Pain and Motor Control 2011 Hodges
Pain and Motor Control 2011 Hodges
Uploaded by
Pedro SilvaCopyright:
Available Formats
Pain and Motor Control 2011 Hodges
Pain and Motor Control 2011 Hodges
Uploaded by
Pedro SilvaCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Pain and Motor Control 2011 Hodges
Pain and Motor Control 2011 Hodges
Uploaded by
Pedro SilvaCopyright:
Available Formats
Journal of Electromyography and Kinesiology 21 (2011) 220228
Contents lists available at ScienceDirect
Journal of Electromyography and Kinesiology
journal homepage: www.elsevier.com/locate/jelekin
Review
Pain and motor control: From the laboratory to rehabilitation
Paul W. Hodges
The University of Queensland, Centre for Clinical Research Excellence in Spinal Pain, Injury and Health, School of Health and Rehabilitation Sciences, Brisbane, Qld 4072, Australia
a r t i c l e
i n f o
a b s t r a c t
Movement is changed in pain and is the target of clinical interventions. Yet the understanding of the physiological basis for movement adaptation in pain remains limited. Contemporary theories are relatively simplistic and fall short of providing an explanation for the variety of permutations of changes in movement control identied in clinical and experimental contexts. The link between current theories and rehabilitation is weak at best. New theories are required that both account for the breadth of changes in motor control in pain and provide direction for development and renement of clinical interventions. This paper describes an expanded theory of the motor adaptation to pain to address these two issues. The new theory, based on clinical and experimental data argues that: activity is redistributed within and between muscles rather than stereotypical inhibition or excitation of muscles; modies the mechanical behaviour in a variable manner with the objective to protect the tissues from further pain or injury, or threatened pain or injury; involves changes at multiple levels of the motor system that may be complementary, additive or competitive; and has short-term benet, but with potential long-term consequences due to factors such as increased load, decreased movement, and decreased variability. This expanded theory provides guidance for rehabilitation directed at alleviating a mechanical contribution to the recurrence and persistence of pain that must be balanced with other aspects of a multifaceted intervention that includes management of psychosocial aspects of the pain experience. 2011 Elsevier Ltd. All rights reserved.
Article history: Received 11 October 2010 Received in revised form 24 December 2010 Accepted 6 January 2011
Keywords: Motor control Pain Musculoskeletal pain Rehabilitation
Contents 1. 2. 3. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Current theoretical models for the motor adaptation to pain and their relationship to rehabilitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . New theory of the adaptation to pain. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.1. Redistribution of activity within and between muscles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.2. Altered mechanical behaviour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3. Protection from further pain or injury, or threatened pain or injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.4. Changes at multiple levels of the motor system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.5. Short-term benefit, but with potential long-term consequences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Implications of the new theory of motor adaptation in pain for rehabilitation of musculoskeletal pain. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Can motor adaptation be changed with intervention and does it make a difference? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221 221 222 222 223 223 223 223 224 225 226 226 226
4. 5. 6.
Tel.: +61 7 3365 2008; fax: +61 7 3365 1284.
E-mail addresses: p.hodges@uq.edu.au, p.hodges@shrs.uq.edu.au 1050-6411/$ - see front matter 2011 Elsevier Ltd. All rights reserved. doi:10.1016/j.jelekin.2011.01.002
P.W. Hodges / Journal of Electromyography and Kinesiology 21 (2011) 220228
221
1. Introduction Rehabilitation of control of movement and muscle activity is a mainstay of management of many pain conditions related to the musculoskeletal system. This is based on the premise that pain and movement are intimately linked. In the acute phase, the motor system provides an opportunity for the nervous system to respond and remove or reduce a threatening noxious stimulus (mechanical, chemical or thermal) to the tissues. If the nervous system concludes that a situation is threatening (this may be in response to discharge of nociceptive afferents or the threat of a noxious input) it can move or change the mechanical behaviour of the body to remove the threat, and reduce the potential for further pain/injury to the tissues. In the chronic phase the motor response may be less meaningful, less accurate or unnecessary as the threat to the tissues may be less relevant as a result of the range of physiological and psychological issues that change the gain of the pain system. Thus, the pain that a person experiences does not necessarily match the input from the nociceptive afferents and pain may not reect harm or potential harm to the tissues. Maintenance of a motor adaptation in chronic pain may not provide benet to the system. Many clinical interventions target changes in motor control that accompany pain. These include motor learning strategies (e.g. exercise with error correction, augmented feedback, part-practice), some psychological interventions (e.g. treatments to reduce threat value of pain), and hands-on techniques (e.g. manual therapy, muscle stretching, needling techniques). However, the mechanisms that underlie the motor adaptation to pain are surprisingly poorly understood and two primary theories have been proposed: vicious cycle (Roland, 1986) and pain adaptation (Lund et al., 1991). These theories explain some observations in clinical and experimental pain. However, there are two major limitations. First, many clinical and experimental observations are inconsistent with predictions made by these theories; and second, the link between these theories and rehabilitation is weak. The aim of this paper is to review the limitations of current theoretical models of the motor
adaptation to pain, to review a new theory (Hodges and Tucker, in press) that accounts for many of the observations that cannot be explained by existing theories, and to consider the implications for rehabilitation. 2. Current theoretical models for the motor adaptation to pain and their relationship to rehabilitation The vicious cycle theory proposes a stereotypical increase in activity of muscles that are painful or move the painful region. This muscle activity induces ischaemia from vascular compromise and becomes a source of further pain due to accumulation of pain metabolites (Roland, 1986). Various mechanisms have been proposed to explain the increase in muscle activity, including increased sensitivity of muscle spindles (Johansson and Sojka, 1991). Treatments based on this theory include the use of electromyography (EMG) biofeedback to train muscle relaxation, such as reduced activity of the erector spinae muscles in back pain (Flor et al., 1983) and the temporalis muscle in tension headache (Holroyd et al., 1984). Although this approach received some initial support (Flor et al., 1983; Nouwen, 1983) two issues compromise the validity of the approach. First, although there is evidence of increased muscle activity, this is not uniform and many studies show decreased (Wolf and Basmajian, 1977; Zedka et al., 1999) or no change (Kravitz et al., 1981; Cram and Steger, 1983) in activity. Second, clinical improvement has been reported despite no changes in muscle activity (Holroyd et al., 1984). This suggests clinical efcacy of may be related to cognitive aspects rather than rehabilitation of the motor adaptation. Alternative theories are required to explain the non-uniform changes in muscle activity and movement with pain and to guide interventions (see Fig. 1). The pain adaptation theory was developed to explain changes in voluntary movement and argues that activity of a muscle that is painful or produces a painful movement is uniformly inhibited, whereas that of the muscles that oppose the movement (antagonist) is facilitated (Lund et al., 1991). The outcome would
New theory for adaptation to pain R e h a b ilita tio n
Reduce pain to reduce impact on control and motor learning Pain/injury or threat of pain/injury Identify and train relevant aspects of redistributed activity high quality training
R e h a b ilita tio n
Multiple techniques likely to be required to Influence motor adaptation at different levels of the motor system including exercise, psychological treatments, and other modalities
Changes at multiple levels of the nervous system
Redistribution of activity within & between muscles
Changes the mechanical behaviour
Optimise load with balance between useful (compensation for injury) and unnecessary adaptation
Stiffness
Modified direction/load distribution
Enhance helpful components of adaptation
Short term benefit
Long term consequences
Reduce unnecessary components of adaptation
Protection of the injured/painful part
load movement variability
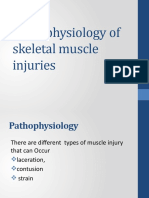
Fig. 1. New theory of motor adaptation to pain and implications for rehabilitation.
