C 4 Kapplicationform
C 4 Kapplicationform
Download as pdf or txt
You might also like
- Food Stamps ApplicationDocument10 pagesFood Stamps ApplicationboydreamwonderNo ratings yet
- Vsf011 Form - Removal and or Inspection of A Veh at A VSFDocument2 pagesVsf011 Form - Removal and or Inspection of A Veh at A VSFTyler Beals0% (1)
- Child Dla FormDocument44 pagesChild Dla FormSamGlover0% (1)
- WWW - Humanservices.gov - Au SPW Customer Forms Resources Modjy-1211enDocument17 pagesWWW - Humanservices.gov - Au SPW Customer Forms Resources Modjy-1211enLeslie BrownNo ratings yet
- Difference Between A General Partnership and Limited PartnershipDocument7 pagesDifference Between A General Partnership and Limited PartnershipBasriJayNo ratings yet
- 03.23.20 TWW COVID 19 Stay at Home OrderDocument2 pages03.23.20 TWW COVID 19 Stay at Home OrderGovernor Tom WolfNo ratings yet
- English 13-14 App and LTRDocument5 pagesEnglish 13-14 App and LTRapi-259143520No ratings yet
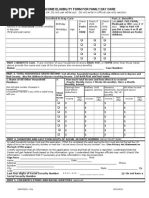
- Income Eligibility Form For Family Day CareDocument4 pagesIncome Eligibility Form For Family Day Careapi-158762543No ratings yet
- Combined Enrollment PacketDocument9 pagesCombined Enrollment PacketJustin FXNo ratings yet
- Application For AssistanceDocument13 pagesApplication For Assistanceapi-242882048No ratings yet
- Application For Health Coverage & Help Paying Costs (Short Form)Document5 pagesApplication For Health Coverage & Help Paying Costs (Short Form)Dick Díaz DelgadoNo ratings yet
- ParentApplicationLetter (Lunch)Document7 pagesParentApplicationLetter (Lunch)lakeshoreshoriansNo ratings yet
- Individual Short FormDocument5 pagesIndividual Short FormJenifer SanchezNo ratings yet
- Free and Reduced Lunch ApplicationDocument2 pagesFree and Reduced Lunch Applicationhakone9027No ratings yet
- Il444 2378BDocument14 pagesIl444 2378BKevin MccullumNo ratings yet
- CA-SingleStreamApp 66MAX 092713 With EditDocument36 pagesCA-SingleStreamApp 66MAX 092713 With EditJonihe Saul SandovalNo ratings yet
- Dss 8207 IaDocument10 pagesDss 8207 IaMaliNo ratings yet
- Free Reduced AppDocument2 pagesFree Reduced ApplakeshoreshoriansNo ratings yet
- 2013-Appendix-2 1-Child-Enrolment-FormDocument15 pages2013-Appendix-2 1-Child-Enrolment-Formapi-311470786No ratings yet
- Financial Assistance ApplicationDocument4 pagesFinancial Assistance ApplicationMulu Kindu MihretNo ratings yet
- 14-15 FR Price Program PacketDocument5 pages14-15 FR Price Program Packetapi-285638683No ratings yet
- 11-12 CCA Family Income FormDocument1 page11-12 CCA Family Income FormWilliena OwesNo ratings yet
- Packet A INVL PACKETDocument19 pagesPacket A INVL PACKETleegoodson55No ratings yet
- Myschoolapps Online Instructions EnglishDocument7 pagesMyschoolapps Online Instructions Englishgaydensdireny46No ratings yet
- IN Georgia: Division of Family and Children ServicesDocument12 pagesIN Georgia: Division of Family and Children ServicesChrisNo ratings yet
- Abcd Early Learning Application Packet: Office Use OnlyDocument11 pagesAbcd Early Learning Application Packet: Office Use OnlyrockyNo ratings yet
- 47 EnglishDocument12 pages47 Englishvannwigging41No ratings yet
- 47 EnglishDocument11 pages47 EnglishThet Thet MarNo ratings yet
- University of Pittsburgh: Financial Aid Application Supplement (FAAS) For The 2014-15 School YearDocument5 pagesUniversity of Pittsburgh: Financial Aid Application Supplement (FAAS) For The 2014-15 School YearAisha KannehNo ratings yet
