Sports Physical
Sports Physical
Download as pdf or txt
You might also like
- Pediatrics - Question Bank - RGUHSDocument51 pagesPediatrics - Question Bank - RGUHSArun Kumar88% (8)
- Colorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsDocument48 pagesColorado Revised Statutes (CRS 12 42.5) Title 12 Article 42.5 Professions and Occupations Pharmacists, Pharmacy Businesses, and PharmaceuticalsBrian HarrisNo ratings yet
- Cardiology An Illustrated Textbook (Jaypee) (PDF) (Tahir99) VRGDocument2,136 pagesCardiology An Illustrated Textbook (Jaypee) (PDF) (Tahir99) VRGGoglea Theodor94% (18)
- Case Study-Congestive Heart FailureDocument71 pagesCase Study-Congestive Heart FailureKentTangcalagan92% (13)
- Test Bank CardioDocument16 pagesTest Bank CardioLudwigJayBarayuga86% (7)
- DCFS Inspector General - Report To The Governor and The General AssemblyDocument384 pagesDCFS Inspector General - Report To The Governor and The General AssemblyNewsTeam20No ratings yet
- Open Letter To ICE From Medical Professionals Re COVID-19Document68 pagesOpen Letter To ICE From Medical Professionals Re COVID-19Jesus Garcia0% (1)
- Inmates' Lawsuit Against Allegheny County Jail (Full Text)Document60 pagesInmates' Lawsuit Against Allegheny County Jail (Full Text)jmicekNo ratings yet
- Assistance and Service Animal Request FormDocument7 pagesAssistance and Service Animal Request FormhygreevaNo ratings yet
- Parr Et Al v. Sigalas Et Al - ComplaintDocument29 pagesParr Et Al v. Sigalas Et Al - ComplaintMatthew420100% (1)
- DBS Declaration FormDocument5 pagesDBS Declaration Formakshay12489No ratings yet
- Drs. Squier and Barnes and Wisconsin Law ReportDocument80 pagesDrs. Squier and Barnes and Wisconsin Law ReportbriandocsNo ratings yet
- NLRB Denies Leslie Smith Appeal LetterDocument13 pagesNLRB Denies Leslie Smith Appeal LetterMMA PayoutNo ratings yet
- 2016-08-25 - ComplaintDocument8 pages2016-08-25 - Complaintthe kingfishNo ratings yet
- THE 24 Page Front CoverDocument246 pagesTHE 24 Page Front CoverDolan Holba100% (1)
- Homeopathic Care, Don Hamilton DVM PDFDocument48 pagesHomeopathic Care, Don Hamilton DVM PDFBibek Sutradhar0% (1)
- Lawrence Two Years Probated SuspensionDocument5 pagesLawrence Two Years Probated SuspensionAnonymous Pb39klJNo ratings yet
- Krisis HipertensiDocument12 pagesKrisis HipertensiDani NurseNo ratings yet
- Wound Assessment Tools. ReviewDocument9 pagesWound Assessment Tools. ReviewNguyễn Nhật LinhNo ratings yet
- Read Ver Tips For Drafting An Affidavit: Family Law in BC PDFDocument7 pagesRead Ver Tips For Drafting An Affidavit: Family Law in BC PDFAvelino Garchitorena Alfelor Jr.No ratings yet
- Bail Judgement 1Document57 pagesBail Judgement 1VikasNo ratings yet
- Unofficial Transcript of Oral Argument in Kitchen v. Herbert Before The Tenth Circuit Court of AppealsDocument39 pagesUnofficial Transcript of Oral Argument in Kitchen v. Herbert Before The Tenth Circuit Court of Appealsragad3199No ratings yet
- The Law of AlimonyDocument38 pagesThe Law of Alimonyshockwave4No ratings yet
- Senate Hearing, 111TH Congress - Assessing Foster Care and Family Services in The District of Columbia: Challenges and SolutionsDocument177 pagesSenate Hearing, 111TH Congress - Assessing Foster Care and Family Services in The District of Columbia: Challenges and SolutionsScribd Government DocsNo ratings yet
- Legal ResearchDocument19 pagesLegal ResearchAR ReburianoNo ratings yet
- Notice of Hearing and Motion For Relief From Stay Lenny FrolovDocument8 pagesNotice of Hearing and Motion For Relief From Stay Lenny FrolovCamdenCanaryNo ratings yet
- 10-05-01 Kids For Cash: Luzerne County Pennsylvania Vs Los Angeles County California - ABA Journal News and CommentsDocument3 pages10-05-01 Kids For Cash: Luzerne County Pennsylvania Vs Los Angeles County California - ABA Journal News and CommentsHuman Rights Alert - NGO (RA)No ratings yet
- Oca Jane Doe 072314Document3 pagesOca Jane Doe 072314Editor, Hartford CourantNo ratings yet
