The cardiac conduction system consists of the sinoatrial node, internodal pathways, atrioventricular node, bundle of His, and Purkinje fibers. The sinoatrial node acts as the primary pacemaker by generating electrical impulses slightly faster than other areas. It can be affected by the parasympathetic and sympathetic nervous systems. An electrocardiogram is used to record the heart's electrical activity through electrodes on the skin. It can detect abnormalities in heart rate, axis, intervals, and rhythms including various types of tachycardia and bradycardia. Atrial flutter, atrial fibrillation, ventricular tachycardia, and ventricular fibrillation are abnormal heart rhythms that appear
The cardiac conduction system consists of the sinoatrial node, internodal pathways, atrioventricular node, bundle of His, and Purkinje fibers. The sinoatrial node acts as the primary pacemaker by generating electrical impulses slightly faster than other areas. It can be affected by the parasympathetic and sympathetic nervous systems. An electrocardiogram is used to record the heart's electrical activity through electrodes on the skin. It can detect abnormalities in heart rate, axis, intervals, and rhythms including various types of tachycardia and bradycardia. Atrial flutter, atrial fibrillation, ventricular tachycardia, and ventricular fibrillation are abnormal heart rhythms that appear
The cardiac conduction system consists of the sinoatrial node, internodal pathways, atrioventricular node, bundle of His, and Purkinje fibers. The sinoatrial node acts as the primary pacemaker by generating electrical impulses slightly faster than other areas. It can be affected by the parasympathetic and sympathetic nervous systems. An electrocardiogram is used to record the heart's electrical activity through electrodes on the skin. It can detect abnormalities in heart rate, axis, intervals, and rhythms including various types of tachycardia and bradycardia. Atrial flutter, atrial fibrillation, ventricular tachycardia, and ventricular fibrillation are abnormal heart rhythms that appear
The cardiac conduction system consists of the sinoatrial node, internodal pathways, atrioventricular node, bundle of His, and Purkinje fibers. The sinoatrial node acts as the primary pacemaker by generating electrical impulses slightly faster than other areas. It can be affected by the parasympathetic and sympathetic nervous systems. An electrocardiogram is used to record the heart's electrical activity through electrodes on the skin. It can detect abnormalities in heart rate, axis, intervals, and rhythms including various types of tachycardia and bradycardia. Atrial flutter, atrial fibrillation, ventricular tachycardia, and ventricular fibrillation are abnormal heart rhythms that appear
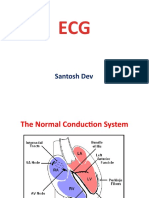
SA node also called the sinus node is the impulse-generating (pacemaker) tissue located in the right atrium of the heart SA node is a generator of sinus rhythm (60100/min) these cells are modified cardiac myocytes.
Role as a pacemaker Although all of the heart's cells possess the ability to generate the electrical impulses that trigger cardiac contraction, the sinoatrial node normally initiates it, simply because it generates impulses slightly faster than the other areas with pacemaker potential. Because the sinoatrial node is responsible for the rest of the heart's electrical activity, it is sometimes called the primary pacemaker.
Role as a pacemaker If the SA node does not function, or the impulse generated in the SA node is blocked before it travels down the electrical conduction system, a group of cells further down the heart will become the heart's pacemaker
Innervation of the SA node
The SA node is richly innervated by parasympathetic nervous system fibers (CN X) and by sympathetic nervous system fibers (Spinal Nerve). Stimulation of the vagus nerve (the parasympathetic fibers) causes a decrease in the SA node rate. Stimulation via sympathetic fibers causes an increase in the SA node rate (thereby increasing the heart rate and force of contraction)
ECG The ECG is a recording of the activity of the heart. The electrical currents generated by the heart spread throught the body to the skin, where they can be sensed by appropiately placed electrodes.
ECG Adventages: Very cheap diagnostic metod Available Easy to do Disadventages: No 100% specyfic diagnostic metod
How to do ECG???
Limb leads
Placement of electrodes ???
ECG C
Precordial leads Limb leads
V1 V2 V3 V4
In the fourth intercostal space (between ribs 4 & 5) just to the right of the sternum (breastbone). In the fourth intercostal space (between ribs 4 & 5) just to the left of the sternum. Between leads V2 and V4.
