Myocardial Protection - An Update
Myocardial Protection - An Update
Download as pptx, pdf, or txt
You might also like
- Care Plan 5Document13 pagesCare Plan 5مالك مناصرة100% (3)
- Shahzad G. Raja - Cardiac Surgery - A Complete Guide-Springer (2020)Document1,043 pagesShahzad G. Raja - Cardiac Surgery - A Complete Guide-Springer (2020)sebaedmund1999100% (1)
- Raju B Soma Ed Clinical Methods in Cardiology PDFDocument522 pagesRaju B Soma Ed Clinical Methods in Cardiology PDFAshishsanjay Munoli50% (2)
- Haemodynamic Monitoring & Manipulation: an easy learning guideFrom EverandHaemodynamic Monitoring & Manipulation: an easy learning guideNo ratings yet
- Ventricular Septal Defect-OverviewDocument42 pagesVentricular Septal Defect-OverviewRezwanul Hoque Bulbul100% (1)
- Rheumatic Heart DiseaseDocument39 pagesRheumatic Heart DiseaseRezwanul Hoque Bulbul100% (1)
- Clinical Cases in AnesthesiaDocument539 pagesClinical Cases in AnesthesiaCamila Rodrigues Jaña100% (6)
- 2018 043 00060 FU3 - Investigator Safety Alert Letter - 1541503583 PDFDocument14 pages2018 043 00060 FU3 - Investigator Safety Alert Letter - 1541503583 PDFComan IoanaNo ratings yet
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
- Advanced Endovascular Therapy of Aortic DiseaseFrom EverandAdvanced Endovascular Therapy of Aortic DiseaseAlan B. LumsdenNo ratings yet
- The Natural and Unnatural History of Congenital Heart DiseaseFrom EverandThe Natural and Unnatural History of Congenital Heart DiseaseNo ratings yet
- Pediatric Ventricular Assist Devices: Ishlt Monograph Series Volume 11From EverandPediatric Ventricular Assist Devices: Ishlt Monograph Series Volume 11No ratings yet
- Handbook of Interventional Cardiac Procedures for Junior Cardiologists: A Summary of Current Cardiology LiteratureFrom EverandHandbook of Interventional Cardiac Procedures for Junior Cardiologists: A Summary of Current Cardiology LiteratureNo ratings yet
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationFrom EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationRating: 5 out of 5 stars5/5 (2)
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- Arterial and Venous Access in the Cardiac Catheterization Lab: Arterial and Venous Access in the Cardiac Catheterization LabFrom EverandArterial and Venous Access in the Cardiac Catheterization Lab: Arterial and Venous Access in the Cardiac Catheterization LabMazen Abu-FadelNo ratings yet
- Endovascular InterventionsFrom EverandEndovascular InterventionsJose M. WileyNo ratings yet
- Critical Decisions in Emergency and Acute Care ElectrocardiographyFrom EverandCritical Decisions in Emergency and Acute Care ElectrocardiographyNo ratings yet
- Haimovici's Vascular SurgeryFrom EverandHaimovici's Vascular SurgeryEnrico AscherNo ratings yet
- Understanding Clinical Cardiac Electrophysiology: A Conceptually Guided ApproachFrom EverandUnderstanding Clinical Cardiac Electrophysiology: A Conceptually Guided ApproachNo ratings yet
- Development, Basic Goals and Concepts in MyocardialDocument13 pagesDevelopment, Basic Goals and Concepts in MyocardialAtia KiranNo ratings yet
- Myocardial ProtectionDocument36 pagesMyocardial ProtectionRheecha JoshiNo ratings yet
- Myocardial ProtectionDocument77 pagesMyocardial Protectiondrbrdas100% (1)
- ShockDocument20 pagesShock065 Lawm SangzualiNo ratings yet
- Organ Protection Strategies For Anneurysm SurgeriesDocument12 pagesOrgan Protection Strategies For Anneurysm SurgerieslakshmiNo ratings yet
