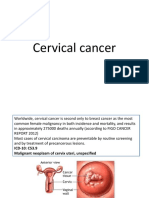
Cervical Cancer
Cervical Cancer
Download as docx, pdf, or txt
You might also like
- Reproductive Tract MalignanciesDocument30 pagesReproductive Tract Malignanciesjeelani saima100% (3)
- Cervical CancerDocument18 pagesCervical CancerErjohn Vincent LimNo ratings yet
- Description: Cervical Cancer IsDocument22 pagesDescription: Cervical Cancer IsmeanneclavioNo ratings yet
- CaseDocument5 pagesCaseBles B. MercadoNo ratings yet
- Cervical CancerDocument5 pagesCervical Cancerjinoop100% (1)
- OUTPUT SabellanoDocument18 pagesOUTPUT SabellanoNedeve OznedNo ratings yet
- Cervical Cancer: Dr. Vijay PrakashDocument23 pagesCervical Cancer: Dr. Vijay PrakashVijay PrakashNo ratings yet
- Cervical Cancer FactsDocument4 pagesCervical Cancer FactsRamy AsollaremNo ratings yet
- En Dome Trial CancerDocument2 pagesEn Dome Trial CancerJaymeeNo ratings yet
- Gynaecological CancersDocument4 pagesGynaecological CancerssdfNo ratings yet
- Cervical CancerDocument36 pagesCervical CancerDebabrata SatapathyNo ratings yet
- RRLDocument6 pagesRRLsheenayeahNo ratings yet
- Symptoms: Definition of Cervical Cancer: Cancer That Forms in Tissues of The Cervix (The Organ Connecting The UterusDocument5 pagesSymptoms: Definition of Cervical Cancer: Cancer That Forms in Tissues of The Cervix (The Organ Connecting The UterusHazel Joy Hokson-DiazNo ratings yet
- Newest Cervical CancerDocument14 pagesNewest Cervical CancerSAMMYNo ratings yet
- Cervical CancerDocument7 pagesCervical CancerChristine Joy Clemente BerjaNo ratings yet
- Cervical Cancer - A Global Health CrisisDocument9 pagesCervical Cancer - A Global Health Crisispb.nakulaNo ratings yet
- Low Risk of Cervical Cancer Precancer Among Most.3Document11 pagesLow Risk of Cervical Cancer Precancer Among Most.3Yosie Yulanda PutraNo ratings yet
- Milla Kviatkovsky, OMS-III, April 2013Document23 pagesMilla Kviatkovsky, OMS-III, April 2013api-210786702No ratings yet
- KarsinomaDocument12 pagesKarsinomaWahyudi Pratama HarliNo ratings yet
- Ovarian Cancer Research PaperDocument8 pagesOvarian Cancer Research PapershaunNo ratings yet
- Cervical Cancer Prevention and Early DetectionDocument28 pagesCervical Cancer Prevention and Early DetectionTriponiaNo ratings yet
- Kanker ServiksDocument13 pagesKanker ServiksVhiaLiviaNo ratings yet
- Cervical DysplasiaDocument10 pagesCervical DysplasiaJaweria ShujaatNo ratings yet
- Cervical Cancer: Prevention and Early DetectionDocument28 pagesCervical Cancer: Prevention and Early DetectionAnisha Puspa MelatiNo ratings yet
- Cervical Cancer: Kepaniteraan Klinik Bagian Obstetri Ginekologi FK Uns / Rsud Dr. Moewardi SurakartaDocument28 pagesCervical Cancer: Kepaniteraan Klinik Bagian Obstetri Ginekologi FK Uns / Rsud Dr. Moewardi SurakartaobsgynNo ratings yet
- Proiect EnglezaDocument20 pagesProiect EnglezaRenata BendeNo ratings yet
- tmpF425 TMPDocument8 pagestmpF425 TMPFrontiersNo ratings yet
- Endometrial CancerDocument31 pagesEndometrial CancerabtewdralehegnNo ratings yet
- Thesis Statement On Cervical CancerDocument6 pagesThesis Statement On Cervical Cancerbkx3abyc100% (2)
- Cervical CancerDocument23 pagesCervical CancerShinal Chand100% (1)
- Cervical CancerDocument2 pagesCervical CancerLicio LentimoNo ratings yet
- Cervical CancerDocument27 pagesCervical CancerHanif RezaNo ratings yet
- Colposcopy: Prof. M. AddarDocument58 pagesColposcopy: Prof. M. AddarAvnish KumarNo ratings yet
