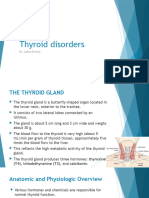
Hypothyroidism: Classification
Hypothyroidism: Classification
Download as rtf, pdf, or txt
You might also like
- Step 1 UworldDocument25 pagesStep 1 UworldKarl Abiaad100% (23)
- DR Lal Path Labs TestDocument2 pagesDR Lal Path Labs TestPIVOT GRAVITYNo ratings yet
- Thyroid Disorder in Medical Astrology - Jyotish Surfer PDFDocument40 pagesThyroid Disorder in Medical Astrology - Jyotish Surfer PDFAria AriaNo ratings yet
- Lecture 10 Protein Energy Malnutrition (PEM)Document26 pagesLecture 10 Protein Energy Malnutrition (PEM)jaish8904100% (1)
- Hashimoto's Thyroiditis InfographicDocument2 pagesHashimoto's Thyroiditis InfographicPetraNo ratings yet
- TSSM Unit 1 Exam 2018Document28 pagesTSSM Unit 1 Exam 2018nisulNo ratings yet
- 8.2hypo& HyperthyroidismDocument32 pages8.2hypo& HyperthyroidismMamatha JavvajiNo ratings yet
- HypothyridismDocument18 pagesHypothyridismanuu1404No ratings yet
- Hperthyroidism 1Document4 pagesHperthyroidism 1Salwa KaramanNo ratings yet
- HypothyroidismDocument4 pagesHypothyroidismDennis RosinNo ratings yet
- HPERTHYROIDISMDocument4 pagesHPERTHYROIDISMSalwa KaramanNo ratings yet
- Thyroid Disorders: DR Raghuveer ChoudharyDocument53 pagesThyroid Disorders: DR Raghuveer ChoudharyPhysiology by Dr RaghuveerNo ratings yet
- Endocrinology ThyroidDocument66 pagesEndocrinology ThyroidDr. Manish RamavatNo ratings yet
- HypothyroidismDocument14 pagesHypothyroidismmirmurtazarind82No ratings yet
- Group 4 - Alteration of Hormonal RegulationDocument17 pagesGroup 4 - Alteration of Hormonal RegulationMarcus KaglNo ratings yet
- What Is The Function of The Thyroid Gland?: Thyrotropin-Releasing Hormone (TRH)Document4 pagesWhat Is The Function of The Thyroid Gland?: Thyrotropin-Releasing Hormone (TRH)Jessel Mae JavierNo ratings yet
- Lecture 4Document36 pagesLecture 4tamtamtamtama0No ratings yet
- Hypothyroidis SecondaryDocument4 pagesHypothyroidis SecondaryfynneroNo ratings yet
- CVD & ThyroidDocument12 pagesCVD & ThyroidShang AllertseNo ratings yet
- Hyperthyroidism Vs Hypothyroidism: Ngmontecillo SSLC 1ST SEM 2021-2022Document76 pagesHyperthyroidism Vs Hypothyroidism: Ngmontecillo SSLC 1ST SEM 2021-2022Giovanne BuendiaNo ratings yet
- Hypothyroidism in PregnancyDocument29 pagesHypothyroidism in PregnancyhanaddulNo ratings yet
- Gabriel Chacón - ULA (VE) - Pharmacy - 1041 Physiopathology - Subject 4 - Endocrine DisordersDocument8 pagesGabriel Chacón - ULA (VE) - Pharmacy - 1041 Physiopathology - Subject 4 - Endocrine DisordersGabriel ChacónNo ratings yet
- Hashimoto Thyroiditis, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHashimoto Thyroiditis, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Oral Revalida Round 2Document63 pagesOral Revalida Round 2Mercy Anne EcatNo ratings yet
- Thyroid and ParathyroidDocument29 pagesThyroid and Parathyroidpranutan739No ratings yet
- Etiology-Hypothyroidism: Chronic Autoimmune ThyroiditisDocument4 pagesEtiology-Hypothyroidism: Chronic Autoimmune ThyroiditisNungky KusumaNo ratings yet
- Pathophysiology of EndocrinologyDocument25 pagesPathophysiology of EndocrinologyISRAELNo ratings yet
- Hypothyroidism (Underactive Thyroid) Part 1: Too Little Thyroid HormoneDocument11 pagesHypothyroidism (Underactive Thyroid) Part 1: Too Little Thyroid HormoneRex Bryan RanalanNo ratings yet
