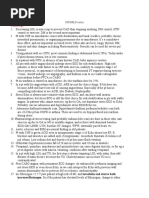
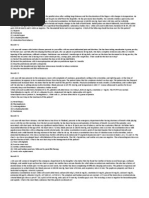
PracticeExam CCS
PracticeExam CCS
Download as doc, pdf, or txt
You might also like
- Risk Factors & Prognosis For USMLE STEP 3 PDFDocument182 pagesRisk Factors & Prognosis For USMLE STEP 3 PDFSadia Ghani100% (1)
- USMLE Step 3 CCS in ShortDocument4 pagesUSMLE Step 3 CCS in ShortPraneeth Reddy100% (7)
- Step 3 NBME Form 1Document58 pagesStep 3 NBME Form 1Sadia Ghani100% (8)
- CCS Cases NotesDocument12 pagesCCS Cases NotesMandeep100% (1)
- Step 3 CCS Mnemonics... NEW..Document1 pageStep 3 CCS Mnemonics... NEW..madiha85% (13)
- Bio-Stats Step 3Document9 pagesBio-Stats Step 3S100% (4)
- USMLE Step 3 CCS NotesDocument20 pagesUSMLE Step 3 CCS Notesaustinhitz96% (28)
- Step 3 Form 3 CorrectedDocument41 pagesStep 3 Form 3 CorrectedSBG BPT100% (2)
- SURVIVOR'S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 2CK.From EverandSURVIVOR'S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 2CK.Rating: 5 out of 5 stars5/5 (1)
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1Rating: 5 out of 5 stars5/5 (2)
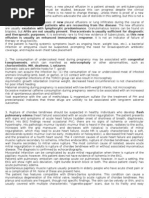
- Summary of Consensus Statements On The Diagnosis and Management of COPD in The PhilippinesDocument34 pagesSummary of Consensus Statements On The Diagnosis and Management of COPD in The PhilippinesDivye GuptaNo ratings yet
- UWorld Step 3 NotesDocument91 pagesUWorld Step 3 Noteshellayeah86% (7)
- Uworld Step 3 NotesDocument59 pagesUworld Step 3 Noteskeyurb100% (1)
- CCS Cases TemplateDocument7 pagesCCS Cases TemplatesaraatifNo ratings yet
- USMLE Epidemiology BiostatsDocument1 pageUSMLE Epidemiology BiostatsSylvia Gonzalez100% (1)
- PracticeExam 3 AnsDocument52 pagesPracticeExam 3 AnsBehrouz YariNo ratings yet
- Step 3 CCS OutlineDocument10 pagesStep 3 CCS OutlineDuncan Jackson100% (2)
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Ccs Tips Step 3Document18 pagesCcs Tips Step 3JMi Grca Pbla100% (6)
- How To Get The Highest Score On The USMLE Step 3. Strategy.: Alex - Babak - LiveJournalDocument14 pagesHow To Get The Highest Score On The USMLE Step 3. Strategy.: Alex - Babak - LiveJournalcoralkaoma100% (4)
- Usmle CCSDocument224 pagesUsmle CCSShane Allen100% (7)
- UW Qbank Step-3 MWDocument513 pagesUW Qbank Step-3 MWSukhdeep Singh88% (8)
- Arlete's Notes For Step 3 - USMLE ForumsDocument14 pagesArlete's Notes For Step 3 - USMLE ForumsWyz Class100% (3)
- Friends Ccs CasesDocument23 pagesFriends Ccs Casesvivekmo100% (2)
- Musa 100 Rules For Step 3 CCSDocument4 pagesMusa 100 Rules For Step 3 CCSHaroon Ahmed100% (7)
- Step 3 Lecture Notes - CompleteDocument834 pagesStep 3 Lecture Notes - CompletetreezeeMD100% (4)
- Biostatistics Step 3 NotesDocument17 pagesBiostatistics Step 3 Notesrsimranjit100% (1)
- Step 3 DiagramDocument11 pagesStep 3 DiagramJorge Luis Lopez100% (2)
- ERAS - Personal StatementDocument1 pageERAS - Personal StatementfewNo ratings yet
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3Rating: 5 out of 5 stars5/5 (1)
- Strategies for the MCCQE Part II: Mastering the Clinical Skills Exam in CanadaFrom EverandStrategies for the MCCQE Part II: Mastering the Clinical Skills Exam in CanadaNo ratings yet
- Respiratory System QuestionsDocument8 pagesRespiratory System Questionschristine_8995No ratings yet