In the fifth intercostal space (between ribs 5 & 6) in the mid-clavicular line (the imaginary line that extends down from the midpoint of the clavicle (collarbone). Horizontally even with V4, but in the anterior axillary line. (The anterior axillary line is the imaginary line that runs down from the point midway between the middle of the clavicle and the lateral end of the clavicle; the lateral end of the collarbone is the end closer to the arm.) Horizontally even with V4 and V5 in the midaxillary line. (The midaxillary line is the imaginary line that extends down from the middle of the patient's armpit.)
V5
V6
V1: right 4th intercostal space V2: left 4th intercostal space V3: halfway between V2 and V4
V4: left 5th intercostal space, mid-clavicular line
V5: horizontal to V4, anterior axillary line
V6: horizontal to V5, mid-axillary line
Precordial leads
Holter monitor is named for Dr. Norman J. Holter who invented telemetric cardiac monitoring in 1949 is a portable device for continuously monitoring various electrical activity of the central nervous system for at least 24 hours. The most common use is for monitoring the heart or ECG, but can also be used for monitoring EEG
Therapeutic use of Holter monitor
And olso another therapeutic use
Difrencess between interval and segmet
Normal ECG
Diagram of the ECG and representative depolarrization and repolarization of the atria and ventricle
Normal ECG It is important to remember that there is a wide range of normal variability in the 12 lead ECG. Measurements Heart Rate: 60 - 90 bpm PR Interval: 0.12 - 0.20 sec QT Interval (QTc 0.40 sec) P duration < 0.12 sec and P amplitude < 2.5 mm QRS duration 0.12 sec
Normal ECG Rhythm Normal sinus rhythm: the P wave before every QRS complex and in leads I and II must be upright (positive) if the rhythm is coming from the sinus node. Axis The normal QRS axis should be between - 30 and +90 degrees
Axis The fastest, non-specific method to determine the QRS axis is to find the major direction of the QRS complex (positive or negative) in leads I and aVF. If the QRS complex is upright (positive) in both lead I and lead aVF, then the axis is normal (see the picture).
Axis If the QRS is upright in lead I and downward (negative) in lead aVF, then the axis is between 0 and -90 degrees, likely left axis deviation. However, in this scenario the axis could fall between 0 and -30 which is technically a normal QRS axis. To further distinguish normal from left axis deviation in this setting, look at lead II. If lead II is downward (negative), then the axis is more towards -90 and left axis deviation is present. If the QRS complex in lead II is upright (positive), then the axis is more towards 0 degrees and the QRS axis is normal.
Axis If the QRS is predominantly downward in both leads I and aVF, then the axis is indeterminate. If the QRS is downward (negative) in lead I and upward (positive) in lead aVF, then the axis is rightward.
Heart Rate Because ECG paper usually moves at a standardized 25mm/sec, the vertical lines can be used to measure time. There is a 0.20 sec between 2 of the large lines. Therefore, if you count the number of heart beats (QRS complexes) in between 30 large boxes (6 seconds) and multiply by 10, you have beats per minute. Conveniently, ECG paper usually has special markings every 3 seconds so you don't have to count 30 large boxes.
Bradycardia is defined as a resting heart rate of under 60 beats per minute Classification: Atrial bradycardia Atrioventricular nodal bradycardia Ventricular bradycardia
Causes of bradycardia 1. Cardiac causes (acute or chronic ischemic heart disease, valvular heart disease, or degenerative primary electrical disease)
2. Non-cardiac causes (drug use, metabolic
or endocrine issues, especially in the thyroid)
Tachycardia In tachycardia, heart pumps less efficiently and provides less blood flow to the rest of the body, including the heart itself. The increased heart rate also leads to increased work and oxygen demand for the myocardium, which can cause a heart attack if it persists.
Causes of tachycardia Autonomic causes Endocrine causes Hemodynamic responses - If blood pressure decreases, the heart beats faster in an attempt to raise it. This is called r e f l ex ta c hy c a r d i a . This can happen in response to a decrease in blood volume (through dehydration or bleeding), or an unexpected change in blood flow.