222
P.W. Hodges / Journal of Electromyography and Kinesiology 21 (2011) 220228
be decreased displacement, velocity or force to reduce pain provocation and further injury. These changes in excitability were proposed to be mediated by networks in the spinal cord or brainstem (Lund et al., 1991). Data in support of the theory can be identied largely from the effect of acute experimental pain. For instance, agonist muscle activity is reduced during voluntary movements of the jaw (Svensson et al., 1995), trunk (Zedka et al., 1999), neck (Falla et al., 2007) and limbs (Farina et al., 2005) and a combination of reduced and increased activity of opposing muscle groups has been shown in dynamic movements of the leg (Graven-Nielsen et al., 1997). However, the observations are not universally supported. First, recent work of motoneuron excitability by evaluation of the response to excitation of corticospinal axons at the level of the mastoid processes showed increased excitability of the motoneurons innervating both the painful muscle and its antagonist (Martin et al., 2008), rather than the predicted reduction of excitability of the agonist muscle. Second, activity of motoneurons in a painful muscle is not uniformly decreased (Tucker et al., 2009). Although discharge rate of some motoneurons is decreased (Farina et al., 2004a,b; Sohn et al., 2004), if the person is asked to generate a constant force between trials with and without pain, activity of other units increases to maintain the force output (Tucker and Hodges, 2009). Other data of motor behaviour (coordination of whole muscle activity) show that experimentally induced low back pain is accompanied by redistribution of activity between the multiple muscles of the trunk rather than a stereotypical and predictable change in muscle activation during slow voluntary trunk movements (Hodges et al., 2006). This is consistent with the high degree of variability observed in changes in trunk muscle control across many studies of clinical low back pain (van Dien et al., 2003). There are similar observations from other body systems such as the jaw (Murray and Peck, 2007). The link between the pain adaptation theory and rehabilitation is unclear. What would inhibition and excitation to reduce voluntary movement suggest for rehabilitation of pain? It may suggest that activity should be discouraged to relieve pain, but this is unlikely to be successful in restoring function. Consideration of the motor adaptation to pain in this paradigm has not led to clear implications for management and new models are required to drive improvements in rehabilitation.
protection from further pain or injury, or threatened pain or injury (as a result of a variety of changes such as decreased activity to reduce voluntary movement, increased activity to splint a body region, or change distribution of activity to modify the distribution of load on a structure); (iv) is not explained by simple changes in excitability, but involves changes at multiple levels of the motor system and these changes may be complementary, additive or competitive (rather than isolated effects of nociceptor afferent input at the spinal cord); and (v) has short-term benet, but with potential long-term consequences due to factors such as increased load, decreased movement, and decreased variability (Hodges and Tucker, in press) (Fig. 1). 3.1. Redistribution of activity within and between muscles The new theory proposes that rather that a uniform increase or decrease of activity there is an adaptation that may vary between individuals and tasks to change the mechanical response to protect the tissues or remove threat. A variety of options are available to meet the overall objective of protection. In some cases this may involve reduced activity (such as the inhibition of masseter muscles during painful jaw movement (Svensson et al., 1997) consistent with the pain adaptation theory), increased activity (such as increased activity of sternocleidomastoid in neck pain (Johnston et al., 2008) consistent with the vicious cycle theory) or a combination of both (such as increased and decreased abdominal muscle activity with slow trunk movements during experimental pain (Hodges et al., 2006). Studies of changes in responsiveness of corticomotor pathways indicate that muscles can be affected differentially. For instance, noxious stimuli to that hand increase responsiveness of hand muscles to magnetic stimuli over the motor cortex, but simultaneously decrease responsiveness of proximal arm muscles (Koer et al., 1998). Recent work shows similar differential affects on the distribution of activity between abdominal muscles with experimental back pain; responsiveness of pathways to transversus abdominis is reduced whereas those to obliquus abdominis externus are more responsive (Tsao et al., submitted for publication). The redistribution of activity may also occur within a muscle. Although reduced discharge rate of active motor units during experimental pain has been interpreted to suggest inhibition (Farina et al., 2004a,b; Sohn et al., 2004), recent work shows the force output is maintained by recruitment of additional units that were not active during contractions without pain (Tucker and Hodges, 2009). This cannot be explained by uniform inhibition of the motoneuron pool as new motor units are recruited despite reduced discharge of others. Although the adaptation of muscle activity may be predictable in some situations (e.g. voluntary jaw (Svensson et al., 1997) and limb movements (Graven-Nielsen et al., 1997)) this is not the case for complex systems such as the trunk. There is considerable redundancy amongst the trunk muscles (i.e. multiple muscles perform similar functions) and the objective of protection could be achieved via multiple strategies such as co-contraction of antagonist exor and extensor muscles, or increased activity of many combinations of these muscles (van Dien et al., 2003; Hodges et al., 2006). This is supported by modelling work (Van Dien et al., 2003). Although the large variation in adaptation in trunk muscle activity could be interpreted to suggest that no underlying theory can explain the adaptation, the alternative argument is that each individual develops a protective strategy that is unique based on experience, anthropometrics, posture, task, etc. The multiple possible solutions are likely to be related to the clinical subgroups of low back pain that have been proposed (Sahrman, 2002; OSullivan, 2005). If a goal of rehabilitation (e.g. using motor learning strategies) is to modify the adaptation (remove, modify or enhance,
3. New theory of the adaptation to pain A new theory has been developed on the basis of data from micro (motoneuron discharge) to macro (whole muscle behaviour) levels of the motor system in order to reconcile the complex nature of the adaptation in motor control that accompanies pain (Hodges and Tucker, in press). This theory is a progression from the vicious cycle and pain adaptation theories and is inclusive of the observations associated with the basis for those theories. The key progression of the theory is that it aims to account for variation in the adaptation in motor control rather than the stereotypical adjustments in behaviour predicted by existing theories and includes consideration of multiple concurrent possible mechanisms throughout the nervous system that can mediate such changes. The theory also has an objective to provide guidance for the development and renement of treatments. The following provides a summary of the main elements of the theory, the associated evidence, and implications for rehabilitation. The new theory proposes that pain is associated with an adaptation in motor behaviour that: (i) involves redistribution of activity within and between muscles (rather than inhibition or excitation of muscles in a stereotypical manner); (ii) changes the mechanical behaviour such as modied movement and stiffness; (iii) leads to
P.W. Hodges / Journal of Electromyography and Kinesiology 21 (2011) 220228
223
see below) then this needs to be considered on an individual basis with respect to the unique solution adopted by the patient. This would require development or renement of methods to assess the adaptation in motor control (e.g. with ultrasound imaging or electromyography). 3.2. Altered mechanical behaviour Removal or reduction of threat to the tissues can be achieved via multiple changes to the mechanics of a system. This could be removal of the body part from the threat (e.g. nociceptive withdrawal reex (Clarke and Harris, 2004), fright/ight response), reduced displacement/velocity/force (e.g. reduced displacement and velocity of voluntary jaw movement (Svensson et al., 1995)), stiffening a segment to prevent movement that is association with pain or the threat of pain or injury (e.g. trunk stiffening (Hodges et al., 2009b)), or modication of the distribution of load on a painful structure (e.g. changed angle of knee extension force (Tucker and Hodges, 2010)). Although some of these changes could be coordinated at a basic level of the nervous system (e.g. spinal cord control of the nociceptive withdrawal reex), other changes are more complex involving changes in higher processing and planning or even voluntary adjustment of force (e.g. search for a less painful movement option). It is likely that such adaptation would generally occur subconsciously and in the case of threat of pain it would not be necessary to have explicit conscious recognition of fear of pain/(re)injury. Although, the adaptation may be benecial in the short term, it may pose problems in the long-term and training an individual to reduce or modify the adaptation may form the basis of effective treatments (see below). 3.3. Protection from further pain or injury, or threatened pain or injury A basic assumption, like that proposed in the vicious cycle and pain adaptation theories, is that the adaptation aims to protect the body segment from pain or injury, or the threat of pain or injury. Although the vast majority of experimental and clinical observations can be reconciled on this basis (e.g. nociceptive withdrawal reex, reduced agonist activity during voluntary movement), recent work provides additional support. When stepping down from a stair, activity of gluteal muscles precedes foot contact to control hip loading (Zazulak et al., 2005) and this activity is earlier and greater to enhance the protection for the hip when the stair height increases (e.g. 5 cm vs. 15 cm step height) (Hodges et al., 2009a). Consistent with the hypothesised protective nature of the adaptation of motor control with pain, when the contact of the foot with the oor is associated with pain or anticipated pain (e.g. painful electrical shock to the back triggered by foot contact) the strategy normally reserved for the 15 cm stair height is used for the 5 cm stair (Hodges et al., 2009a) (i.e. a solution reserved for a high load task is used for a lower load task). Many permutations of adapted motor behaviour may lead to enhanced protection such as decreased muscle activity and force (Svensson et al., 1995); muscle splinting (Kaigle et al., 1998); withdrawal (Clarke and Harris, 2004) as described in the previous section. 3.4. Changes at multiple levels of the motor system Initial theories assumed relatively simple mechanisms to explain the adaptation to pain, such as direct input from nociceptive afferents on motoneurons (Kniffki et al., 1979), inhibitory and facilitatory interneurons and circuits in the spinal cord and brain stem (Lund et al., 1991), and increased spindle sensitivity (Matre et al., 1998; Wang et al., 2000; Svensson et al., 2001; Thunberg et al.,
