My Case Study of Liver Cirrhosis
My Case Study of Liver Cirrhosis
Download as docx, pdf, or txt
You might also like
- Intracerebral Haemorrhage: Disease PrimersDocument18 pagesIntracerebral Haemorrhage: Disease PrimersMarlon VillanuevaNo ratings yet
- Case Study Liver CirrhosisDocument6 pagesCase Study Liver CirrhosisAngelica Barcelona Yumang67% (3)
- Surgical Case Study: CranioplastyDocument50 pagesSurgical Case Study: Cranioplastyrhia casinillo100% (8)
- CKD Case StudyDocument24 pagesCKD Case Studyapi-384366795No ratings yet
- Cholecystitis Case PresDocument103 pagesCholecystitis Case PresAnton LaurencianaNo ratings yet
- Liver Cirrhosis Case PresentationDocument146 pagesLiver Cirrhosis Case Presentationjennachristy0395% (21)
- Case Study 10 Renal FailureDocument19 pagesCase Study 10 Renal FailureAriadne Cordelette100% (2)
- Liver Cirrhosis: A Case Study OnDocument31 pagesLiver Cirrhosis: A Case Study OnCharmaine del RosarioNo ratings yet
- Case Study Liver CirrhosisDocument20 pagesCase Study Liver CirrhosisFate ZephyrNo ratings yet
- Liver Cirrhosis CaseDocument8 pagesLiver Cirrhosis Casemarlx5No ratings yet
- Liver CirrhosisDocument31 pagesLiver CirrhosisAsniah Hadjiadatu Abdullah100% (1)
- Case Study On Alcoholic Liver DiseaseDocument24 pagesCase Study On Alcoholic Liver DiseaseKristine Alejandro100% (5)
- LIVER CirrhosisDocument45 pagesLIVER CirrhosisBeRnAlie50% (4)
- Case Study On Alcoholic Liver DiseaseDocument20 pagesCase Study On Alcoholic Liver DiseaseHomework PingNo ratings yet
- Liver CirrhosisDocument76 pagesLiver Cirrhosiskathy100% (2)
- Chronic Renal FailureDocument37 pagesChronic Renal Failuredorkiebaby100% (10)
- Case Study 18Document4 pagesCase Study 18api-271284613No ratings yet
- Anatomy and Physiology-Liver CirrhosisDocument2 pagesAnatomy and Physiology-Liver CirrhosisHilmi Ramos100% (3)
- Case Liver CirrhosisDocument73 pagesCase Liver CirrhosisJesus Orita-Delima100% (1)
- Chronic Kidney Disease Case PresDocument32 pagesChronic Kidney Disease Case Presnnaesor_1091No ratings yet
- Final CholelithiasisDocument36 pagesFinal CholelithiasisRalph Pelegrino100% (2)
- Case StudyDocument7 pagesCase StudyMicah Jonah ElicañoNo ratings yet
- CHOLELITHIASISDocument46 pagesCHOLELITHIASIShttp_ugly88% (8)
- Myocardial InfarctionDocument20 pagesMyocardial Infarctionshmily_0810100% (2)
- Case Study - Septic ShockDocument16 pagesCase Study - Septic ShockIrene Mae Villanueva Ariola100% (2)
- Diabetic KetoacidosisDocument21 pagesDiabetic KetoacidosisDrishti ShresthaNo ratings yet
- Case Study On Chronic Kidney DiseaseDocument9 pagesCase Study On Chronic Kidney DiseaseHalles Beverlyn Crisostomo Geralde100% (1)
- CHOLECYSTOLITHIASISDocument77 pagesCHOLECYSTOLITHIASISMarkie ArqueroNo ratings yet
- Final Major Case StudyDocument17 pagesFinal Major Case Studyapi-546876878No ratings yet
- Diabetes Melitus 2 DkaDocument104 pagesDiabetes Melitus 2 DkaLaiza Fatima LacsonNo ratings yet
- Case Analysis FinalDocument29 pagesCase Analysis FinalVeyNo ratings yet
- Hypertension - Docx NCPDocument9 pagesHypertension - Docx NCPMarjorie BelanteNo ratings yet
- CP - Liver CirrhosisDocument161 pagesCP - Liver CirrhosisRomeo ReyesNo ratings yet
