Lumbar Spine
Lumbar Spine
Download as pdf or txt
At a glance
Powered by AI
The document discusses joint play and packing positions of the lumbar spine, as well as special tests and anatomy related to assessing the lumbar spine and hip.
Joint play is the small amount of range of motion a therapist can passively obtain at a joint. The loose packed position is when the joint is under the least amount of stress and ligaments are most lax. The closed packed position is when the joint is under the most stress and ligaments are tightest.
Some special tests discussed include transverse vertebral pressure in flexion, extension, and side flexion as well as central vertebral pressure tests.
You might also like
- Orthopedic Physical Assessment 6e Musculoskeletal Rehabilitation Downloads Torrent PDFDocument3 pagesOrthopedic Physical Assessment 6e Musculoskeletal Rehabilitation Downloads Torrent PDFNicoleNo ratings yet
- Cat 2Document5 pagesCat 2Edgardo BivimasNo ratings yet
- 2014 Helsinki Workshop Material ShacklockDocument43 pages2014 Helsinki Workshop Material ShacklockAl100% (1)
- Rotator Cuff Tears Orthoinfo - Aaos.org TopicDocument7 pagesRotator Cuff Tears Orthoinfo - Aaos.org TopicMontserrat LandaNo ratings yet
- HIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10Document116 pagesHIp & Knee Extremity Notes Sorgenfrey Gindl 7.16.10joe joeNo ratings yet
- PHT 1261C Tests and Measurements Dr. KaneDocument17 pagesPHT 1261C Tests and Measurements Dr. Kanenico7christian100% (1)
- Exception Include Burst # of Spine, Some Lateral Wedge # and Extension Injuries of Cervical SpineDocument29 pagesException Include Burst # of Spine, Some Lateral Wedge # and Extension Injuries of Cervical Spinebhavesh jain100% (2)
- Upper Extremities Ortho SG3Document119 pagesUpper Extremities Ortho SG3Nuhu Bankwhot100% (1)
- PostureDocument2 pagesPostureNader Morris100% (1)
- Approaches To Therapeutic Exercise and Activity For NeurologicalDocument69 pagesApproaches To Therapeutic Exercise and Activity For NeurologicalPedro M. BorgesNo ratings yet
- Examination of Cervical SpineDocument39 pagesExamination of Cervical SpinedrkanthikirangNo ratings yet
- Knee, Ankle and Foot Joint MobilizationDocument17 pagesKnee, Ankle and Foot Joint MobilizationLokesh Sharma100% (1)
- 25 Congenital Scoliosis (Dr. Fazl Karam)Document45 pages25 Congenital Scoliosis (Dr. Fazl Karam)Dev ZunigaNo ratings yet
- Lumbar Spine AssessmentDocument26 pagesLumbar Spine Assessmentyoyo_pt2007100% (1)
- IvdpDocument89 pagesIvdpFelix Sabu100% (1)
- Epicondylitis, Lateral: (Tennis Elbow)Document6 pagesEpicondylitis, Lateral: (Tennis Elbow)ArieZta Kautsar RahmanNo ratings yet
- Anatomi PelvisDocument44 pagesAnatomi Pelvisari naNo ratings yet
- Lumbar Spine ExaminationDocument6 pagesLumbar Spine ExaminationSaddam Kanaan100% (1)
- Cervical SpineDocument51 pagesCervical SpineEvandiar IzwardyNo ratings yet
- Scapular DyskinesisDocument24 pagesScapular DyskinesisbarbaraNo ratings yet
- Diagnostic Palpation in Osteopathic Medi-7437305Document324 pagesDiagnostic Palpation in Osteopathic Medi-7437305MirtaNo ratings yet
- MC Kenzie: Diagnostic, Prognostic, Therapeutic, and ProphylacticDocument19 pagesMC Kenzie: Diagnostic, Prognostic, Therapeutic, and ProphylacticEvaNo ratings yet
- Passive Scapular Adduction TestDocument15 pagesPassive Scapular Adduction Testapi-468597987No ratings yet
- Case of Thoracic Outlet Syndrome - Cervical Rib: Presented and Discussed By: DR Praveen C.RDocument42 pagesCase of Thoracic Outlet Syndrome - Cervical Rib: Presented and Discussed By: DR Praveen C.RPraveen CrNo ratings yet
- Biomechanics of The Shoulder ComplexDocument83 pagesBiomechanics of The Shoulder ComplexpiciliviNo ratings yet
- CWK en DemoDocument16 pagesCWK en DemoVishal YogiNo ratings yet
- Thoracic and Lumbar Spine Anatomy: DR .S.NizamudeenDocument57 pagesThoracic and Lumbar Spine Anatomy: DR .S.NizamudeenPogo LocoNo ratings yet
- Ankylosing SpondylitisDocument19 pagesAnkylosing SpondylitisZulhida YuniNo ratings yet