2002). Work over the past few decades has highlighted multiple mechanisms. In addition to well-established spinal mechanisms, changes have been identied in excitability (Le Pera et al., 2001; Strutton et al., 2003; Martin et al., 2008; Tsao et al., 2008) and organisation (Maihfner et al., 2007; Tsao et al., 2008) of the motor cortex, and more complex changes in the planning of motor responses that may be mediated upstream of the motor cortex (Hodges and Moseley, 2003). This latter class of changes include changes in the pattern of activity of muscles of the trunk initiated prior to predictable perturbations to the body, such as anticipatory postural adjustments (Hodges and Richardson, 1996). Changes in sensory function will have profound effects on control of movement and have been identied in many painful conditions of the musculoskeletal system (e.g. ankle sprain (Garn and Newton, 1988), shoulder pain (Warner et al., 1996), back pain (Newcomer et al., 2000), neck pain (Treleaven et al., 2006), knee osteoarthritis (Sharma and Pai, 1997)). Changes include reduced sensory acuity (Sharma and Pai, 1997), increased errors in repositioning (Brumagne et al., 1999), reduced responsiveness to sensory input (Brumagne et al., 2004), and reorganisation of the somatosensory regions of the brain cortex (Flor et al., 1997). The multiple mechanisms that may inuence movement could be complementary, additive, or competitive. For instance, competing effects have been identied following injury to a porcine intervertebral disc with reduced responsiveness of spinal pathways, but increased responsiveness to stimulation over the motor cortex (Hodges et al., 2009c). In contrast, activation of groups III and IV muscle afferents (nociceptive afferents) by hypertonic saline injection into human biceps brachii facilitates motoneurons innervating elbow exor and extensor muscles but depresses excitability of motor cortical cells projecting to these muscles (Martin et al., 2008). The net effect may be to limit voluntary activation but enhance responsiveness to other inputs. Other work cites complementary inhibition at both the cortex and motoneurons, but with a different time-course (Le Pera et al., 2001). The critical message for clinical practice is that the motor output observed in patients may have multiple underlying mechanisms and each may have unique implications for rehabilitation. 3.5. Short-term benet, but with potential long-term consequences Although adaptation in motor behaviour may be benecial in the short-term, failure of the adaptation to resolve after the initial period following injury (at which time a protective response may be appropriate for survival) may pose risks for the tissues and nervous system. The vicious cycle theory also proposes a consequence of the adaptation to pain, yet this was simply explained by chemical irritation of nociceptive afferents due to ischaemia from sustained contraction (Roland, 1986). In addition to this possibility, the new theory proposes consequences from modied loading of the tissues as a result of altered mechanical behaviour. This has important implications for rehabilitation as techniques to resolve the adaptation may help to reduce persistence or recurrence of pain. There are a number of reasons why the changes in mechanical behaviour may not be ideal if maintained. First, the protective solution may compromise the quality of movement. For instance, increased trunk stiffness in low back pain is associated with decreased damping (i.e. control of velocity) (Hodges et al., 2009b), which is likely to be important to minimise the effect of perturbations. Although people normally move the spine in advance of predictable challenges to the spine, this is less frequently used in people with pain (Mok et al., 2007), and is accompanied by greater perturbation to the spine (Mok et al., 2007) and decreased quality of the postural recovery after the perturbation (Mok et al., 2009). In the lower limb, decreased knee exion (i.e. increased knee
224
P.W. Hodges / Journal of Electromyography and Kinesiology 21 (2011) 220228
stiffness) is present in non-copers following ACL tear (Rudolph et al., 1998) and may underlie ongoing problems. Second, the adaptation may increase load on the tissues (e.g. if muscle activity is increased) or change the distribution of load (e.g. change distribution of activity within or between synergist muscles), which may lead to tissue irritation, particularly if there is sensitisation. For instance people with back pain have greater load on the spine during lifting than pain-free individuals as a direct result of changes in muscle activation (Marras et al., 2004) and this may lead to structural change over time (Kumar, 1990). Although changes in the distribution of load may theoretically benet the system by unloading a painful structure with short-term benet to decrease pain and injury, the adaptation would inevitably increase load on other structures. Many other examples have been presented in the literature. For instance, movement adaptations follow ankle sprain such as reduced ankle dorsiexion (Friel et al., 2006) to reduce loading of the injured ankle structures leads to modied kinematics at proximal joints (Davis and Seol, 2005). If maintained in the long-term these changes may lead to problems elsewhere in the body (Davis and Seol, 2005). Third, adaptations in motor behaviour such as increased muscle activity to splint the painful pain may reduce movement variability. Although too much variation is not ideal (Tzagarakis et al., 2010), so too is too little variation (Hamill et al., 1999). If movement is performed in the same manner with each repetition this will load the same structures, same joint surface, same muscles each time. With some variation the load is shared resulting in potential benets for tissue health. Reduced variation has been identied in a range of conditions, such as lower limb pathologies and variability in gait (Hamill et al., 1999). An underlying premise of the new theory of motor adaptation to pain is that the adaptation is less relevant or even detrimental in the long-term. This is aligned to current pain theory that proposes that when pain persists beyond the period of tissue healing the mechanics at the tissue level may be less important and the central mechanisms for maintenance of pain may be more important. Both physiological and psychosocial factors underlie a mismatch between the nociceptive discharge in the periphery and the pain experienced by the individual (Waddell, 1998; Latremoliere and Woolf, 2009). These changes include: plastic changes in the responsiveness and function of neurons and circuits in the spinal cord that change the gain of the pain system (Cook et al., 1987); modication of function of the descending facilitatory and inhibitory pain systems (Arendt-Nielsen et al., 2010); cognitive aspects of pain such as catastrophising and fear of pain that modify threat value (Sullivan et al., 2001). In each of these cases there may be a mismatch between the relevance of nociceptive afferent discharge and the experience of pain, and at the tissue level the adaptation in movement control may no longer be relevant or appropriate. The alternative argument is that some degree of tissue-level change may have a maintained contribution to the perpetuation of pain. Panjabi (1992) proposed that adaptation in muscle and neural control is required to compensate for any loss of passive support from joint structures as a result of tissue injury. In this case some degree of adaptation may be benecial (van Dien et al., 2003). Although this may be true in some cases, the possibility to replicate changes in motor control (e.g. increased protection) simply by the threat of pain, in the absence of injury (Moseley et al., 2004), implies the relationship between injury and adaptation is not linear; i.e. input is not directly related to output. In some cases the adaptation may be appropriate leading to reduced pain in the long-term, and this could explain the mismatch between structural joint changes and pain where some people experience little pain despite signicant joint damage. The lack of pain in this context may be due to a combination of an appropriate adaptation of the motor system to compensate for
the structural damage (i.e. appropriate protective strategy) and the fact that pain is an output of the central nervous system based on interpretation of inputs, and not directly explained by the input from nociceptor discharge. If the nervous system has taken action to protect the injured/painful part (i.e. adapted the motor behaviour), then the pain output may be reduced. Taken together it would seem reasonable to conclude that it is necessary nd the right balance between restoration of control to some baseline and the maintenance or retention of elements of the adaptation in order to meet the demands of function. Although the proposal that failure of resolution of the adaptation to pain may contribute to recurrence or persistence of pain is based on sound reasoning, there is lack of data from high quality longitudinal studies to support this hypothesis. Some data support the association between non-resolution of acute atrophy of the multidus muscle and future recurrence of back pain (Hides et al., 2001). However, that study was small and the group with muscle recovery also received a different treatment package than the control group and this may have independently affected the outcome. Investigation of the relationship between adaptation and long-term outcome will not be simple as there is potential for enormous variation in adaptation and the interaction between biological, psychological and social aspects when pain persists is complex. A nal consideration is that adaptation leading to long-term changes may be caused by factors other than an initial injury or pain related to a musculoskeletal structure. For instance, motor control may adapt in response to more widespread or centrally mediated pain states or other issues that challenge the motor system (e.g. respiratory (Hodges et al., 2001) and continence (Smith et al., 2007) challenges affect trunk muscle control in a similar manner to spinal pain). Like the adaptation to an acute pain/injury these changes may lead to further problems (Smith et al., 2009).