- CholedocholithiasisDocument44 pagesCholedocholithiasisGerli Bismonte100% (6)
- Case Study CholelithiasisDocument14 pagesCase Study Cholelithiasisb_faye20No ratings yet
- A Review: Nutrition in Chronic Kidney Disease PatientsDocument13 pagesA Review: Nutrition in Chronic Kidney Disease Patientsscience worldNo ratings yet
- Nursing Upper Gi BleedingDocument23 pagesNursing Upper Gi BleedingLord Pozak Miller100% (3)
- CKD - Case PresDocument29 pagesCKD - Case PresChristine Joy Ilao PasnoNo ratings yet
- Case Pre.. Cushing SyndromeDocument11 pagesCase Pre.. Cushing Syndromedee_day_8No ratings yet
- Case Study ThyroidectomyDocument8 pagesCase Study Thyroidectomyapi-347153077No ratings yet
- Final EditDocument43 pagesFinal EditMary Rose LinatocNo ratings yet
- Ulcerative ColitisDocument12 pagesUlcerative Colitisquidditch07No ratings yet
- Murari Lal Memorial School and College of Nursing, SolanDocument18 pagesMurari Lal Memorial School and College of Nursing, SolanSimran ChauhanNo ratings yet
- Case PresentationDocument31 pagesCase PresentationYogaPratayogaMNo ratings yet
- Renal Case Study Final1Document41 pagesRenal Case Study Final1api-202881815100% (1)
- Case: Liver Cirrhosis Assessment:: Nursing InferenceDocument7 pagesCase: Liver Cirrhosis Assessment:: Nursing InferenceLovelyn GanirNo ratings yet
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case Study19lyon92100% (6)
- Cholelithiasis Case StudyDocument6 pagesCholelithiasis Case StudySarah DentyNo ratings yet
- Case Study - Acute PancreatitisDocument12 pagesCase Study - Acute Pancreatitisfoe_azishan_kazaff100% (2)
- Novilyn C. Pataray Bsn-Ii Retinophathy: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray Bsn-Ii Retinophathy: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- case study حنانDocument35 pagescase study حنانMera Abo ElhassanNo ratings yet
- Liver CirrhosisDocument5 pagesLiver CirrhosisRLLTNo ratings yet
- Clinical Paper Liver CirrhosisDocument65 pagesClinical Paper Liver CirrhosisNeølie Abello LatúrnasNo ratings yet
- Case Study CholeDocument38 pagesCase Study CholeMerlene Sarmiento Salunga0% (1)
- CHOLECYSTITISDocument13 pagesCHOLECYSTITISdolly joy100% (1)
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Cirrhosis Description Highlights Causes of CirrhosisDocument18 pagesCirrhosis Description Highlights Causes of Cirrhosisen-oleNo ratings yet
- Case Study Liver CirrhosisDocument15 pagesCase Study Liver CirrhosisJester GalayNo ratings yet
- ColDocument40 pagesCol12F 24 Renu SinghNo ratings yet
- Case Study of Liver CirrhosisDocument3 pagesCase Study of Liver Cirrhosisbuzz Q100% (1)
- Liver Cirrhosis FinalDocument16 pagesLiver Cirrhosis FinalAmanda ScarletNo ratings yet
- Acute Polymorphic Psychotic Disorder With Symptoms of SchizophreniaDocument4 pagesAcute Polymorphic Psychotic Disorder With Symptoms of SchizophreniadysphileNo ratings yet
- Drug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, VecuroniumDocument12 pagesDrug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, Vecuroniumpaupaulala100% (4)
- NCP Peptic Ulcer DsDocument4 pagesNCP Peptic Ulcer Dsplug0650% (10)