Types of tachycardia Sinus tachycardia Ventricular tachycardia Supraventricular tachycardia rhythms include: Atrial fibrillation AV nodal reentrant tachycardia (AVNRT) AV reentrant tachycardia (AVRT) Junctional tachycardia
Atrial flutter It is a supraventricular tachcardia an atrial rate of ap. 240 to 350 beats/minute the impact and symptoms of atrial flutter depend on the heart rate of the patient it is usually associated with a fast heart rate or tachycardia (230380/minute)
Heart rate is a measure of the ventricular rather than atrial activity in atrial flutter and atrial firbillation the AV node exerts a protective effect on heart rate by blocking atrial impulses in excess of about 180 beats/minute (If the flutter rate is 300/minute only half of these impulses will be conducted, giving a ventricular rate of 150/minute, or a 2:1 heart block)
Atrial flutter
Atrial fibrillation (AF)
is the most common cardiac arrhythmia It is a supraventricular tachycardia indicator of AF is the absence of P waves on an ECG, which are normally present when there is a coordinated atrial contraction at the beginning of each heart beat risk increases with age, 8% of people over 80 having AF
Atrial fibrillation Atrial fibrillation is diagnosed on an electrocardiogram (ECG), an investigation performed routinely whenever an irregular heart beat is suspected.
Atrial fibrillation Characteristic are the absence of P waves, with unorganized electrical activity in their place, and irregular R-R intervals due to irregular conduction of impulses to the ventricles
Sinus rhythm
Atriall fibryllation
Classification of atrial fibrillation
AF Category Defining Characteristics
First detected
only one diagnosed episode recurrent episodes that self-terminate in less than 7 days recurrent episodes that last more than 7 days an ongoing long-term episode and accepted
Paroxysmal
Persistent
Permanent
Management of atrial fibrillation
Electrical cardioversion involves the restoration of normal heart rhythm through the application of a electrical shock. Chemical cardioversion is performed with drugs (amiodarone)
Cardioversion energy corresponds to the R wave of the QRS complex on the ECG.
Ventricular tachycardia HR >100/min that originates in one of the ventricles of the heart Ventricular tachycardia can be classified based on its morphology Monomorphic ventricular tachycardia Polymorphic ventricular tachycardia
Non-sustained ventricular tachycardia.
Polymorphic ventricular tachycardia or Torsades de Pointes.
Ventricular flutter over 200 beats/min it is characterized on the ECG by a sinusoidal waveform without clear definition of the QRS and T waves ventricular fibrillation
Ventricular fibrillation (VF)
is a condition in which there is uncoordinated contraction of the cardiac muscle of the ventricles in the heart. when this happens, chambers contract in a rapid, unsynchronized way. The heart pumps little or no blood.
S TA R T C P R ! ! !
Ventricular fibrillation (VF)
ventricular fibrillation is very serious event. collapse and sudden cardiac death will follow in minutes unless medical help is provided immediatel to STOP VF defibrillator
Defibrillation is the definitive treatment for the lifethreatening cardiac arrhythmias: ventricular fibrillation and pulseless ventricular tachycardia terminates the arrhythmia, and allows normal sinus rhythm to be reestablished by the body's natural pacemaker, in the sinoatrial node of the heart.
cardioverter-defibrillator Today one effective way to correct lifethreatening rhythms is by using an electronic device called an implantable cardioverterdefibrillator (ICD). This device shocks the heart to normalize the heartbeat if the heart's own electrical signals become disordered.
cardioverter-defibrillator
cardioverter-defibrillator
Heart Block
A heart block is a disease in the electrical system of the heart. A heart block can be a blockage at any level of the electrical conduction system of the heart.
Types of heart block
Blocks that occur within the sinoatrial node (SA node) are described as S A n o d a l b l o c k s . Blocks that occur within the atrioventricular node (AV node) are described as AV n o d a l b l o c k s . Blocks that occur below the AV node are known as i n f ra H i s i a n b l o c k s ( n a m e d a f te r t h e b u n d l e o f H i s ) . Blocks that occur within the left or right bundle branches are known as b u n d l e b ra n c h b l o c k s . Blocks that occur within the fascicles of the left bundle branch are known as h e m i b l o c k s .
First-degree AV heart block
First-degree heart block, or first-degree AV block, is when the electrical impulse moves through the AV node more slowly than normal. The time it takes for the impulse to get from the atria to the ventricles (the PR interval) should be less than about 0.2 seconds. If it takes longer than this, it's called first-degree heart block.
First-degree heart block
What is a second-degree heart block?
In this condition, some signals from the atria don't reach the ventricles. This causes "dropped beats." On an ECG, the P wave isn't followed by the QRS wave, because the ventricles weren't activated
There are two types of second-degree heart block :
Type I second-degree heart block, or Mobitz Type I, or Wenckebach's AV block. Electrical impulses are delayed more and more with each heartbeat until a beat is skipped. This condition is not too serious but sometimes causes dizziness and/or other symptoms. Type II second-degree heart block, or Mobitz Type II. This is less common than Type I but generally more serious. Because electrical impulses can't reach the ventricles, an abnormally slow heartbeat may result. In some cases a pacemaker is needed.