4. Implications of the new theory of motor adaptation in pain for rehabilitation of musculoskeletal pain How can the new theory inform rehabilitation for people with musculoskeletal pain? Although existing models of the adaptation to pain provide limited guidance for rehabilitation, the expanded theory of motor adaptation to pain provides a rich array of implications that can be used to shape interventions. Such interventions may include exercise (e.g. training of motor control or movement strategy), psychological interventions (e.g. treatments that change the threat value of pain), and physical modalities (e.g. modalities that can inuence muscle activation such as manual therapy techniques). It is important to acknowledge that it is not possible to predict the size of a clinical effect on the basis of physiological data, and clinical trials are needed to determine whether changes to clinical practice lead to better outcomes. However, hypotheses can be proposed for testing in appropriate clinical trials. A key aspect of the new expanded theory for motor adaptation to pain with implications for rehabilitation is the proposal that the adaptation may have short-term benet but with long-term consequences. It is proposed that if the motor adaptation is excessive or fails to resolve after it is no longer helpful it may contribute to the perpetuation or recurrence of injury and pain. The clinical conclusion is that clinicians need to identify aspects that may be excessive/inappropriate and develop a strategy to train the patient to restore more optimal control. The alternative and not mutually exclusive view is that the adaptation may be necessary to compensate for decit in the passive support for the segment (e.g. injury to intervertebral disc) and that enhanced control is required to meet the demands for control of the segment (Panjabi, 1992; van Dien et al., 2003). In rehabilitation the challenge will be to identify the
P.W. Hodges / Journal of Electromyography and Kinesiology 21 (2011) 220228
225
relevance of the adaptation and nd the balance between that which is required and that which is not. According to the theory, resolution of the motor adaptation would involve redistribution of activity between and within muscles to modify the mechanical behaviour of the body segment. Redistribution of activity between muscles is already considered as part of existing interventions. For instance rehabilitation of the coordination between the medial and lateral vasti muscles is effective for the management of anterior knee pain (patellofemoral pain syndrome) (Crossley et al., 2002) and treatment of back pain that includes modication of the coordination between trunk muscles reduces pain and disability and prevents recurrence of episodes (OSullivan et al., 1997; Hides et al., 2001; Stuge et al., 2004; Ferreira et al., 2006; Macedo et al., 2009). Clinical tools are used to aid redistribution of activity between muscles such as techniques to provide feedback (e.g. electromyography (McConnell, 1986; Crossley et al., 2002) and ultrasound imaging (Hides et al., 1996)) and techniques that enhance the function of specic muscles (e.g. application of therapeutic tape (Cowan et al., 2002b)). Redistribution of activity within the upper trapezius has been applied in shoulder pain (Samani et al., 2010). A similar approach may have potential in other conditions. As changes may occur at multiple levels of the nervous system, a range of clinical strategies are likely to be required to restore/retrain ideal control. If the motor adaptation was simply due to input from nociceptive afferents on motoneurons (Kniffki et al., 1979) or due to reex inhibition (Spencer et al., 1984) it could be assumed that the most appropriate treatment should be application of techniques to reduce pain (e.g. analgesic agents) or techniques that may increase motoneuron excitability (e.g. peripheral electrical stimulation). Treatment of pain is unlikely to be sufcient to restore motor control as it has been shown that many aspects of the motor adaptation persist between episodes, despite resolution of pain (Hodges and Richardson, 1996; MacDonald et al., 2009), that is, motor control adaptation does not require ongoing nociceptor stimulation for maintenance. Interventions that target higher levels of the motor system are likely to be required. These include motor learning strategies to change planning and coordination of movement and muscle activity (such as biofeedback techniques to change distribution of activity described above), and management of unhelpful cognitions such as catastrophising and fearavoidance, which may inuence the muscle activation strategies. The greatest challenge will be to validate clinical techniques to determine which aspects of the motor adaptation are necessary to change. 5. Can motor adaptation be changed with intervention and does it make a difference? A variety of clinical interventions have been proposed to retrain motor control in musculoskeletal pain. These interventions vary in their approach and are based on a multitude of clinical theories such as aiming to modify loads on painful structures (Crossley et al., 2000) and enhance protection of a painful part (McGill, 2002; van Dien et al., 2003). The common feature is the use of relearning strategies to change motor features considered to contribute to the perpetuation or recurrence of pain. There are varying levels of experimental support for these approaches, but evidence as accruing that motor adaptation to pain can be resolved with rehabilitation and this is associated with positive clinical effects. One example is work in low back pain that has investigated temporal and spatial aspects of activation of the deep abdominal muscle, transversus abdominis, in trials of motor rehabilitation. The implication is not that this change constitutes the entirety of the adaptation, but that it is a common component that can be used as a marker of adaptation. Delayed and reduced
activation of transversus abdominis is common in low back pain, it persists between pain episodes (Hodges and Richardson, 1996; Ferreira et al., 2004), and can be induced by experimental pain (Hodges et al., 2003). Delayed and reduced activation of transversus abdominis can be restored with motor relearning strategies (Tsao and Hodges, 2007). These changes persist after cessation of training (Tsao and Hodges, 2008), are related to the magnitude of improvement in pain/disability (Ferreira et al., 2010), and baseline values can indicate individuals who will respond to the intervention (Ferreira et al., 2010). These interventions also change the organisation of the motor cortical networks (assessed with transcranial magnetic stimulation of the motor cortex) that have input to this muscle (Tsao et al., 2010b) and the amplitude of change in timing is related to the magnitude of cortical reorganisation (Tsao et al., 2010b). Current data do not clarify whether symptom improvement is due to improved activation of transversus abdominis or the resolution of other aspects of the adaptation, such as more optimal control of other trunk muscles or movement and/posture. Regardless, the activation of transversus abdominis serves as a useful marker of the motor recovery. Other work indicates that activation of another deep trunk muscle, multidus, can be improved with motor control training and net activity of other more supercial trunk muscles reduced (Tsao et al., 2010a). Application of a similar program to the restoration of coordination of vasti muscles of the knee successfully changes relative timing of muscles (Cowan et al., 2002a; Cowan et al., 2003) and this is linked to clinical improvement. An important observation in this work is that improvements in motor control appear dependent on conscious and precise correction of movement and muscle activity. Simple activation of the muscles without feedback or error correction, such as the activation of transversus abdominis during a sit-up, does not lead to changes in temporal or spatial features of muscle activation (Tsao and Hodges, 2007). This is consistent with the observation that cortical plasticity is dependent on the extent of conscious attention and skill during motor training (Karni et al., 1995; Plautz et al., 2000; Remple et al., 2001), and that movement repetition in the absence of skill or precision does not induce reorganisation (Plautz et al., 2000; Remple et al., 2001). Although other clinical techniques may also change coordination (e.g. application of tape over the skin modies symptoms and muscle activation (Crossley et al., 2000; Cowan et al., 2002b; Macgregor et al., 2005); joint manipulation/mobilisation changes transversus abdominis activation is some (Marshall and Murphy, 2006), but not all trials (Ferreira et al., 2007)), current data indicate motor control training with conscious attention to correction of motor control is effective. Does pain interfere with motor learning? It has been suggested that pain may interfere with plastic change in the motor cortex (Boudreau et al., 2007). That study showed when a tongue protrusion task was performed in the presence of pain, the expected training-induced increase in responsiveness of the corticomotor pathway was reduced. This was argued to be due to changes in cortical excitability in presence of pain (Le Pera et al., 2001). Although it is possible that pain may affect learning processes and animal studies indicate compromised capacity for learning due to pain-induced changes at the spinal cord (Hook et al., 2008), inspection of data from the study of Boudreau et al. (2007) suggest that failure of adaptation could be secondary to modied performance of the training task during pain. If quality of movement is maintained, the training-induced changes are unaffected by pain (Tucker et al., 2010). Thus pain may compromise learning by its affect on the performance of the task that is practiced rather than a direct effect of pain on plastic processes that are required for learning in the motor system. This highlights that quality of training is likely to be a key determinant of treatment success, and the poten-