- Application of Fascial Manipulation Technique in Chronic Shoulder Pain Ok PDFDocument8 pagesApplication of Fascial Manipulation Technique in Chronic Shoulder Pain Ok PDFBruno DiasNo ratings yet
- Lower Limb FracturesDocument124 pagesLower Limb Fracturesmau tau100% (1)
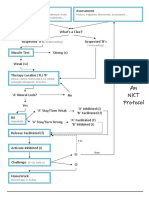
- NKT FlowChart - PDF Version 1 PDFDocument2 pagesNKT FlowChart - PDF Version 1 PDFJay SarkNo ratings yet
- Tendon Problems in Athletic IndividualsDocument15 pagesTendon Problems in Athletic IndividualsMuhammadskNo ratings yet
- 13 - Neural MobilizationDocument19 pages13 - Neural MobilizationAhmed MuflehNo ratings yet
- The Pelvis Hip Thigh Injuries of The AthleteDocument17 pagesThe Pelvis Hip Thigh Injuries of The AthleteSurgicalgownNo ratings yet
- Efficacy of Sot in FemalesDocument7 pagesEfficacy of Sot in FemalesDenise MathreNo ratings yet
- SpondylosisDocument20 pagesSpondylosisLiza Puspita SariNo ratings yet
- Physiotherapy Guidelines For Manual HyperinflationDocument5 pagesPhysiotherapy Guidelines For Manual HyperinflationAhmed Abd Elrauf100% (2)
- Examination of SpineDocument54 pagesExamination of Spinenams ortho100% (1)
- Anatomy and Pathoanatomic of Lumbosacral PlexusDocument33 pagesAnatomy and Pathoanatomic of Lumbosacral PlexusRachmad FaisalNo ratings yet
- Temporomandibular Joint DysfunctionDocument11 pagesTemporomandibular Joint Dysfunctionr.boniver524No ratings yet
- Neurobiomecanica de PelvisDocument34 pagesNeurobiomecanica de PelvisPaula Bustamante MuñozNo ratings yet
- Biomechanics of KneeDocument78 pagesBiomechanics of KneeDr. Sabari ManokaranNo ratings yet
- Special Test KNEE UnaDocument25 pagesSpecial Test KNEE Unasingle_ladyNo ratings yet
- The Painful Shoulder: Part I. Clinical Evaluation - AAFPDocument18 pagesThe Painful Shoulder: Part I. Clinical Evaluation - AAFPMelvin Florens Tania GongaNo ratings yet
- Chap2 Osteopathic ResearchDocument44 pagesChap2 Osteopathic ResearchgymwrestleNo ratings yet
- Full Spine ListingsDocument3 pagesFull Spine ListingsMatthew DriscollNo ratings yet
- Special Test of The Lower ExtremitiesDocument7 pagesSpecial Test of The Lower ExtremitiesElijah QuianoNo ratings yet
- Kozar ScienceOfMotorControlLectureDocument114 pagesKozar ScienceOfMotorControlLectureMari Pao100% (1)
- Biomechanics of The Lumbar Spine: Shira Schecter Weiner, Florian Brunner, and Margareta NordinDocument27 pagesBiomechanics of The Lumbar Spine: Shira Schecter Weiner, Florian Brunner, and Margareta NordinpkrajniNo ratings yet
- Subacromial Impingement Syndrome and Rotator Cuff Tendinopathy: The Dilemma of DiagnosisDocument4 pagesSubacromial Impingement Syndrome and Rotator Cuff Tendinopathy: The Dilemma of DiagnosisTomBramboNo ratings yet
- Genu Recurvatum SyndromDocument7 pagesGenu Recurvatum SyndromRoxana RascaNo ratings yet
- Thoracic Spine and Ribs PDFDocument334 pagesThoracic Spine and Ribs PDFSurender Dhillon0% (1)
- Spine Rehabilitation in 2022 and BeyondDocument276 pagesSpine Rehabilitation in 2022 and BeyondAhmed Abdel MoneimNo ratings yet
- Lumbar Special TestsDocument3 pagesLumbar Special TestsJesiree Dizon100% (1)
- 4) Lumbar Spinous Push Technique (Type IV), Iliomamillary PushDocument3 pages4) Lumbar Spinous Push Technique (Type IV), Iliomamillary PushNoorAkNo ratings yet
- Leg Length Discrepancy Functional Scoliosis Low Back PainDocument8 pagesLeg Length Discrepancy Functional Scoliosis Low Back PainApryana Damayanti ARNo ratings yet
- Cyriax IntroDocument14 pagesCyriax IntrodrrajmptnNo ratings yet
- Unlocking Pathways of Pain: Stories of Innovative Treatments and How They WorkFrom EverandUnlocking Pathways of Pain: Stories of Innovative Treatments and How They WorkNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Thoracic (Dorsal) SpineDocument77 pagesThoracic (Dorsal) Spineeashoor100% (3)
- 2009-2010 CCMH Study ScheduleDocument2 pages2009-2010 CCMH Study Scheduleeashoor100% (2)
- Wrist & HandDocument102 pagesWrist & Handeashoor100% (2)