- Disorders of The Thyroid1Document22 pagesDisorders of The Thyroid1Saddamix AL OmariNo ratings yet
- PathophysiologyDocument7 pagesPathophysiologyAko Si Vern ÖNo ratings yet
- Hypothyroidism (Underactive Thyroid) - Symptoms, Causes, Tests, TreatmentsDocument9 pagesHypothyroidism (Underactive Thyroid) - Symptoms, Causes, Tests, TreatmentsHannah Denise BatallangNo ratings yet
- Hypothyroidism ConspectDocument6 pagesHypothyroidism ConspectHah LaNo ratings yet
- HypothyroidismDocument7 pagesHypothyroidismNader Smadi100% (2)
- Sumant Sharma MD CIC. Regional Lab Nejran. KKSADocument58 pagesSumant Sharma MD CIC. Regional Lab Nejran. KKSADr Sumant SharmaNo ratings yet
- HASHIMOTODocument13 pagesHASHIMOTOeogundipe61No ratings yet
- Comprehensive Review On Hypothyroid Pathophysiology Etiology ManagementDocument22 pagesComprehensive Review On Hypothyroid Pathophysiology Etiology ManagementVinod ChandraNo ratings yet
- Hyperthyroidism & HypothyroidismDocument109 pagesHyperthyroidism & Hypothyroidismmadelynmas75% (4)
- Presentation 6Document26 pagesPresentation 6555556666667777777No ratings yet
- Hyper OfficeDocument4 pagesHyper Officeshakib33001No ratings yet
- Hypothyroidism - StatPearls - NCBI BookshelfDocument10 pagesHypothyroidism - StatPearls - NCBI BookshelfKarla CordobaNo ratings yet
- Pathophysiology of HyperthyroidismDocument97 pagesPathophysiology of HyperthyroidismMarie Joyce SablanNo ratings yet
- Thyroid Disorders: Dr. Lubna DwerijDocument52 pagesThyroid Disorders: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Hashimoto S ThyroiditisDocument5 pagesHashimoto S ThyroiditisGreggy John Rivera CascayanNo ratings yet
- Thyroid EssayDocument2 pagesThyroid EssayAine Graham100% (1)
- HyperthyroidismDocument12 pagesHyperthyroidismShoppe 'n ShoppersNo ratings yet
- Effects of High TSHDocument3 pagesEffects of High TSHSreream KumarNo ratings yet
- What Is HyperthyroidismDocument7 pagesWhat Is HyperthyroidismGelo LeañoNo ratings yet
- 35thyroid DisordersDocument21 pages35thyroid DisordersDurga VoraNo ratings yet
- Laboratory Assessment of Thyroid FunctionDocument22 pagesLaboratory Assessment of Thyroid FunctionelwinrodriguezNo ratings yet
- What Is HypothyroidismDocument16 pagesWhat Is HypothyroidismvinhannyNo ratings yet
- Functions of The Thyroid GlandDocument3 pagesFunctions of The Thyroid Glandred888342193No ratings yet
- What Is HyperthyroidismDocument7 pagesWhat Is HyperthyroidismBheru LalNo ratings yet
- HipothiroidDocument27 pagesHipothiroidYuji AdityaNo ratings yet
- Yoga and Hyperthyroidism PDFDocument16 pagesYoga and Hyperthyroidism PDFRaushan Kumar MishraNo ratings yet
- EndocrinologyDocument39 pagesEndocrinologySoumyajit Ray ChaudhuriNo ratings yet
- Malfunctioning of The Thyroid GlandDocument20 pagesMalfunctioning of The Thyroid GlandonlyglorylightNo ratings yet
- Hypothyroidism: Special Types of HypothyroidismDocument4 pagesHypothyroidism: Special Types of HypothyroidismVictor VicencioNo ratings yet
- Hypothyroidism: Causes, Incidence, and Risk FactorsDocument5 pagesHypothyroidism: Causes, Incidence, and Risk FactorsPhineas KangoreNo ratings yet
- Wo Week 4 (Hyperthyroidism)Document12 pagesWo Week 4 (Hyperthyroidism)Theddyon BhenlieNo ratings yet
- Thyroid: TRH TSHDocument6 pagesThyroid: TRH TSHAjay Pal NattNo ratings yet