226
P.W. Hodges / Journal of Electromyography and Kinesiology 21 (2011) 220228 Farina D, Arendt-Nielsen L, Graven-Nielsen T. Experimental muscle pain decreases voluntary EMG activity but does not affect the muscle potential evoked by transcutaneous electrical stimulation. Clin Neurophysiol 2005;116(7): 155865. Farina D, Arendt-Nielsen L, Merletti R, Graven-Nielsen T. Effect of experimental muscle pain on motor unit ring rate and conduction velocity. J Neurophysiol 2004b;91(3):12509. Ferreira ML, Ferreira PH, Hodges PW. Changes in postural activity of the trunk muscles following spinal manipulative therapy. Manual Therapy 2007;12(3): 2408. Ferreira P, Ferreira M, Hodges P. Changes recruitment of the abdominal muscles in people with low back pain: ultrasound measurement of muscle activity. Spine 2004;29:25606. Ferreira P, Ferreira M, Maher C, Refshauge K, Herbert R, Hodges P. Changes in recruitment of transversus abdominis correlate with disability in people with chronic low back pain. Br J Sports Med 2010;44(16):116672. Ferreira PH, Ferreira ML, Maher CG, Herbert RD, Refshauge K. Specic stabilisation exercise for spinal and pelvic pain: a systematic review. Aust J Physiother 2006;52(2):7988. Flor H, Braun C, Elbert T, Birbaumer N. Extensive reorganization of primary somatosensory cortex in chronic back pain patients. Neurosci Lett 1997;224(1): 58. Flor H, Haag G, Turk DC, Koehler H. Efcacy of EMG biofeedback, pseudotherapy, and conventional medical treatment for chronic rheumatic back pain. Pain 1983;17(1):2131. Friel K, McLean N, Myers C, Caceres M. Ipsilateral hip abductor weakness after inversion ankle sprain. J Athletic Train 2006;41(1):748. Garn SN, Newton RA. Kinesthetic awareness in subjects with multiple ankle sprains. Phys Ther 1988;68(11):166771. Graven-Nielsen T, Svensson P, Arendt-Nielsen L. Effects of experimental muscle pain on muscle activity and co-ordination during static and dynamic motor function. Electroencephalography Clin Neurophysiol 1997;105(2):15664. Hamill J, van Emmerik RE, Heiderscheit BC, Li L. A dynamical systems approach to lower extremity running injuries. Clin Biomech 1999;14(5):297308. Hides JA, Jull GA, Richardson CA. Long term effects of specic stabilizing exercises for rst episode low back pain. Spine 2001;26:2438. Hides JA, Richardson CA, Jull GA. Multidus muscle recovery is not automatic after resolution of acute, rst-episode low back pain. Spine 1996;21(23):27639. Hodges P, Cholewicki J, Coppieters M, MacDonald D. Trunk muscle activity is increased during experimental back pain, but the pattern varies between individuals. In: Proceedings international society for electrophysiology and kinesiology, 2006. Hodges P, Simms K, Tsao H. Gain of postural responses is increased in anticipation of pain. In: Proceedings Australian physiotherapy association national congress week, 2009a. Hodges P, Tucker K. Moving differently in pain: a new theory to explain the adaptation to pain. Pain, in press. doi:10.1016/j.pain.2010.10.020. Hodges P, van den Hoorn W, Dawson A, Cholewicki J. Changes in the mechanical properties of the trunk in low back pain may be associated with recurrence. J Biomech 2009b;42(1):616. Hodges PW, Galea MP, Holm S, Holm AK. Corticomotor excitability of back muscles is affected by intervertebral disc lesion in pigs. Eur J Neurosci 2009c;29(7): 1490500. Hodges PW, Moseley GL. Pain and motor control of the lumbopelvic region: effect and possible mechanisms. J Electromyogr Kinesiol 2003;13(4):36170. Hodges PW, Moseley GL, Gabrielsson A, Gandevia SC. Experimental muscle pain changes feedforward postural responses of the trunk muscles. Exp Brain Res 2003;151(2):26271. Hodges PW, Heijnen I, Gandevia SC. Reduced postural activity of the diaphragm in humans when respiratory demand is increased. J Physiol 2001;537:9991008. Hodges PW, Richardson CA. Inefcient muscular stabilisation of the lumbar spine associated with low back pain: a motor control evaluation of transversus abdominis. Spine 1996;21:264050. Holroyd KA, Penzien DB, Hursey KG, Tobin DL, Rogers L, Holm JE, et al. Change mechanisms in EMG biofeedback training: cognitive changes underlying improvements in tension headache. J Consult Clin Psychol 1984;52(6):103953. Hook MA, Huie JR, Grau JW. Peripheral inammation undermines the plasticity of the isolated spinal cord. Behav Neurosci 2008;122(1):23349. Johansson H, Sojka P. Pathophysiological mechanisms involved in genesis and spread of muscular tension in occupational muscle pain and in chronic musculoskeletal pain syndromes: a hypothesis. Med Hypotheses 1991;35(3):196203. Johnston V, Jull G, Souvlis T, Jimmieson NL. Neck movement and muscle activity characteristics in female ofce workers with neck pain. Spine 2008;33(5): 55563. Kaigle AM, Wessberg P, Hansson TH. Muscular and kinematic behavior of the lumbar spine during exionextension. J Spinal Disord 1998;11(2):16374. Karni A, Meyer G, Jezzard P, Adams MM, Turner R, Ungerleider LG. Functional MRI evidence for adult motor cortex plasticity during motor skill learning. Nature 1995;377(6545):1558. Kniffki KD, Schomburg ED, Steffens H. Synaptic responses of lumbar alphamotoneurones to chemical algesic stimulation of skeletal muscle in spinal cats. Brain Res 1979;160(3):54952. Koer M, Glocker FX, Leis AA, Seifert C, Wissel J, Kronenberg MF, et al. Modulation of upper extremity motoneurone excitability following noxious nger tip stimulation in man: a study with transcranial magnetic stimulation. Neurosci Lett 1998;246(2):97100.
tial benet of combining training with other modalities to relieve pain. Other work also highlights the ability of an intervention to change motor function depends on the quality of training; higher quality training induces larger changes in temporal aspects of muscle activation (Tsao and Hodges, 2007). Taken together these ndings indicate that motor plasticity may be enhanced by training without pain provocation and training with high quality feedback. Although some methods are available to assess motor adaptation and provide feedback (e.g. electromyography (Cowan et al., 2002a), ultrasound imaging (Richardson et al., 1999; Teyhen et al., 2007; Stokes et al., 2007) to change the redistribution of activity within and between muscles further technological development is likely to be required to optimise this approach across a range of conditions.
6. Conclusion The new theory of motor adaptation to pain provides a more comprehensive explanation of clinical and experimental observations. The theory also provides a range of principles that can be applied and trialed for the rehabilitation of musculoskeletal pain. Some of these implications are supported by data from clinical trials whereas others provide predictions that require testing to conrm the magnitude of potential clinical effects. Acknowledgement PH is supported by a Fellowship from the National Health and Medical Research Council of Australia. References
Arendt-Nielsen L, Nie H, Laursen MB, Laursen BS, Madeleine P, Simonsen OH, et al. Sensitization in patients with painful knee osteoarthritis. Pain 2010;149(3): 57381. Boudreau S, Romaniello A, Wang K, Svensson P, Sessle BJ, Arendt-Nielsen L. The effects of intra-oral pain on motor cortex neuroplasticity associated with shortterm novel tongue-protrusion training in humans. Pain 2007;132(12): 16978. Brumagne S, Cordo P, Verschueren S. Proprioceptive weighting changes in persons with low back pain and elderly persons during upright standing. Neurosci Lett 2004;366(1):636. Brumagne S, Lysens R, Spaepen A. Lumbosacral position sense during pelvic tilting in men and women without low back pain: test development and reliability assessment. J Orthop Sports Phys Ther 1999;29(6):34551. Clarke RW, Harris J. The organization of motor responses to noxious stimuli. Brain Res Brain Res Rev 2004;46(2):16372. Cook AJ, Woolf CJ, Wall PD, McMahon SB. Dynamic receptive eld plasticity in rat spinal cord dorsal horn following c-primary afferent input. Nature 1987;325(7000):1513. Cowan SM, Bennell KL, Crossley KM, Hodges PW, McConnell J. Physical therapy alters recruitment of the vasti in patellofemoral pain syndrome. Med Sci Sports Exer 2002a;34(12):187985. Cowan SM, Bennell KL, Hodges PW. Therapeutic patellar taping changes the timing of vasti muscle activation in people with patellofemoral pain syndrome. Clin J Sports Med 2002b;12(6):33947. Cowan SM, Bennell KL, Hodges PW, Crossley KM, McConnell J. Simultaneous feedforward recruitment of the vasti in untrained postural tasks can be restored by physical therapy. J Orthop Res 2003;21(3):5538. Cram JR, Steger JC. EMG scanning in the diagnosis of chronic pain. Biofeedback Self Regulat 1983;8:22941. Crossley K, Bennell K, Green S, Cowan S, McConnell J. Physical therapy for patellofemoral pain: a randomized, double-blinded, placebo-controlled trial. Am J Sports Med 2002;30(6):85765. Crossley K, Cowan SM, Bennell KL, McConnell J. Patellar taping: is clinical success supported by scientic evidence? Manual Therapy 2000;5(3):14250. Davis KG, Seol H. Injury-induced kinematic compensations within the lower back: impact of non-lower back injuries. Ergonomics 2005;48(2):13549. Falla D, Farina D, Dahl MK, Graven-Nielsen T. Muscle pain induces task-dependent changes in cervical agonist/antagonist activity. J Appl Physiol 2007;102(2):6019. Farina D, Arendt-Nielsen L, Graven-Nielsen T. Spike-triggered average torque and muscle ber conduction velocity of low-threshold motor units following submaximal endurance contractions. J Appl Physiol 2004.