- Health Reform without Side Effects: Making Markets Work for Individual Health InsuranceFrom EverandHealth Reform without Side Effects: Making Markets Work for Individual Health InsuranceNo ratings yet
- Health: No Known AllergiesDocument12 pagesHealth: No Known AllergiesSeanmarie CabralesNo ratings yet
- Ex Parte Amber Lovill Tex App 13th Dist Opinion Dec 22 2008Document26 pagesEx Parte Amber Lovill Tex App 13th Dist Opinion Dec 22 2008Rick Thoma100% (1)
- Briscoe Cain Letter To School Districts On Behalf of Texans For Vaccine ChoiceDocument7 pagesBriscoe Cain Letter To School Districts On Behalf of Texans For Vaccine ChoiceBreitbartTexasNo ratings yet
- Alimony Fact SheetDocument3 pagesAlimony Fact SheetMassLiveNo ratings yet
- Army Aviation Digest - Jul 1976Document52 pagesArmy Aviation Digest - Jul 1976Aviation/Space History Library100% (1)
- Supreme Court of The United StatesDocument22 pagesSupreme Court of The United StatesForeclosure FraudNo ratings yet
- Prenatal Assessments by TrimesterDocument6 pagesPrenatal Assessments by TrimesterMauZungNo ratings yet
- Joffe Opposition To K&S Motion For Summary JudgmentDocument30 pagesJoffe Opposition To K&S Motion For Summary Judgmentabd100% (1)
- US Supreme Court Writ CertDocument119 pagesUS Supreme Court Writ CertNausheen ZainulabeddinNo ratings yet
- Plaintiff-Appellant's Brief in Support of Post-Oral Argument StatementDocument33 pagesPlaintiff-Appellant's Brief in Support of Post-Oral Argument StatementC BealeNo ratings yet
- The Tyranny of Usa Civil InjusticeDocument38 pagesThe Tyranny of Usa Civil InjusticeJoshua J. IsraelNo ratings yet
- Senate Hearing, 112TH Congress - Ending The School-To-Prison PipelineDocument855 pagesSenate Hearing, 112TH Congress - Ending The School-To-Prison PipelineScribd Government DocsNo ratings yet
- Texas Democratic Party v. Abbott 5th Circuit Opinion Granting Motion For StayDocument47 pagesTexas Democratic Party v. Abbott 5th Circuit Opinion Granting Motion For StayWashington Free Beacon100% (1)
- 4DCA Div1 Handout On WritsDocument9 pages4DCA Div1 Handout On WritsBunny FontaineNo ratings yet
- 1316096715467-Identity Cum Medical Card ApplicationDocument1 page1316096715467-Identity Cum Medical Card ApplicationMohan VadiveluNo ratings yet
- America's Lone Star Constitution: How Supreme Court Cases from Texas Shape the NationFrom EverandAmerica's Lone Star Constitution: How Supreme Court Cases from Texas Shape the NationNo ratings yet
- CFC Press Release 06-11-2008Document3 pagesCFC Press Release 06-11-2008profanejusticeNo ratings yet
- ACLU Complaint Over Riverside County Sheriff's Department CARES Act SpendingDocument5 pagesACLU Complaint Over Riverside County Sheriff's Department CARES Act SpendingThe Press-Enterprise / pressenterprise.comNo ratings yet
- Pennsylvania Mental Health Procedures Act - The Written Law Archived by Stan Caterbone On July 28, 2009Document49 pagesPennsylvania Mental Health Procedures Act - The Written Law Archived by Stan Caterbone On July 28, 2009Stan J. CaterboneNo ratings yet
- Hand Out PacketDocument26 pagesHand Out PacketEditorNo ratings yet
- Eastman Kodak ERISA LitigationDocument40 pagesEastman Kodak ERISA LitigationRochester Democrat and ChronicleNo ratings yet
- Rizona Ourt of PpealsDocument10 pagesRizona Ourt of PpealsScribd Government DocsNo ratings yet
- AMST 398 SyllabusDocument7 pagesAMST 398 SyllabusNatNo ratings yet
- Summer Study at The University of Colorado BoulderDocument1 pageSummer Study at The University of Colorado BoulderJan MarcNo ratings yet
- b50130 RPF Corruption Motion W Exhibit 1 and All Atts PDFDocument319 pagesb50130 RPF Corruption Motion W Exhibit 1 and All Atts PDFAttachment Pathology DynamicsNo ratings yet
- Murray v. Carrier, 477 U.S. 478 (1986)Document39 pagesMurray v. Carrier, 477 U.S. 478 (1986)Scribd Government DocsNo ratings yet
- Acute Abdomen During Pregnancy 2014 PDFDocument584 pagesAcute Abdomen During Pregnancy 2014 PDFlula gestiana taufan100% (1)