- Welcome To The Kansas Food Assistance Program!: For Office Use OnlyDocument7 pagesWelcome To The Kansas Food Assistance Program!: For Office Use OnlyLars LarsonNo ratings yet
- Perdon de Pago I-912Document11 pagesPerdon de Pago I-912ChrisNo ratings yet
- Application For Calfresh Benefits (Foodstamps) Riverside County CaliforniaDocument5 pagesApplication For Calfresh Benefits (Foodstamps) Riverside County Californiawhyskeegirl131No ratings yet
- Application For Services: What Do I Need To Do To Get Benefits?Document20 pagesApplication For Services: What Do I Need To Do To Get Benefits?antasia011No ratings yet
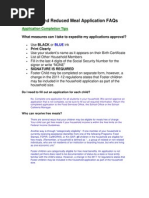
- Reduced Lunch FAQDocument4 pagesReduced Lunch FAQAnonymous 56qRCzJRNo ratings yet
- Family Preparedness PlanDocument10 pagesFamily Preparedness PlanCincinnatiEnquirerNo ratings yet
- Uniform Income & Expense Statement: Contact InformationDocument4 pagesUniform Income & Expense Statement: Contact InformationMaria ENo ratings yet
- InsuranceDocument13 pagesInsuranceelectron_rev5No ratings yet
- Change of Custody Request For Modification, Termination or Credit On ArrearsDocument6 pagesChange of Custody Request For Modification, Termination or Credit On ArrearsMaria ENo ratings yet
- NSLP App Attach BDocument2 pagesNSLP App Attach Bapi-248185821No ratings yet
- Free and Low-Cost Health Care: For Children and Pregnant WomenDocument12 pagesFree and Low-Cost Health Care: For Children and Pregnant WomenTroy RobinsonNo ratings yet
- NHJ 2016-17-Parent-Letter-And-Instructions 2Document5 pagesNHJ 2016-17-Parent-Letter-And-Instructions 2api-230493908No ratings yet
- DS700 Carer Alllowance Claim FormDocument28 pagesDS700 Carer Alllowance Claim FormHassan Mussa KhamisNo ratings yet
- HF Apponly enDocument4 pagesHF Apponly enMina Anti-barcaNo ratings yet
- How To Apply For Free and Reduced Price School MealsDocument3 pagesHow To Apply For Free and Reduced Price School MealsTracey JNo ratings yet
- Application For Assistance: Division of Welfare and Supportive ServicesDocument17 pagesApplication For Assistance: Division of Welfare and Supportive ServicesspunisphunNo ratings yet
- NHJ 2016-17-Parent-Letter-And-Instructions 2Document5 pagesNHJ 2016-17-Parent-Letter-And-Instructions 2api-230493908No ratings yet
- Maw D ApplicationDocument10 pagesMaw D ApplicationRichard GuthNo ratings yet
- HC1 ScotlandDocument20 pagesHC1 ScotlandshatakanNo ratings yet
- FSM Application 2020.202648652 3Document3 pagesFSM Application 2020.202648652 3imanomarbayoumiNo ratings yet
- 101652-Appendix B - Parents, Guardians or Sponsors 2017-18 2Document4 pages101652-Appendix B - Parents, Guardians or Sponsors 2017-18 2allen.solorzano57No ratings yet
- EbtDocument10 pagesEbtescobarjairyNo ratings yet
- Fy18 Application EnglishDocument4 pagesFy18 Application Englishapi-369657227No ratings yet
- CH2 CH3 Combined For Web EnglishDocument9 pagesCH2 CH3 Combined For Web EnglishIoana AndreeaNo ratings yet
- Health Insurance Individual Short Form (Healthcare - Gov / Obamacare)Document5 pagesHealth Insurance Individual Short Form (Healthcare - Gov / Obamacare)Joe ShopeNo ratings yet
- 04 DeterminingFamilySize enDocument47 pages04 DeterminingFamilySize enAshar AwanNo ratings yet
- Food StampsDocument4 pagesFood StampsMaliNo ratings yet
- 2023 Apprenticeship Application and Agreement January 2023Document6 pages2023 Apprenticeship Application and Agreement January 2023Danny MahomaneNo ratings yet
- Special Education: What Every Parent and Lawyer Needs to KnowFrom EverandSpecial Education: What Every Parent and Lawyer Needs to KnowNo ratings yet