- Medical Malpractice Cases: Wesleyan University-Philippines Cabanatuan City College of NursingDocument5 pagesMedical Malpractice Cases: Wesleyan University-Philippines Cabanatuan City College of NursingdysphileNo ratings yet
- Metabolites of The Ellagitannin, Geraniin Inhibit Human ACE in Vitro and in Silico EvidenceDocument9 pagesMetabolites of The Ellagitannin, Geraniin Inhibit Human ACE in Vitro and in Silico EvidencerinNo ratings yet
- Total Parenteral NutritionDocument5 pagesTotal Parenteral Nutritionankita guptaNo ratings yet
- Iferika JR Histology Slide Compilation-1Document197 pagesIferika JR Histology Slide Compilation-1ikembachinomso06No ratings yet
- Venous Thrombosis and Embolism Prevention and ManagementDocument39 pagesVenous Thrombosis and Embolism Prevention and Managementsaeed hasan saeedNo ratings yet
- Blood Pressure ChartDocument9 pagesBlood Pressure ChartVer BautistaNo ratings yet
- DOBUTamineDocument5 pagesDOBUTamineGreats HalomoanNo ratings yet
- Rosuvastatin, Aspirin and ClopidofrelDocument10 pagesRosuvastatin, Aspirin and ClopidofrelNandan GuptaNo ratings yet
- Patofisiologi Sistem KardiovaskularDocument157 pagesPatofisiologi Sistem KardiovaskularNyanmaruNo ratings yet
- ReviewDocument12 pagesReviewKarina EgurenNo ratings yet
- Patho Samplex Ratio CompiledDocument130 pagesPatho Samplex Ratio CompiledIvana BiadoNo ratings yet
- Management of Electric ShockDocument3 pagesManagement of Electric ShockAkun TBSNo ratings yet
- 1 s2.0 S1028455920301753 MainDocument4 pages1 s2.0 S1028455920301753 MainAditi SoniNo ratings yet
- HEMA PracticalDocument14 pagesHEMA PracticalNanik AndianiNo ratings yet
- Glomerulonephritis EngDocument43 pagesGlomerulonephritis EngNosirova ManijaNo ratings yet
- NSGD 2117 - Module 5 WorksheetDocument17 pagesNSGD 2117 - Module 5 Worksheetlindz.andradeNo ratings yet
- AKI in ChildrenDocument43 pagesAKI in ChildrenYonas AwgichewNo ratings yet
- Aiims Jodhpur Mega Test-17 (Fon)Document15 pagesAiims Jodhpur Mega Test-17 (Fon)Poonam Yadav roll no.53No ratings yet
- BOOST Pharm Review - Introduction To Pharm, PNS, Cardiac - ANSWERSDocument24 pagesBOOST Pharm Review - Introduction To Pharm, PNS, Cardiac - ANSWERSHwi GNDCNo ratings yet
- Approach To Acutely Ill PatientDocument22 pagesApproach To Acutely Ill PatientSarah RamliNo ratings yet
- Chapter 14 MisDocument59 pagesChapter 14 MisKeith Mark AlmarinesNo ratings yet
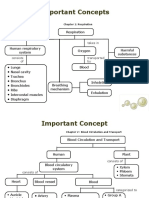
- Important ConceptsDocument6 pagesImportant ConceptscmizalpccfuNo ratings yet
- AMYLOIDOSISDocument16 pagesAMYLOIDOSISSourav NathNo ratings yet
- RESPICARDIODocument2 pagesRESPICARDIOALEJANDRO CORTEZNo ratings yet
- The Oral PresentationDocument6 pagesThe Oral PresentationCarlos MellaNo ratings yet
- Role of Bempedoic Acid in Dyslipidemia ManagementDocument13 pagesRole of Bempedoic Acid in Dyslipidemia ManagementkkkljlkjNo ratings yet
- Nervous SystemDocument28 pagesNervous Systememan el saeedNo ratings yet
- PPS-PIDSP COVID Guidelines - Ver 5 08jan2022Document20 pagesPPS-PIDSP COVID Guidelines - Ver 5 08jan2022Obree Mdn-RfnNo ratings yet
- Indications For Removal of TeethDocument27 pagesIndications For Removal of TeethMoh'dMAssufiNo ratings yet
- Funda Skills ProceduresDocument34 pagesFunda Skills Proceduresjericho obiceNo ratings yet