- Geriatric Anaeshtesia CopyDocument76 pagesGeriatric Anaeshtesia CopyDivya Rekha KolliNo ratings yet
- Shock Shock: DR Budi Enoch SPPDDocument31 pagesShock Shock: DR Budi Enoch SPPDRoby KieranNo ratings yet
- Shock: DR Uwanuruochi KelechukwuDocument35 pagesShock: DR Uwanuruochi KelechukwuJake MillerNo ratings yet
- Circulatory Failure (Shock) : Dr. Bernardo Dámaso MataDocument84 pagesCirculatory Failure (Shock) : Dr. Bernardo Dámaso MataDeivis Dan ErickNo ratings yet
- DocumentDocument46 pagesDocumentlintubabu0No ratings yet
- 4 Shock 2024Document100 pages4 Shock 2024rdlizuran19No ratings yet
- CVS (1) - Converted-1Document12 pagesCVS (1) - Converted-1rival ANo ratings yet
- ShockDocument21 pagesShockEdwina Naomy Octaviany SamosirNo ratings yet
- Approach To The Patient in Shock: by James Holencik, DODocument52 pagesApproach To The Patient in Shock: by James Holencik, DOLydia MamurNo ratings yet
- Shock: Dr. Naser El-Hammuri Head of The Department of Surgery Hashemite UniversityDocument40 pagesShock: Dr. Naser El-Hammuri Head of The Department of Surgery Hashemite UniversityMohammad Husni BanisalmanNo ratings yet
- Myocardial Infarction: Maj Aswathy Ganesh I Year MSC (N) Con, AfmcDocument45 pagesMyocardial Infarction: Maj Aswathy Ganesh I Year MSC (N) Con, AfmcAswathy ganeshNo ratings yet
- 4a Care of Clients in Bioliogic Crisis Shock MODSDocument35 pages4a Care of Clients in Bioliogic Crisis Shock MODSElla RoseNo ratings yet
- Crushsyndromeppt 1 200601160315Document20 pagesCrushsyndromeppt 1 200601160315Sarvarsh JanuNo ratings yet
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruNo ratings yet
- Lecture FMS 3 2015-2016 (Nata) - Pathophysiology and Pathogenesis of Shock (Restored)Document52 pagesLecture FMS 3 2015-2016 (Nata) - Pathophysiology and Pathogenesis of Shock (Restored)BritneyNo ratings yet
- Shock and BleedingDocument24 pagesShock and BleedingRaissa IcaNo ratings yet
- Seminar Shock and Metabolic Response To TraumaDocument114 pagesSeminar Shock and Metabolic Response To TraumaA. TivieanNo ratings yet
- 1) Shock/MODS/SIRS 2) Hematological Principles in SurgeryDocument56 pages1) Shock/MODS/SIRS 2) Hematological Principles in SurgeryRajarshi KumarNo ratings yet
- Shock and HemorhhageDocument84 pagesShock and HemorhhagePoova RagavanNo ratings yet
- Lecture 20 - Shock - 15 Oct 2006Document26 pagesLecture 20 - Shock - 15 Oct 2006api-3703352No ratings yet
- Shock: Deepa Murali Ms IvDocument59 pagesShock: Deepa Murali Ms Ivdee0212No ratings yet
- Seminar On Shock c2Document65 pagesSeminar On Shock c2mubarak abdulkadirNo ratings yet
- SHOCK DiscussionDocument22 pagesSHOCK DiscussionNavpreet Kaur100% (1)
- Shock-Clerk - Alif SholehenDocument20 pagesShock-Clerk - Alif Sholehenサンディリノ ペラタマNo ratings yet
- Acute Coronary Syndrome (ACS)Document39 pagesAcute Coronary Syndrome (ACS)Yowan SusantiNo ratings yet
- ShockDocument36 pagesShockJohnryan NdiranguNo ratings yet
- Shock FinalDocument90 pagesShock Finalمجاهد إسماعيل حسن حسينNo ratings yet
- DHCADocument37 pagesDHCARheecha JoshiNo ratings yet
- DR Dhiman BanikCariogenic Shock Final 2022 DDDocument59 pagesDR Dhiman BanikCariogenic Shock Final 2022 DDCloudySkyNo ratings yet
- Surgical Management of Ischemic Heart Disease - An UpdateDocument48 pagesSurgical Management of Ischemic Heart Disease - An UpdateRezwanul Hoque BulbulNo ratings yet
- Dr. Md. Rezwanul Hoque: Associate Professor Department of Cardiac Surgery BSMMU, Dhaka, BangladeshDocument48 pagesDr. Md. Rezwanul Hoque: Associate Professor Department of Cardiac Surgery BSMMU, Dhaka, BangladeshRezwanul Hoque Bulbul100% (1)