- Dealing with the financial burden of Deadbeat Parents in CanadaFrom EverandDealing with the financial burden of Deadbeat Parents in CanadaNo ratings yet
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsFrom EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsNo ratings yet
- Labor Case DigestDocument2 pagesLabor Case DigestKR ReborosoNo ratings yet
- Collective Bargaining - ppt1Document15 pagesCollective Bargaining - ppt1Komal Madhan100% (1)
- LHNHS Standard Election CodeDocument10 pagesLHNHS Standard Election CodeLevi HernandezNo ratings yet
- Mizoram Lottery IssueDocument34 pagesMizoram Lottery IssuekgbijuNo ratings yet
- OSG Petition For Quo Warranto Against SerenoDocument34 pagesOSG Petition For Quo Warranto Against SerenoOffice of the Solicitor General - Republic of the Philippines100% (6)
- Taxation Review BarDocument10 pagesTaxation Review Barjemgutierrez82No ratings yet
- Indian Income Tax Return ITR-1 Sahaj: Assessment Year 2 0 18 - 1 9Document16 pagesIndian Income Tax Return ITR-1 Sahaj: Assessment Year 2 0 18 - 1 9pingbadriNo ratings yet
- Group 3: Renjith Deepthi Neethu AnithaDocument25 pagesGroup 3: Renjith Deepthi Neethu Anitharen1985mkNo ratings yet
- Supreme Court Quarterly Digest 2024 On BAIL January To March, 2024Document11 pagesSupreme Court Quarterly Digest 2024 On BAIL January To March, 2024Preet Pal SinghNo ratings yet
- Ombudsman Complaint by Head Teacher Almaira Macatanong-Bato, Et Al VERSUS DepEd-ARMM Sec. Dr. John A. Magno, Et Al.Document27 pagesOmbudsman Complaint by Head Teacher Almaira Macatanong-Bato, Et Al VERSUS DepEd-ARMM Sec. Dr. John A. Magno, Et Al.Salman Ranaw100% (1)
- Project On Injuria Sine DamnoDocument13 pagesProject On Injuria Sine DamnoAditya Singh75% (4)
- Florida v. J.L. Case BriefDocument2 pagesFlorida v. J.L. Case Brief劉映廷No ratings yet
- 18 Additional CasesDocument21 pages18 Additional CasesHassy Opaco100% (1)
- Abetment To SuicideDocument4 pagesAbetment To SuicideRITU AMARNARAYAN 1850259No ratings yet
- Indemsure - Processes and Procedures PDFDocument95 pagesIndemsure - Processes and Procedures PDFYudi SuyantoNo ratings yet
- Contract of Employment MINDSHARdEDocument2 pagesContract of Employment MINDSHARdESnooky Benitez QuisilNo ratings yet
- How To Read Court Judgments Quickly and EfficientlyDocument3 pagesHow To Read Court Judgments Quickly and EfficientlySara agrawalNo ratings yet
- PlaintDocument6 pagesPlaintAayush PandeyNo ratings yet
- CorrectionDocument24 pagesCorrectionJerome MasangyaNo ratings yet
- Imerys Talc Chapter 11 Petition - Includes List of Top 30 Plaintiff FirmsDocument26 pagesImerys Talc Chapter 11 Petition - Includes List of Top 30 Plaintiff FirmsKirk HartleyNo ratings yet
- The Law of ConfessionDocument34 pagesThe Law of ConfessionMayank Jain63% (8)
- Uttarakhand State Infrastructure Development Corporation Limited (Usidcl)Document5 pagesUttarakhand State Infrastructure Development Corporation Limited (Usidcl)ErRajivAmieNo ratings yet
- Notification Marudhara Gramin Bank Officer Scale I II III Office AssistantDocument11 pagesNotification Marudhara Gramin Bank Officer Scale I II III Office AssistantBrij Raj SahaniNo ratings yet
- Real Estate MortgageDocument2 pagesReal Estate Mortgagecristy_ingusanNo ratings yet
- Boa Syllabus RFBTDocument4 pagesBoa Syllabus RFBTAaron Joy Dominguez Putian100% (1)
- CHAVEZ vs. NHADocument54 pagesCHAVEZ vs. NHACyrusNo ratings yet
- Assignment 4 - Nagasarath PandurangiDocument6 pagesAssignment 4 - Nagasarath PandurangiNagasarath PandurangiNo ratings yet