Mobitz Type I = Wenckebach's AV block
Mobitz Type II
Third-degree heart block
Complete heart block, also referred to as thirddegree atrioventricular (AV) block is a disorder of the cardiac conduction system where there is no conduction through the AV node
SA impulse is blocked and an accessory pacemaker in the lower chambers will typically activate the ventricles.
Third-degree heart block
Since this accessory pacemaker also activates independently of the impulse generated at the SA node, two independent rhythms can be noted on the electrocardiogram (ECG). One of the most important characteristic of this block is the absolute absence of the opportunity for atrial impulses to enter and capture the ventricles
Third-degree heart block
the most common cause is coronary ischemia
Third-degree heart block
Left ventricular hypertrophy
while ventricular hypertrophy occurs naturally as a reaction to aerobic exercise and strength training, it is most frequently referred to as a pathological reaction to cardiovascular disease, or high blood pressure.
The principal method to diagnose LVH is echocardiography
Left ventricular hypertrophy
Sokolow + Lyon (Am Heart J, 1949;37:161) S in V1 + R in V5 or V6 (whichever is larger) 35 mm R in aVL 11 mm
Left ventricular hypertrophy
Right ventricular hypertrophy
Right ventricular hypertrophy is commonly associated with any form of right ventricular outflow obstruction or pulmonary hypertension
Wolf-Parkinson-White Syndrome (WPW)
This is characterized by an extra electrical pathway (bypass tract) that is present at birth The bypass tract connects the atrium to the ventricle and conducts the electrical impulse between upper and lower chambers more quickly than the normal conduction pathway. WPW is also dangerous in patients who have atrial fibrillation, because the rapid, chaotic atrial impulses in the atrium can travel through the bypass tract to the ventricle and result in a very rapid heart rate.
Wolf-Parkinson-White Syndrome
Wolff-Parkinson-White syndrome Ventricular Pre-excitation is represented by the short P-R interval, wide QRS complex, and delta wave
Long QT syndrome (LQTS)
is a congenital disorder characterized by a prolongation of the QT interval on ECG and a propensity to ventricular tachyarrhythmias, which may lead to syncope, cardiac arrest, or sudden death. the QT interval on the ECG, measured from the beginning of the QRS complex to the end of the T wave, represents the duration of activation and recovery of the ventricular myocardium
QTc QT intervals corrected for heart rate (QTc) longer than 0.44 seconds are generally considered abnormal, however a normal QTc can be more prolonged in females (up to 0.46 sec). The Bazett formula is used to calculate the QTc, as follows:
QTc = QT/square root of the R-R interval.
Long QT syndrome In LQTS, QT prolongation can lead to polymorphic ventricular tachycardia, or torsade de pointes, which itself may lead to ventricular fibrillation and sudden cardiac death.
Acute myocardial infarction
non-ST-elevated myocardial infarction
ST-elevated myocardial infarction
Localization of ischemia
V1-V4 correspond to the anterior wall
II, III, aVF correspond to the inferior wall V5, V6, I, aVL correspond to the lateral wall
The changes in the ECG
The changes in the ECG are seen in the leads adjacent to the infarct. In the first few hours the T waves become abnormally tall and the ST segments begin to rise. In the first 24 hours the T wave will become inverted, as the ST elevation begins to resolve. Pathological Q waves may appear within hours or may take greater than 24 hr. Long term changes of ECG include persistent Q waves in 90% In non Q-wave infarcts, ST depression and T wave inversion occur without ST elevation.
Sequence of Changes in Myocardial Infarction
Sudden cardiac death.
is death resulting from an abrupt loss of heart function. The victim may or may not have diagnosed heart disease. The time and mode of death are unexpected. It occurs within minutes after symptoms appear. The most common underlying reason for patients to die suddenly from cardiac arrest is coronary heart disease.
Causes of sudden cardiac death
Most of the cardiac arrests that lead to sudden death occur when the electrical impulses in the diseased heart become rapid (ventricular tachycardia) or chaotic (ventricular fibrillation) or both. This irregular heart rhythm (arrhythmia) causes the heart to suddenly stop beating