- Tobacco Lesson PlanDocument4 pagesTobacco Lesson Planapi-240857737No ratings yet
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Ccs InfoDocument13 pagesCcs Info786ss100% (1)
- Skan's Step 3 CocktailDocument82 pagesSkan's Step 3 CocktailVS100% (6)
- Step 3 Experience With CCS TipsDocument6 pagesStep 3 Experience With CCS TipsDiorella Marie López González100% (4)
- Tips USMLE Step 3Document2 pagesTips USMLE Step 3mnigam64100% (1)
- Archer Step 3 CCSDocument62 pagesArcher Step 3 CCSJMi Grca Pbla100% (10)
- L LocationDocument2 pagesL LocationZee MirzaNo ratings yet
- Drsanchana: Kaplan Step 2 CK Lecture Notes 2011-12Document10 pagesDrsanchana: Kaplan Step 2 CK Lecture Notes 2011-12palak320% (1)
- HY Pearls From UWorld Step3 PDFDocument91 pagesHY Pearls From UWorld Step3 PDFJohn Smith100% (1)
- Step 3 Sample Questions 2015Document41 pagesStep 3 Sample Questions 2015yepherenow100% (2)
- 41 Practice Cases (Version 2 - Better Version)Document23 pages41 Practice Cases (Version 2 - Better Version)Mohammad GhaniNo ratings yet
- Surgery Notes For The USMLE Step 3 ExamDocument13 pagesSurgery Notes For The USMLE Step 3 ExamsaraatifNo ratings yet
- CCS RheumatologyDocument3 pagesCCS RheumatologyMostafa Mahmoud ElsebeyNo ratings yet
- Step 3 CCS OutlineDocument10 pagesStep 3 CCS OutlineRyan Turner100% (1)
- Step 3 NotesDocument4 pagesStep 3 Notesjhk0428No ratings yet
- Uw Ccs Blog CasesDocument5 pagesUw Ccs Blog Cases808kailuaNo ratings yet
- My Overview: Preparation Resources 1. USMLE Free Practice QuestionsDocument4 pagesMy Overview: Preparation Resources 1. USMLE Free Practice Questionsmnigam64No ratings yet
- An Insight Into Step 3Document4 pagesAn Insight Into Step 3Spencer0% (1)
- 50 Star Ccs Cases - USMLE ForumsDocument43 pages50 Star Ccs Cases - USMLE ForumsAbia Izzeldin Kamil100% (1)
- Dokumen - Tips Usmle Step 3 Essestial ObgynDocument10 pagesDokumen - Tips Usmle Step 3 Essestial ObgynMuhammad AbubakarNo ratings yet
- Sports MedicineDocument32 pagesSports Medicinersimranjit100% (1)
- Arlete S Notes PDFDocument28 pagesArlete S Notes PDFjrabeNo ratings yet
- Master the Physician Assistant National Recertifying Exam (PANRE)From EverandMaster the Physician Assistant National Recertifying Exam (PANRE)No ratings yet
- Beyond Residency: The New Physician’s Guide to the Practice of MedicineFrom EverandBeyond Residency: The New Physician’s Guide to the Practice of MedicineRating: 3.5 out of 5 stars3.5/5 (2)
- Back to Zero: FNP Board Review NotesFrom EverandBack to Zero: FNP Board Review NotesRating: 5 out of 5 stars5/5 (3)
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- PANCE (Physician Assistant Nat. Cert Exam) Flashcard BookFrom EverandPANCE (Physician Assistant Nat. Cert Exam) Flashcard BookRating: 1.5 out of 5 stars1.5/5 (4)
- Practice Exam 4Document94 pagesPractice Exam 4Debo AdeosoNo ratings yet
- PracticeExam 4 QsDocument17 pagesPracticeExam 4 QsBehrouz YariNo ratings yet
- PracticeExam 3 QsDocument17 pagesPracticeExam 3 QsBehrouz YariNo ratings yet
- PracticeExam 2 AnsDocument51 pagesPracticeExam 2 AnsBehrouz YariNo ratings yet
- PracticeExam 2 QsDocument24 pagesPracticeExam 2 QsBehrouz YariNo ratings yet
- PracticeExam 1 QsDocument16 pagesPracticeExam 1 QsBehrouz YariNo ratings yet