- Cervical Cancer: Emedicine Specialties Obstetrics and Gynecology Gynecologic OncologyDocument19 pagesCervical Cancer: Emedicine Specialties Obstetrics and Gynecology Gynecologic OncologyFatah Abdul YasirNo ratings yet
- Cervical Cancer What Is Cervical Cancer?Document16 pagesCervical Cancer What Is Cervical Cancer?Angeli LambinoNo ratings yet
- OBGYN Invasive Cervical Cancer ArticleDocument7 pagesOBGYN Invasive Cervical Cancer ArticleVanessa HermioneNo ratings yet
- CERVICAL CANCER SeminarDocument15 pagesCERVICAL CANCER SeminarAkinsoun MotunrayoNo ratings yet
- Cervical CancerDocument7 pagesCervical CancerLarisse de LeonNo ratings yet
- Cervical Cancer PresentationDocument25 pagesCervical Cancer PresentationRinjaya Teguh100% (1)
- Premalignant Lesions of The Uterine Cervix - Sundhed - DKDocument7 pagesPremalignant Lesions of The Uterine Cervix - Sundhed - DKPavel BerlinschiNo ratings yet
- Clinical Evaluation of The BreasDocument6 pagesClinical Evaluation of The BreasSalim Mwiti NabeaNo ratings yet
- Iva Screening2Document9 pagesIva Screening2ponekNo ratings yet
- Risk Factors: About Breast CancerDocument5 pagesRisk Factors: About Breast CancerShyamol Bose100% (1)
- Endometrialcancer 181007003100Document49 pagesEndometrialcancer 181007003100abdulghaniNo ratings yet
- Cancer Cervix: BY Ahmed Magdy ElmohandesDocument34 pagesCancer Cervix: BY Ahmed Magdy ElmohandesAhmed ElmohandesNo ratings yet
- Colposcopy: Cervical Cancer Is Cancer of The Cervix (Lowermost Opening of The Uterus in TheDocument4 pagesColposcopy: Cervical Cancer Is Cancer of The Cervix (Lowermost Opening of The Uterus in TheMayuri SwamiNo ratings yet
- ObGyn Secrets, 3rDocument1 pageObGyn Secrets, 3rCahyadi PangemananNo ratings yet
- Cervix Uteri1Document5 pagesCervix Uteri1twiggy484No ratings yet
- Intl J Gynecology Obste - 2021 - Adams - Cancer of The Vagina 2021 Update 2Document9 pagesIntl J Gynecology Obste - 2021 - Adams - Cancer of The Vagina 2021 Update 2mintunlananobgynNo ratings yet
- Pap IntroductionDocument390 pagesPap IntroductionAnish VeettiyankalNo ratings yet
- Benign Breast Disorders+++Document16 pagesBenign Breast Disorders+++Fernando Peralta PalmezanoNo ratings yet
- Screening For Ovarian CancerDocument12 pagesScreening For Ovarian CancerKerlyn GuerraNo ratings yet
- Types of Ovarian CancerDocument5 pagesTypes of Ovarian Cancerوسام وميض عبدالله CNo ratings yet
- Tumor PayudaraDocument53 pagesTumor PayudaraBeivyNo ratings yet
- Ovarian Cancer - StatPearls - NCBI BookshelfDocument13 pagesOvarian Cancer - StatPearls - NCBI BookshelfeeeeeeNo ratings yet
- Intl J Gynecology Obste - 2021 - AdamsDocument9 pagesIntl J Gynecology Obste - 2021 - AdamsKalaivathanan VathananNo ratings yet
- Review Article: Ovarian Cancer Pathogenesis: A Model in EvolutionDocument13 pagesReview Article: Ovarian Cancer Pathogenesis: A Model in Evolutionn2763288No ratings yet
- Cervical Cancer ESMODocument12 pagesCervical Cancer ESMOAndrei CorhaNo ratings yet
- Cervical Cancer: A Comprehensive Resource for Patients and FamiliesFrom EverandCervical Cancer: A Comprehensive Resource for Patients and FamiliesNo ratings yet
- Accelerating Cervical Cancer Control and PreventionDocument2 pagesAccelerating Cervical Cancer Control and Preventionderr barrNo ratings yet
- Copan Flock Tech BrochureDocument8 pagesCopan Flock Tech BrochuremohdkhairNo ratings yet
- Vulva NeoplasmDocument40 pagesVulva NeoplasmAyuw AgustrianiNo ratings yet
- Brosur KIT HPV DNADocument2 pagesBrosur KIT HPV DNARonna EfriyanaNo ratings yet