- May 2015 Idaho Administrative Rules BulletinDocument150 pagesMay 2015 Idaho Administrative Rules BulletinDustinHurstNo ratings yet
- Progress of The Michigan Department of Human Services Monitoring Report For Dwayne B. v. Snyder MODIFIED SETTLEMENT AGREEMENT ISSUED MARCH 10, 2014Document81 pagesProgress of The Michigan Department of Human Services Monitoring Report For Dwayne B. v. Snyder MODIFIED SETTLEMENT AGREEMENT ISSUED MARCH 10, 2014Beverly TranNo ratings yet
- 2010 US V Dominique StephensDocument51 pages2010 US V Dominique StephensJennifer WilliamsNo ratings yet
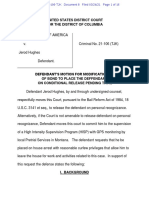
- Defendant's Motion To Place The Deffendant On Conditional Release Pending TrialDocument16 pagesDefendant's Motion To Place The Deffendant On Conditional Release Pending TrialNBC MontanaNo ratings yet
- Johnson V Johnson (2000) HCA 48 201 CLR 488 174 ALR 655 74 ALJR 1380 (7 September 2000)Document22 pagesJohnson V Johnson (2000) HCA 48 201 CLR 488 174 ALR 655 74 ALJR 1380 (7 September 2000)James JohnsonNo ratings yet
- Responsible Healthy Lifestyles: Course DescriptionDocument8 pagesResponsible Healthy Lifestyles: Course DescriptionJennifer RoyNo ratings yet
- Types of Heart DiseasesDocument4 pagesTypes of Heart DiseaseslalalallaNo ratings yet
- Heart Failure Treatment in The Intensive Care Unit in ChildrenDocument28 pagesHeart Failure Treatment in The Intensive Care Unit in ChildrenNatalia Alejandra Cardozo GomezNo ratings yet
- KanMend NMCDDocument32 pagesKanMend NMCDSincerely ReynNo ratings yet
- Dilated CardiomyopathyDocument6 pagesDilated CardiomyopathyMuthuswamyNo ratings yet
- Evolving Indications For Permanent PacemakersDocument12 pagesEvolving Indications For Permanent PacemakersJazmín Alejandra AGNo ratings yet
- Dr. Senthil Priya Heart Disease in Pregnancy FINALDocument68 pagesDr. Senthil Priya Heart Disease in Pregnancy FINALKai ParkerNo ratings yet
- Nejmlvhfabrys2022 March 2023Document11 pagesNejmlvhfabrys2022 March 2023Rahul PrasadNo ratings yet
- Cardiovascular Physical TherapyDocument206 pagesCardiovascular Physical TherapyJuanitoCabatañaLimIII100% (2)
- 1Document24 pages1Noey TabangcuraNo ratings yet
- Elective II FinalsDocument15 pagesElective II FinalsAljon Dofeliz LlamasNo ratings yet
- 2008 Device-Based Therapy of Cardiac Rhythm AbnormalitiesDocument62 pages2008 Device-Based Therapy of Cardiac Rhythm AbnormalitiesRafi UllahNo ratings yet
- Cardiology Board Review and Self Assessment A Companion Guide To Hursts The Heart Mark J Eisenberg Et Al Full ChapterDocument52 pagesCardiology Board Review and Self Assessment A Companion Guide To Hursts The Heart Mark J Eisenberg Et Al Full Chapterdouglas.zimmer226100% (21)
- CR 481Document9 pagesCR 481danielleclimacoNo ratings yet
- ICD 10 Penyakit KardiovaskularDocument20 pagesICD 10 Penyakit KardiovaskularMaya ShofiaNo ratings yet
- CardiomyopathiesDocument13 pagesCardiomyopathiesNinna Isabel VictorioNo ratings yet
- Cardiomyopathy Case StudyDocument11 pagesCardiomyopathy Case StudyJen Faye Orpilla100% (1)
- 19 Cardiac DisordersDocument51 pages19 Cardiac DisordersChessie Garcia100% (1)
- NMRF MRFDocument2 pagesNMRF MRFjoyrena ochondraNo ratings yet
- Heart Failure - A Clinical Nursing HandbookDocument273 pagesHeart Failure - A Clinical Nursing Handbookjustbeingclever100% (2)
- 118a - CardiomyopathyDocument10 pages118a - CardiomyopathyJoanna TaylanNo ratings yet
- Chapter 29 - Management of Patients With Structural, Infectious, andDocument6 pagesChapter 29 - Management of Patients With Structural, Infectious, andMichael BoadoNo ratings yet
- Pathology COMPRE2018 Finale PDFDocument79 pagesPathology COMPRE2018 Finale PDFrinkal chavdaNo ratings yet
- Miocardiopatia Periparto. NEJM, 2024Document11 pagesMiocardiopatia Periparto. NEJM, 2024susanpinky13No ratings yet
- PREP ICU 2013 Answers and Critiques - 2 - Mar & AprDocument39 pagesPREP ICU 2013 Answers and Critiques - 2 - Mar & AprNicholasHuffNo ratings yet
- Sas 13Document5 pagesSas 13Sistine Rose LabajoNo ratings yet