- Practice Exam 1Document103 pagesPractice Exam 1aayceeNo ratings yet
- Farmakoterapi PPOK PDFDocument61 pagesFarmakoterapi PPOK PDFElizabeth SniderNo ratings yet
- Health 8 Fourth QuarterDocument19 pagesHealth 8 Fourth QuarterAbcde FghijkNo ratings yet
- Lung Ultrasound Made Easy Step-By-Step GuideDocument48 pagesLung Ultrasound Made Easy Step-By-Step GuideEL SHITA100% (1)
- AARC Clinical Practice Guideline - Pulmonary RehabilitationDocument9 pagesAARC Clinical Practice Guideline - Pulmonary RehabilitationCristina CamachoNo ratings yet
- Oxygen Therapy Learning Module Cat 1and2Document62 pagesOxygen Therapy Learning Module Cat 1and2Baha'aeddin HammadNo ratings yet
- Istan Respiratory Deleted Learner)Document2 pagesIstan Respiratory Deleted Learner)Brandie StrangeNo ratings yet
- Ventolin PPT ADocument14 pagesVentolin PPT AZiaulNo ratings yet
- Board Exam Compilation Book 2Document163 pagesBoard Exam Compilation Book 2Aaron Cy Untalan100% (6)
- Administering Oxygen Therapy Powerpoint 3Document58 pagesAdministering Oxygen Therapy Powerpoint 3reema_rt80% (10)
- A Disease of The Blood Vessels Characterized by The Deposition of Fats and Cholesterol Within The Walls of The ArteryDocument6 pagesA Disease of The Blood Vessels Characterized by The Deposition of Fats and Cholesterol Within The Walls of The ArteryLongyapon Sheena Stephanie50% (2)
- 06 Offline Module CourseDocument15 pages06 Offline Module CourseDylan Angelo AndresNo ratings yet
- 00547-2020 Full PDFDocument56 pages00547-2020 Full PDFirmaNo ratings yet
- 2016 - July Confidential Cures NL FinalDocument22 pages2016 - July Confidential Cures NL Finalemagoo100% (1)
- Assignment Ratio Respi FluidDocument12 pagesAssignment Ratio Respi FluidsenyorakathNo ratings yet
- Support GRP Lungs Centre Copd - BrochureDocument2 pagesSupport GRP Lungs Centre Copd - BrochureDivye GuptaNo ratings yet
- FormularyDocument190 pagesFormularyMahesh T MadhavanNo ratings yet
- Research Paper1Document16 pagesResearch Paper1Tonet Salago CantereNo ratings yet
- PediatricsDocument87 pagesPediatricsCarlos HernándezNo ratings yet
- Hse Guidance Document On Pulmonary RehabilitationDocument48 pagesHse Guidance Document On Pulmonary RehabilitationeimearNo ratings yet
- Efficacy of Pursed-Lips Breathing: A Breathing Pattern Retraining Strategy For Dyspnea ReductionDocument8 pagesEfficacy of Pursed-Lips Breathing: A Breathing Pattern Retraining Strategy For Dyspnea ReductionGaoudam NatarajanNo ratings yet
- The Effects of Cigarette SmokingDocument5 pagesThe Effects of Cigarette SmokingMarvin AnciaCupid100% (1)
- Cfu Med SurgDocument25 pagesCfu Med SurgCharlene Jacobe CornistaNo ratings yet
- 2023 CHP Ro EnglishDocument24 pages2023 CHP Ro EnglishWimukthi Sagara SilvaNo ratings yet
- July PNLE 2011 PreBoard ExamDocument9 pagesJuly PNLE 2011 PreBoard ExamRon KimNo ratings yet
- Theresa ncp-7Document3 pagesTheresa ncp-7Jovel CortezNo ratings yet
- Case Study On CopdDocument35 pagesCase Study On CopdPraty Sawaden100% (1)
- Ebooks File Developing The Digital Lung: From First Lung CT To Clinical AI 1st Edition John D. Newell All ChaptersDocument30 pagesEbooks File Developing The Digital Lung: From First Lung CT To Clinical AI 1st Edition John D. Newell All ChaptersavnaimirmaaNo ratings yet