- Simplifying Active Inhibition TechiquesDocument3 pagesSimplifying Active Inhibition Techiqueseashoor100% (4)
- Lesson Plan Week 12 - Main PhaseDocument5 pagesLesson Plan Week 12 - Main PhasekerryNo ratings yet
- MSK Lec #3.1 HipDocument3 pagesMSK Lec #3.1 HipCUTE ONENo ratings yet
- Acute Pelvic FracturesDocument49 pagesAcute Pelvic FracturesGustafPandyHattaNo ratings yet
- Lower Crossed SyndromeDocument11 pagesLower Crossed SyndromeJúnior Alvacir Camargo50% (2)
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument7 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- TzUpdated Low Back and Core PDFDocument8 pagesTzUpdated Low Back and Core PDFStephanie JonesNo ratings yet
- Four Phases of Parturition: Phase 1 Phase 2 Phase 3 Phase 4Document2 pagesFour Phases of Parturition: Phase 1 Phase 2 Phase 3 Phase 4Elizer Mario Pre Raboy100% (1)
- UNIVERSAL COLLEGE OF PARANAQUE. FinalsDocument26 pagesUNIVERSAL COLLEGE OF PARANAQUE. FinalsDon'tAsK TheStupidOnesNo ratings yet
- (OBQ04.162) What Is The Main Blood Supply To The Abductor Digiti Minimi?Document19 pages(OBQ04.162) What Is The Main Blood Supply To The Abductor Digiti Minimi?Yoedi YuNo ratings yet
- Sacro Occipital Techniques Category Two A Remedy For Fixated Thinking 1352662451Document7 pagesSacro Occipital Techniques Category Two A Remedy For Fixated Thinking 1352662451rcastello20100% (1)
- Gambar 3.2. Anatomi Rongga Mulut Kadal (Eutropis Multifasciata) Keterangan GambarDocument5 pagesGambar 3.2. Anatomi Rongga Mulut Kadal (Eutropis Multifasciata) Keterangan GambarrefestufuNo ratings yet
- OBGYN Clinical RotationDocument5 pagesOBGYN Clinical Rotationriczen mae vilaNo ratings yet
- Analab Skeletal Reviewer Michie PDFDocument7 pagesAnalab Skeletal Reviewer Michie PDFMichieNo ratings yet
- Anatomy, Embryology and Uterine AnomailesDocument45 pagesAnatomy, Embryology and Uterine AnomailesMesk BanatNo ratings yet
- VulvaDocument9 pagesVulvanathan100% (2)
- PeritoneumDocument8 pagesPeritoneumDavid BadaruNo ratings yet
- Lesson 2 Skeletal SystemDocument79 pagesLesson 2 Skeletal SystemLemuel CunananNo ratings yet
- Stretch An Ullustrated Step by Step Guide To 90 Slimming Yoga PosturesDocument112 pagesStretch An Ullustrated Step by Step Guide To 90 Slimming Yoga PosturesIsabelle Mullesch100% (3)
- Module 5 - MCN MaternalDocument13 pagesModule 5 - MCN MaternalChristine DuqueNo ratings yet
- Biomechanics of Side Impact: Injury Criteria, Aging Occupants, and Airbag TechnologyDocument17 pagesBiomechanics of Side Impact: Injury Criteria, Aging Occupants, and Airbag TechnologyStefanita CiunelNo ratings yet
- Lower Limb Muscles: Muscle Origin Insertion Innervation Main ActionsDocument6 pagesLower Limb Muscles: Muscle Origin Insertion Innervation Main ActionsJade Phoebe AjeroNo ratings yet
- Calisthenics UltimateDocument116 pagesCalisthenics Ultimateaalupade94100% (1)
- Pelvic Floor DysfunctionDocument92 pagesPelvic Floor DysfunctionWindy Puspa KusumahNo ratings yet
- Different of Position For Medical ExaminationDocument19 pagesDifferent of Position For Medical ExaminationQueeny Anne Apil100% (1)
- Dislocation: Muhammad ShahiduzzamanDocument30 pagesDislocation: Muhammad ShahiduzzamanAliceNo ratings yet
- Developing The Complete Hockey Off Season Program: Brijesh Patel, MA, CSCSDocument67 pagesDeveloping The Complete Hockey Off Season Program: Brijesh Patel, MA, CSCSRobinHoodCookiesNo ratings yet
- Don't Slouch! Five Exercises To Fix Bad Posture - Top - MeDocument7 pagesDon't Slouch! Five Exercises To Fix Bad Posture - Top - MeAlexander Eden Robert100% (2)
- Reproductive SystemDocument49 pagesReproductive SystemAyro Business CenterNo ratings yet
- CT/MRI Ordering Guide: Body Part Signs/Symptoms Exam To OrderDocument2 pagesCT/MRI Ordering Guide: Body Part Signs/Symptoms Exam To OrderCourtNo ratings yet
- (ANA) 4.01 Abdomen in General - Dr. ElevazoDocument22 pages(ANA) 4.01 Abdomen in General - Dr. ElevazopasambalyrradjohndarNo ratings yet