P.W. Hodges / Journal of Electromyography and Kinesiology 21 (2011) 220228 Kravitz E, Moore ME, Glaros AG. Paralumbar muscle activity in chronic low back pain. Arch Phys Med Rehab 1981;62:1726. Kumar S. Cumulative load as a risk factor for back pain. Spine 1990;15(12):13116. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural plasticity. J Pain 2009;10(9):895926. Le Pera D, Graven-Nielsen T, Valeriani M, Oliviero A, Di Lazzaro V, Tonali PA, et al. Inhibition of motor system excitability at cortical and spinal level by tonic muscle pain. Clin Neurophysiol 2001;112(9):163341. Lund JP, Donga R, Widmer CG, Stohler CS. The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity. Can J Physiol Pharmacol 1991;69(5):68394. MacDonald D, Moseley GL, Hodges PW. Why do some patients keep hurting their back? Evidence of ongoing back muscle dysfunction during remission from recurrent back pain. Pain 2009;142(3):1838. Macedo LG, Maher CG, Latimer J, McAuley JH. Motor control exercise for persistent, nonspecic low back pain: a systematic review. Phys Ther 2009;89(1):925. Macgregor K, Gerlach S, Mellor R, Hodges PW. Cutaneous stimulation from patella tape causes a differential increase in vasti muscle activity in people with patellofemoral pain. J Orthop Res 2005;23(2):3518. Maihfner C, Baron R, DeCol R, Binder A, Birklein F, Deuschl G, et al. The motor system shows adaptive changes in complex regional pain syndrome. Brain 2007;130(Pt. 10):267187. Marras WS, Ferguson SA, Burr D, Davis KG, Gupta P. Spine loading in patients with low back pain during asymmetric lifting exertions. Spine J 2004;4:6475. Marshall P, Murphy B. The effect of sacroiliac joint manipulation on feed-forward activation times of the deep abdominal musculature. J Manipulat Physiol Therap 2006;29(3):196202. Martin PG, Weerakkody N, Gandevia SC, Taylor JL. Group iii and iv muscle afferents differentially affect the motor cortex and motoneurones in humans. J Physiol 2008;586(5):127789. Matre DA, Sinkjaer T, Svensson P, Arendt-Nielsen L. Experimental muscle pain increases the human stretch reex. Pain 1998;75(23):3319. McConnell J. The management of chondromalacia patellae: a long term solution. Aust J Physiother 1986;23(4):21523. McGill S. Low back disorders: evidence based prevention and rehabilitation. Champaign, IL: Human Kinetics Publishers, Inc.; 2002. Mok N, Brauer S, Hodges P. Delayed initiation of trunk movement and prolonged balance recovery in response to unexpected loading in people with chronic low back pain. In: Proceedings international society for the study of the lumbar spine, 2009. Mok NW, Brauer SG, Hodges PW. Failure to use movement in postural strategies leads to increased spinal displacement in low back pain. Spine 2007;32(19):E53743. Moseley GL, Nicholas MK, Hodges PW. Does anticipation of back pain predispose to back trouble? Brain 2004;127(Pt 10):233947. Murray GM, Peck CC. Orofacial pain and jaw muscle activity: a new model. J Orofac Pain 2007;21(4):26378. Newcomer KL, Laskowski ER, Yu B, Johnson JC, An KN. Differences in repositioning error among patients with low back pain compared with control subjects. Spine 2000;25(19):248893. Nouwen A. Emg biofeedback used to reduce standing levels of parspinal muscle tension in chronic low back pain. Pain 1983;17:35360. OSullivan P. Diagnosis and classication of chronic low back pain disorders: maladaptive movement and motor control impairments as underlying mechanism. Manual Ther 2005;10(4):24255. OSullivan PB, Twomey LT, Allison GT. Evaluation of specic stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine 1997;22(24):295967. Panjabi MM. The stabilizing system of the spine. Part i. Function, dysfunction, adaptation, and enhancement. J Spinal Disord 1992;5(4):3839. Plautz EJ, Milliken GW, Nudo RJ. Effects of repetitive motor training on movement representations in adult squirrel monkeys: role of use versus learning. Neurobiol Learn Memory 2000;74(1):2755. Remple MS, Bruneau RM, VandenBerg PM, Goertzen C, Kleim JA. Sensitivity of cortical movement representations to motor experience. Evidence that skill learning but not strength training induces cortical reorganization. Behav Brain Res 2001;123(2):13341. Richardson CA, Jull GA, Hodges PW, Hides JA. Therapeutic exercise for spinal segmental stabilisation in low back pain: Scientic basis and clinical approach. Edinburgh: Churchill Livingstone; 1999. Roland M. A critical review of the evidence for a pain-spasm-pain cycle in spinal disorders. Clin Biomech 1986;1:1029. Rudolph KS, Eastlack ME, Axe MJ, Snyder-Mackler L. Basmajian student award paper: movement patterns after anterior cruciate ligament injury: a comparison of patients who compensate well for the injury and those who require operative stabilization. J Electromyogr Kinesiol 1998;8(6):34962. Sahrman S. Diagnosis and treatment of movement impairment syndromes. St. Louis: Mosby, Inc.; 2002. Samani A, Holtermann A, Sgaard K, Madeleine P. Active biofeedback changes the spatial distribution of upper trapezius muscle activity during computer work. Eur J Appl Physiol 2010;110(2):41523. Sharma L, Pai YC. Impaired proprioception and osteoarthritis. Curr Opin Rheumatol 1997;9(3):2538. Smith MD, Russell A, Hodges PW. Do incontinence, breathing difculties, and gastrointestinal symptoms increase the risk of future back pain? J Pain 2009;10:87686.
227
Smith MD, Coppieters MW, Hodges PW. Postural response of the pelvic oor and abdominal muscles in women with and without incontinence. Neurourol Urodyn 2007;26:37785. Sohn MK, Graven-Nielsen T, Arendt-Nielsen L, Svensson P. Effects of experimental muscle pain on mechanical properties of single motor units in human masseter. Clin Neurophysiol 2004;115(1):7684. Spencer JD, Hayes KC, Alexander IJ. Knee joint effusion and quadriceps reex inhibition in man. Arch Phys Med Rehab 1984;65:1717. Stokes M, Hides J, Elliott J, Kiesel K, Hodges P. Rehabilitative ultrasound imaging of the posterior paraspinal muscles. J Orthop Sports Phys Ther 2007;37:58195. Strutton PH, Catley M, McGregor AH, Davey NJ. Corticospinal excitability in patients with unilateral sciatica. Neurosci Lett 2003;353(1):336. Stuge B, Veierod MB, Laerum E, Vollestad N. The efcacy of a treatment program focusing on specic stabilizing exercises for pelvic girdle pain after pregnancy: a two-year follow-up of a randomized clinical trial. Spine 2004;29(10): E197203. Sullivan MJ, Thorn B, Haythornthwaite JA, Keefe F, Martin M, Bradley LA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 2001;17(1):5264. Svensson P, Arendt-Nielsen L, Houe L. Sensorymotor interactions of human experimental unilateral jaw muscle pain: a quantitative analysis. Pain 1995;64:2419. Svensson P, Houe L, Arendt-Nielsen L. Bilateral experimental muscle pain changes electromyographic activity of human jaw-closing muscles during mastication. Exp Brain Res 1997;116(1):1825. Svensson P, Macaluso GM, De Laat A, Wang K. Effects of local and remote muscle pain on human jaw reexes evoked by fast stretches at different clenching levels. Exp Brain Res 2001;139(4):495502. Teyhen DS, Gill NW, Whittaker JL, Henry SM, Hides JA, Hodges P. Rehabilitative ultrasound imaging of the abdominal muscles. J Orthop Sports Phys Ther 2007;37:45066. Thunberg J, Ljubisavljevic M, Djupsjobacka M, Johansson H. Effects on the fusimotor-muscle spindle system induced by intramuscular injections of hypertonic saline. Exp Brain Res 2002;142(3):31926. Treleaven J, Jull G, Low Choy N. The relationship of cervical joint position error to balance and eye movement disturbances in persistent whiplash. Manual Therapy 2006;11(2):99106. Tsao H, Druitt TR, Schollum TM, Hodges PW. Motor training of the lumbar paraspinal muscles induces immediate changes in motor coordination in patients with recurrent low back pain. J Pain 2010a;11(11):11208. Tsao H, Galea MP, Hodges PW. Reorganization of the motor cortex is associated with postural control decits in recurrent low back pain. Brain 2008;131(Pt. 8):216171. Tsao H, Galea MP, Hodges PW. Driving plasticity in the motor cortex in recurrent low back pain. Eur J Pain 2010b;14(8):8329. Tsao H, Hodges P. Persistence of improvements in postural strategies following motor control training in people with recurrent low back pain. J Electromyogr Kinesiol 2008;18:55967. Tsao H, Hodges PW. Immediate changes in feedforward postural adjustments following voluntary motor training. Exp Brain Res 2007;181(4):53746. Tsao H, Tucker K, Hodges P. Changes in excitability of corticomotor inputs to the trunk muscles during experimentally-induced acute low back pain. submitted for publication. Tucker K, Butler J, Graven-Nielsen T, Riek S, Hodges P. Motor unit recruitment strategies are altered during deep-tissue pain. J Neurosci 2009;29(35):108206. Tucker K, Ingham D, Tsao H, Hodges P. Pain alone does not interfere with motor cortical plasticity. In Proceedings international society for electrophysiology and kinesiology, 2010. Tucker KJ, Hodges PW. Motoneurone recruitment is altered with pain induced in non-muscular tissue. Pain 2009;141(12):1515. Tucker KJ, Hodges PW. Changes in motor unit recruitment strategy during pain alters force direction. Eur J Pain 2010;14(9):9328. Tzagarakis GN, Tsivgoulis SD, Papagelopoulos PJ, Mastrokalos DS, Papadakis NC, Kampanis NA, et al. Inuence of acute anterior cruciate ligament deciency in gait variability. J Int Med Res 2010;38(2):51125. Van Dien JH, Cholewicki J, Radebold A. Trunk muscle recruitment patterns in patients with low back pain enhance the stability of the lumbar spine. Spine 2003;28(8):83441. van Dien JH, Selen LP, Cholewicki J. Trunk muscle activation in low-back pain patients, an analysis of the literature. J Electromyogr Kinesiol 2003;13(4):33351. Waddell G. The back pain revolution. Edinburgh: Churchill Livingstone; 1998. Wang K, Arima T, Arendt-Nielsen L, Svensson P. EMG-force relationships are inuenced by experimental jaw-muscle pain. J Oral Rehab 2000;27(5):394402. Warner JJ, Lephart S, Fu FH. Role of proprioception in pathoetiology of shoulder instability. Clin Orthop 1996;330:359. Wolf SL, Basmajian JV. Assessment of paraspinal electromyographic activity in normal subjects and chronic low back pain patients using a muscle biofeedback device. In: Asmussen E, Jorgensen K, editors. Biomechanics IVb. Baltimore: University Park Press; 1977. p. 31924. Zazulak BT, Ponce PL, Straub SJ, Medvecky MJ, Avedisian L, Hewett TE. Gender comparison of hip muscle activity during single-leg landing. J Orthop Sports Phys Ther 2005;35(5):2929. Zedka M, Prochazka A, Knight B, Gillard D, Gauthier M. Voluntary and reex control of human back muscles during induced pain. J Physiol (Lond) 1999;520(Pt 2):591604.