- Introduction To Biotechnology PDFDocument39 pagesIntroduction To Biotechnology PDFFitaSucia100% (1)
- Assigned Reading - Human PapillomavirusesDocument4 pagesAssigned Reading - Human Papillomavirusestheodore_estradaNo ratings yet
- Oral Viral Infections Diagnosis and Management PDFDocument13 pagesOral Viral Infections Diagnosis and Management PDFWesley Rodrigues100% (1)
- B) Reassurance That This Is Normal InitiallyDocument51 pagesB) Reassurance That This Is Normal InitiallygofisheeNo ratings yet
- Microbiology II - VirologyDocument8 pagesMicrobiology II - Virologyangel mintsNo ratings yet
- Viral Wart - DermNet NZDocument6 pagesViral Wart - DermNet NZMudassar SattarNo ratings yet
- Chapter 3.2 The Sexual SelfDocument62 pagesChapter 3.2 The Sexual SelfVhallerie joy CalpitoNo ratings yet
- Factors Associated With Human Papillomavirus Related Stigma, Shame, and Intent of HPV TestDocument9 pagesFactors Associated With Human Papillomavirus Related Stigma, Shame, and Intent of HPV TestChiboyKrenzNo ratings yet
- (Current Cancer Research) Erle S. Robertson - Microbiome and Cancer-Springe PDFDocument406 pages(Current Cancer Research) Erle S. Robertson - Microbiome and Cancer-Springe PDFmariomg100% (1)
- Causes and Symptoms & The Oral Cancer ExamDocument4 pagesCauses and Symptoms & The Oral Cancer ExamAndykaYayanSetiawanNo ratings yet
- Written Report: Sexually Transmitted Infections (Stis)Document3 pagesWritten Report: Sexually Transmitted Infections (Stis)Paul Michael B. VillanuevaNo ratings yet
- Distribuţia Genotipurilor Virusului Papiloma Uman La Paciente Din Zona MoldoveiDocument5 pagesDistribuţia Genotipurilor Virusului Papiloma Uman La Paciente Din Zona MoldoveiZama VitalieNo ratings yet
- HSTP II HMIS Hospital Heath Centre and Health PostDocument367 pagesHSTP II HMIS Hospital Heath Centre and Health PostDagmawitNo ratings yet
- Pap SmearDocument4 pagesPap SmearRamy AsollaremNo ratings yet
- Lesson Plan - HPVDocument6 pagesLesson Plan - HPVMonique MavronicolasNo ratings yet
- Influence of Morinda Citrifolia (Noni) On Expression of DNA Repair Genes in Cervical Cancer CellsDocument5 pagesInfluence of Morinda Citrifolia (Noni) On Expression of DNA Repair Genes in Cervical Cancer CellsAtika Nur NabilaNo ratings yet
- Virus Papiloma Humano y Cáncer Cérvico-Uterino: Papillomavirus and Cervical Cancer in ChileDocument4 pagesVirus Papiloma Humano y Cáncer Cérvico-Uterino: Papillomavirus and Cervical Cancer in ChileAnonymous QV38xzhceNo ratings yet
- Anti Same Sex MarriageDocument3 pagesAnti Same Sex MarriageMaria Juliana ESTEVESNo ratings yet
- @MBS MedicalBooksStore 2020 HeadDocument238 pages@MBS MedicalBooksStore 2020 HeadtamiNo ratings yet
- AbizhaDocument163 pagesAbizhaSrideviRaviNo ratings yet
- Malignant Diseases of The CervixDocument128 pagesMalignant Diseases of The Cervixnicewan0% (1)
- WLP - Q1 - W4 - Als SEPT 25 28 2023 EXODUESDocument13 pagesWLP - Q1 - W4 - Als SEPT 25 28 2023 EXODUESRicardo De GuzmanNo ratings yet
- Assessment of An Educational Intervention To Increase Knowledge ADocument146 pagesAssessment of An Educational Intervention To Increase Knowledge AHimanshu ShahNo ratings yet
- STD PRESENTATIONDocument89 pagesSTD PRESENTATIONKaarthigan RamaiahNo ratings yet
- Young Adults Awareness and Knowledge of Human Papillomavirus orDocument117 pagesYoung Adults Awareness and Knowledge of Human Papillomavirus orHimanshu ShahNo ratings yet
- Consumer Information CatalogDocument16 pagesConsumer Information CatalogAnonymous YcGbGGsMYNo ratings yet