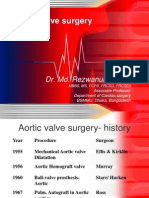
- Aortic Valve SurgeryDocument73 pagesAortic Valve SurgeryRezwanul Hoque Bulbul100% (2)
- Cardiac Pacing For The SurgeonsDocument46 pagesCardiac Pacing For The SurgeonsRezwanul Hoque BulbulNo ratings yet
- Cardiopulmonary by PassDocument62 pagesCardiopulmonary by PassRezwanul Hoque Bulbul100% (1)
- Surgical Restoration of Ventricular FunctionDocument40 pagesSurgical Restoration of Ventricular FunctionRezwanul Hoque BulbulNo ratings yet
- BSC OTAT I Year Question Bank 2022Document23 pagesBSC OTAT I Year Question Bank 2022musbira2710No ratings yet
- The A To Z of Surface AnatomyDocument236 pagesThe A To Z of Surface AnatomyAspenPharma83% (6)
- AP 10th Class Biology Bits Chapter 3 Transportation With Answers - AP Board SolutionsDocument45 pagesAP 10th Class Biology Bits Chapter 3 Transportation With Answers - AP Board Solutionsritvik.juluruNo ratings yet
- Case Questions: I. Understanding The Disease and PathophysiologyDocument8 pagesCase Questions: I. Understanding The Disease and Pathophysiologyapi-532124328No ratings yet
- Case StudyDocument5 pagesCase StudyMary Mae Boncayao50% (4)
- Coronary AngiographyDocument71 pagesCoronary AngiographyEileen del Rosario100% (2)
- The CIP (Comprehensive Integrative Puzzle) Assessment MethodDocument6 pagesThe CIP (Comprehensive Integrative Puzzle) Assessment MethodFrederico PóvoaNo ratings yet
- NCLEX Practice Exam 21 (60 Questions)Document36 pagesNCLEX Practice Exam 21 (60 Questions)Melodia Turqueza GandezaNo ratings yet
- IABP Self Study GuideDocument27 pagesIABP Self Study GuideJadie Barringer IIINo ratings yet
- Cardiovascular Nursing ReviewDocument20 pagesCardiovascular Nursing ReviewsboNo ratings yet
- Myocardial Infarction QuestionsDocument10 pagesMyocardial Infarction Questionsdsaitta108No ratings yet
- Congestive Heart FailureDocument13 pagesCongestive Heart Failureali alrashediNo ratings yet
- Biology Notes: Cie IgcseDocument64 pagesBiology Notes: Cie Igcsehamza96No ratings yet
- Tipdil Sentence CompletionDocument51 pagesTipdil Sentence CompletionYasar TepeNo ratings yet
- Medical Terminology LicentaDocument75 pagesMedical Terminology LicentaGabriel BarbarasaNo ratings yet
- Biology Project Human HeartDocument17 pagesBiology Project Human HeartdeepmanisharmaNo ratings yet
- Cheat Sheet ExamsDocument5 pagesCheat Sheet ExamsSwe LayNo ratings yet
- I. Intro To Cardio: Pericardial FluidDocument5 pagesI. Intro To Cardio: Pericardial FluidElle Ricab EnimesNo ratings yet
- AV UWorld EOs (Rough Draft) - Data - Repeat LandscapeDocument139 pagesAV UWorld EOs (Rough Draft) - Data - Repeat LandscapeJonathan AiresNo ratings yet
- Herbs - Hawthorne (Crataegus Oxyacantha)Document5 pagesHerbs - Hawthorne (Crataegus Oxyacantha)adanicNo ratings yet
- Cardiovascular Physiology Applied To Critical Care and AnesthesiDocument12 pagesCardiovascular Physiology Applied To Critical Care and AnesthesiLuis CortezNo ratings yet
- A4 QB-MC Ch08 Transport in HumansDocument23 pagesA4 QB-MC Ch08 Transport in HumansReg ChooNo ratings yet
- APK Cardiology - Pulmonology (Without Answers)Document14 pagesAPK Cardiology - Pulmonology (Without Answers)sereNo ratings yet
- LA Myxoma Case PresentationDocument34 pagesLA Myxoma Case PresentationWiwik Puji LestariNo ratings yet
- Assessment of The Human Coronary Collateral CirculationDocument11 pagesAssessment of The Human Coronary Collateral CirculationSitiMaghfirahHafizNo ratings yet