228
P.W. Hodges / Journal of Electromyography and Kinesiology 21 (2011) 220228
Paul Hodges Ph.D. Med. Dr. D.Sc. B.Phty. (Hons.) FACP is the Director of the Centre for Clinical Research Excellence in Spinal Pain, Injury and Health (CCRE SPINE) funded by the National Health and Medical Research Council (NHMRC) of Australia and is an NHMRC Senior Principal Research Fellow. He has 3 doctorates; one in physiotherapy and two in neuroscience. His research blends these skills to understand pain and control of movement. The large multidisciplinary research centre that he leads focuses on understanding pain physiology, and the development and testing of novel treatments. Recent work has led to the development of new understanding of the motor adaptation to pain. He has received numerous international research awards (including the 2006 ISSLS Prize for back pain research), published >200 scientic papers, presented >120 invited lectures at conferences in >30 countries, and received more than $AU22 million in research funds.
You might also like
- Risk Assessment Sheet For Installation of Wooden DoorsDocument3 pagesRisk Assessment Sheet For Installation of Wooden DoorsYash Sharma50% (2)
- Dry Needling Jan DommerholtDocument15 pagesDry Needling Jan DommerholtAléssio NovaisNo ratings yet
- Effects of Petrissage Massage On Fatigue and ExercDocument8 pagesEffects of Petrissage Massage On Fatigue and ExercJGRBBKDVRNo ratings yet
- Updates Clinical: International Association For The Study of PainDocument6 pagesUpdates Clinical: International Association For The Study of PainSuaeni Kurnia WirdaNo ratings yet
- Scientific Research Journal of India (SRJI) Vol - 2, Issue - 1, Year - 2013Document59 pagesScientific Research Journal of India (SRJI) Vol - 2, Issue - 1, Year - 2013Dr. Krishna N. SharmaNo ratings yet
- Introduction To Hoac II, ICF-RPS & OutcomeDocument40 pagesIntroduction To Hoac II, ICF-RPS & OutcomeKC MutiaNo ratings yet
- Ji-Hyun Lee - The Effect of Scapular Posterior Tilt ExerciseDocument8 pagesJi-Hyun Lee - The Effect of Scapular Posterior Tilt Exercisesebafigueroa94No ratings yet
- LaserDocument8 pagesLaserALİ YAVUZ KARAHANNo ratings yet
- ElectrogoniometerDocument3 pagesElectrogoniometerGaurav MolankarNo ratings yet
- CP PDFDocument7 pagesCP PDFannaNo ratings yet
- TENSDocument20 pagesTENSchandran2679100% (2)
- Do Sliders' Slide and Tensioners' Tension An Analysis of Neurodynamic Techniques and Considerations Regarding Their Application PDFDocument9 pagesDo Sliders' Slide and Tensioners' Tension An Analysis of Neurodynamic Techniques and Considerations Regarding Their Application PDFryanbroad82No ratings yet
- The Painful Dysfunctional ShoulderDocument3 pagesThe Painful Dysfunctional ShoulderAnanta Resti AyundariNo ratings yet
- Physiotherapy Pain CareDocument3 pagesPhysiotherapy Pain CareMuhammad Aurangzeb FahimNo ratings yet
- 03mb5 17 PDFDocument3 pages03mb5 17 PDFKhusnah KhauliyaNo ratings yet
- Aquatic Exercise & Balneotherapy in Musculoskeletal ConditionsDocument9 pagesAquatic Exercise & Balneotherapy in Musculoskeletal ConditionsAleCsss123No ratings yet
- Journal Pre-Proof: ExploreDocument43 pagesJournal Pre-Proof: ExploreLuís CorreiaNo ratings yet
- Floating Manipulative TherapyDocument7 pagesFloating Manipulative TherapyrahmatsahaquillaNo ratings yet
- 13 - Neural MobilizationDocument19 pages13 - Neural MobilizationAhmed MuflehNo ratings yet
- Effect of Dry Needling On Lumbar Muscle Stiffness in Patients With Low Back PainDocument11 pagesEffect of Dry Needling On Lumbar Muscle Stiffness in Patients With Low Back PainValeria AlfaroNo ratings yet
- Muscle Plasticity in Response To Electrical Stimulation: - Priyanka. Parate MPTH, PuneDocument35 pagesMuscle Plasticity in Response To Electrical Stimulation: - Priyanka. Parate MPTH, Punemilananand100% (1)
- REFERENCES REGARDING THE Neurocalometer and NervoscopeDocument5 pagesREFERENCES REGARDING THE Neurocalometer and NervoscopenicoNo ratings yet
- 1 Peripheral Manipulation Lecture OneDocument13 pages1 Peripheral Manipulation Lecture Onebuhlembatha304No ratings yet
- Pathophysiology of Spastic Paresis IDocument17 pagesPathophysiology of Spastic Paresis Ivarahamihir100% (2)
- Guidelines For Dry Needling Practice ISCP IrlandaDocument59 pagesGuidelines For Dry Needling Practice ISCP IrlandaDaniel Vargas100% (1)
- Effect of Maitland Spinal Mobilization Therapy Versus Conventional Therapy in Lumbar Spondylosis With RadiculopathyDocument8 pagesEffect of Maitland Spinal Mobilization Therapy Versus Conventional Therapy in Lumbar Spondylosis With RadiculopathyjuancaNo ratings yet
- Lecture Scap Malaga 2Document47 pagesLecture Scap Malaga 2danielaNo ratings yet
- Passive MovementsDocument21 pagesPassive MovementsElla Cooper100% (1)
- Scoliosis: Degenerative & IdiopathicDocument34 pagesScoliosis: Degenerative & IdiopathicClaudia MariscaNo ratings yet
- Application of Fascial Manipulation Technique in Chronic Shoulder PainDocument8 pagesApplication of Fascial Manipulation Technique in Chronic Shoulder PainEnyaw DroffatsNo ratings yet
- Galvanic CurrentundefinedundefinedDocument1 pageGalvanic CurrentundefinedundefinedYahia Tawfeek AlkilanyNo ratings yet
- Electronic Edge ExampleDocument138 pagesElectronic Edge Examplezarrin77No ratings yet
- A Proposed Evidence-Based Shoulder Special Testing Examination Algorithm - Clinical Utility Based On A Systematic Review of The LiteratureDocument14 pagesA Proposed Evidence-Based Shoulder Special Testing Examination Algorithm - Clinical Utility Based On A Systematic Review of The LiteratureAfonso MacedoNo ratings yet
- Fac 45 Handbook 2007Document233 pagesFac 45 Handbook 2007anon-963170100% (1)
- History of Physical TherapyDocument11 pagesHistory of Physical Therapyapi-271035341No ratings yet
- Pathophysiology of Skeletal Muscle InjuriesDocument32 pagesPathophysiology of Skeletal Muscle InjuriesZaroon Abdullah Khan100% (1)
- Kinetic Control Cap1Document17 pagesKinetic Control Cap1Yennifer Serna MoncadaNo ratings yet
- Theories of Pain and Its Application in PaediatricsDocument7 pagesTheories of Pain and Its Application in PaediatricsJamaru NishaNo ratings yet
