Case reports in Ophthalmological medicine, vol. 2012,
Article ID 371498, 2 pages, 2012. Google Scholar.
[2] Sivaramasubramaniyam
P,
Sadanand
A
V.
Ophthalmomyiasis. Brit. J. Ophthalmol. 1968; 52: 64.
[3] Reingold WJ, Robin JB, Leipa D, Kondra L, Schanzlin
DJ, Smith RE. Oestrtrus ovis ophthalmomyiasis
externa. Am J Ophthalmol. 1984; 97: 7.
Case Report
[4] Khataminia G, Aghajanzadeh R, Vazirianzadeh
BRahdar M. Orbital Myiasis. J Ophthalmic Vis Res. 2011
Jul; 6(3): 199-203
[5] Agarwal DC, Singh B. Orbital myiasis – a case report.
Ind J Ophthalmol 1990; 38: 187-8.
[6] Caca I, Unlu K, Cakmak S.S, Bilek K, Sakalar Y B, Unlu
G. Orbital myiasis: Case report. Japanese J
Ophthalmol. 2003; 47(4): 412-414
[7] Raina U K, Gupta M, Kumar V, Ghosh B, Sood R, Bodh
S. Orbital miasis in a case of invasive basal cell
carcinoma. Oman J Ophthalmol. 2009; 26(1) 41-42.
[8] Sardesai V R, Omcherry A S, Trasi S S. Ocular myiasis
with basal cell carcinoma. Indian J Dermatology. 2014.
56(3): 308-309.
[9] Masoodi M, Hosseini K. Extrnal ophthalmomyiasis
caused by sheep botfly (Oestrus ovis) larva: a case
report of 8 cases. Arch Iran Med.2004; 7: 136-139.
[10] Yeung J C C, Chung C F, Lai J S M. Orbital myiasis
complicating squamous cell carcinoma of eye lid. Hong
Kong Medical Journal. 2010; 16(1): 63-65.
[11] Sachdev M S, Harsh Kumar, Jain A K, Arora R, Dada V
K. Destructive ocular myiasis in a non-compromised
host. Indian J Ophthalmol. 1990; 38: 184-6.
[12] Osorio J, Moncada L, Molano S, Valderrama S, Gualtero
S, Franco-Paredes C. Role of Ivermectin in the
treatment of severe orbital myiasis due to Cochliomyia
hominivorax. 2006; 43(6): 57-59.
[13] Wakamatsu TH, Pierre-Filho PT. Ophthalmomyiasis
externa caused by Dermatobia hominis: a successful
treatment with oral Ivermectin. Eye (Lond) 2006; 20:
1088-1090.
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 6/Issue 1/Jan. 7, 2019
Page 64
�
 Vaibhav Yadav
Vaibhav Yadav