- Underactivity of Thyroid Gland (Hypothyroidism)Document5 pagesUnderactivity of Thyroid Gland (Hypothyroidism)Mohamed Omar SamatarNo ratings yet
- Hypothyroidism: Autoimmune DiseaseDocument3 pagesHypothyroidism: Autoimmune DiseaseAnand SwamiNo ratings yet
- Hypothyroidism, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypothyroidism, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Thyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!From EverandThyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!No ratings yet
- Nomenklatur Alat KesehatanDocument38 pagesNomenklatur Alat KesehatanYudha PrabowoNo ratings yet
- 2023 HeinWCED Life Sciences Grade 12 - JIT Session 3 - 24 May 2023.Pptx 2Document59 pages2023 HeinWCED Life Sciences Grade 12 - JIT Session 3 - 24 May 2023.Pptx 2carolmurendwaNo ratings yet
- Down Syndrome and Thyroid Disorders: A Review: 25 V. P. PrasherDocument18 pagesDown Syndrome and Thyroid Disorders: A Review: 25 V. P. PrasherErNi CiewekwekcrewetNo ratings yet
- ScienceDocument112 pagesScienceAnkit JainNo ratings yet
- Anfis Endokrin S2 (Compatibility Mode) .CompressedDocument66 pagesAnfis Endokrin S2 (Compatibility Mode) .CompressedAmiliya EmilNo ratings yet
- Group 4Document45 pagesGroup 4Nicole Juliette CCNo ratings yet
- Annex 2-2 IFU of RocheDocument4 pagesAnnex 2-2 IFU of Rocheyingchen242No ratings yet
- Basic Medical Endocrinology Fourth EditionDocument33 pagesBasic Medical Endocrinology Fourth EditionIrakanutyun ElNo ratings yet
- CLIA Acceptable Test Performance CriteriaDocument4 pagesCLIA Acceptable Test Performance CriteriaMihaelaHorgaNo ratings yet
- Endo 1.0 - FrameDocument33 pagesEndo 1.0 - FrameIshNo ratings yet
- Labreportnew 6782Document1 pageLabreportnew 6782Shahabuddin AnsariNo ratings yet
- Normal Lab Values UsmleDocument3 pagesNormal Lab Values UsmleAnne Maria50% (2)
- Thyroid HormonesDocument9 pagesThyroid Hormonesftaaa oshaNo ratings yet
- Chapter 39 Endorcrine and Reproductive SystemDocument20 pagesChapter 39 Endorcrine and Reproductive SystemgjaenNo ratings yet
- Key Points - RevisionDocument58 pagesKey Points - RevisionsophieNo ratings yet
- Med Law PerspectivesDocument3 pagesMed Law PerspectivesbiscaynediverNo ratings yet
- GCSE (9-1) Biology ExemplarsDocument51 pagesGCSE (9-1) Biology ExemplarsT-AnimeNo ratings yet
- Product Support Booklet: Lara Briden Endometriosis and PcosDocument24 pagesProduct Support Booklet: Lara Briden Endometriosis and PcosVeronica TestaNo ratings yet
- Does Ashwagandha Side EffectsDocument5 pagesDoes Ashwagandha Side Effectsnvenkatesh485No ratings yet
- Medical Lab Technician: Vocational Curriculum - 2020 2020Document64 pagesMedical Lab Technician: Vocational Curriculum - 2020 2020sm7865143No ratings yet
- Lecture Notes in Medical Technology - Lecture #5 - THYROID FUNCTION TESTSDocument14 pagesLecture Notes in Medical Technology - Lecture #5 - THYROID FUNCTION TESTSKat JornadalNo ratings yet
- Pediatrics Examination ReviewDocument224 pagesPediatrics Examination ReviewMobin Ur Rehman KhanNo ratings yet
- Pediatrics Block 2Document207 pagesPediatrics Block 2Ghada ElhassanNo ratings yet
- Nurseslabs Normal Lab Values 1.2 PDFDocument5 pagesNurseslabs Normal Lab Values 1.2 PDFPrincess BaciaNo ratings yet
- Processes Paper 1&2 Life Sciences Grade 12Document25 pagesProcesses Paper 1&2 Life Sciences Grade 12mongsterbNo ratings yet