- Therapybook Interferencial TherapyDocument34 pagesTherapybook Interferencial TherapyBrian RaymondNo ratings yet
- 4 UE Orthoses Part V - Elbow and ForearmDocument50 pages4 UE Orthoses Part V - Elbow and Forearmcorememories10100% (1)
- Physiotherapy in Disaster MenegementDocument82 pagesPhysiotherapy in Disaster MenegementAtiKa YuLiantiNo ratings yet
- Mulligan Concept IFI Kudus, 29 Oktober 2017-1Document84 pagesMulligan Concept IFI Kudus, 29 Oktober 2017-1Ilham Sii Pendekar Biru100% (1)
- The Theory and Techniques of Cupping TherapyDocument9 pagesThe Theory and Techniques of Cupping TherapymandrakeNo ratings yet
- A Practical Physiotherapy Approach in Intensive Care Unit: April 2019Document12 pagesA Practical Physiotherapy Approach in Intensive Care Unit: April 2019NSSNS BALAJINo ratings yet
- Advanced Physiotherapeutic SyllabusDocument1 pageAdvanced Physiotherapeutic SyllabusAnup SharmaNo ratings yet
- Muscle PhysioexDocument13 pagesMuscle PhysioexElvira BasilioNo ratings yet
- Lumbar Virtual Rounds 1 - 2021Document146 pagesLumbar Virtual Rounds 1 - 2021مركز ريلاكس للعلاج الطبيعي100% (1)
- Frozen Shoulder Review Nature 2022Document17 pagesFrozen Shoulder Review Nature 2022joaquinNo ratings yet
- AGE Max HR (220-Age) Max HR (208 - 0.7xage) : Maximum Heart RateDocument10 pagesAGE Max HR (220-Age) Max HR (208 - 0.7xage) : Maximum Heart RateJinaan MahmudNo ratings yet
- Joint Mobilizations PDFDocument1 pageJoint Mobilizations PDFErik TellezNo ratings yet
- Myofascial Pain SyndromeDocument4 pagesMyofascial Pain SyndromeHifnaDavesal'AyeshaNo ratings yet
- Rehabilitation Will Increase The Capacity of Your Insert Musculoskeletal Tissue Here Defining Tissue Capacity A Core Concept For CliniciansDocument3 pagesRehabilitation Will Increase The Capacity of Your Insert Musculoskeletal Tissue Here Defining Tissue Capacity A Core Concept For CliniciansChristhoper HermosillaNo ratings yet
- 2 51 1656420123 1ijmpsdec20221Document4 pages2 51 1656420123 1ijmpsdec20221TJPRC PublicationsNo ratings yet
- Serratus Anterior 2Document2 pagesSerratus Anterior 2api-659065431No ratings yet
- Superficial Versus Deep Dry Needling PDFDocument5 pagesSuperficial Versus Deep Dry Needling PDFludimilaGNo ratings yet
- Diadynamic CurrentDocument30 pagesDiadynamic CurrentvladNo ratings yet
- 10 Knee MobilizationDocument12 pages10 Knee MobilizationGautamNo ratings yet
- Myofascial ReleaseDocument8 pagesMyofascial Releaseprokin_martinezNo ratings yet
- Muhammed Kocabiyik Physical Medicine & Rehabilitation Iv. Class V. GroupDocument14 pagesMuhammed Kocabiyik Physical Medicine & Rehabilitation Iv. Class V. GroupsanalcrazyNo ratings yet
- Advances in Spinal Stabilization PDFDocument333 pagesAdvances in Spinal Stabilization PDFMateo CortesNo ratings yet
- SCBT User Guide - July 2012Document28 pagesSCBT User Guide - July 2012Mario SerraNo ratings yet
- The Independent 13 March 2016Document64 pagesThe Independent 13 March 2016artedlcNo ratings yet
- Presentation On General Insurance CompaniesDocument43 pagesPresentation On General Insurance Companiesskenkan50% (6)
- S I: N E S I Writing The Erasure of Emotions in Dystopian Young Adult Fiction: Reading Lois Lowry's TheDocument16 pagesS I: N E S I Writing The Erasure of Emotions in Dystopian Young Adult Fiction: Reading Lois Lowry's TheAlif KharuddinNo ratings yet
- Haven of Serenity PDFDocument75 pagesHaven of Serenity PDFVaal TraderzNo ratings yet
- Permission Is Granted Subject To The Following ConditionsDocument2 pagesPermission Is Granted Subject To The Following ConditionsShankar BanrwalNo ratings yet
- Process Validation 3 PDF FreeDocument26 pagesProcess Validation 3 PDF FreeSandro SotomayorNo ratings yet
- MVK Series: 105 1,000 2,000Hrs AssuredDocument5 pagesMVK Series: 105 1,000 2,000Hrs AssureddiegooliveiraEENo ratings yet
- Low Voltage Electrical Component of Electric Two - Three WheelerDocument6 pagesLow Voltage Electrical Component of Electric Two - Three WheelerENESH SOLANKINo ratings yet
- EDiscount Application 138Document2 pagesEDiscount Application 138Abdul JalaludinNo ratings yet
- Mapeh First Quarter Unit Test HealthDocument2 pagesMapeh First Quarter Unit Test HealthSeachiel Anagaran100% (1)
- Transformador Medir Corriente Alterna T75a11Document2 pagesTransformador Medir Corriente Alterna T75a11Jose BuferNo ratings yet
- NoticeDocument46 pagesNoticeZaneNo ratings yet
- Principles of Attic VentilationDocument20 pagesPrinciples of Attic VentilationSal BassNo ratings yet
- Risk Management Topic 1Document18 pagesRisk Management Topic 1Lucid LucidNo ratings yet
- Ashish KumarDocument4 pagesAshish Kumarmritunjay kumarNo ratings yet
- Aef3 File 5 WordlistDocument6 pagesAef3 File 5 WordlistYahya Al-AmeriNo ratings yet
- 5 Clamps Connectors 220 400kv SsDocument12 pages5 Clamps Connectors 220 400kv SsJaswanth SaiNo ratings yet
- Powerware BPIII Industrial UPS: FeaturesDocument4 pagesPowerware BPIII Industrial UPS: Featuresandy175No ratings yet
- Stoeckle Thaler Final Reduced 002Document30 pagesStoeckle Thaler Final Reduced 002Júnior SenseyNo ratings yet
- Diabetes Ielts Reading AnswersDocument2 pagesDiabetes Ielts Reading AnswersMohammed AbdallahNo ratings yet
- 2012 Year 11 Atar Wace Chemistry ExamDocument40 pages2012 Year 11 Atar Wace Chemistry ExamismailmarsiddiqueNo ratings yet
- JSA For DewateringDocument9 pagesJSA For DewateringAbdul WahabNo ratings yet
- Plantas Medicinales BoliviaDocument17 pagesPlantas Medicinales BoliviaNatalia Alejandra Gonzalez Sanchez100% (1)
- Bridgestone Behavioral Health Center: Cost-Volume-Profit (CVP) Analysis For Planning and ControlDocument8 pagesBridgestone Behavioral Health Center: Cost-Volume-Profit (CVP) Analysis For Planning and ControlAbbey Li0% (1)
- Lecture 7 Reforming and IsomerizationDocument5 pagesLecture 7 Reforming and IsomerizationMadhuri Gupta100% (1)
- Geography Paper Three NotesDocument160 pagesGeography Paper Three NotesOwor Kennedy100% (2)
- Abdominal Ultrasound in Cats and Dogs, An Illustrated Reference Value Guide (VetBooks - Ir)Document49 pagesAbdominal Ultrasound in Cats and Dogs, An Illustrated Reference Value Guide (VetBooks - Ir)Abril A. MendozaNo ratings yet
- Cat in The Rain EssayDocument7 pagesCat in The Rain Essayafhbctdfx100% (2)