Dot
Dot
Download as pdf or txt
You might also like
- Operation Press ReleaseDocument9 pagesOperation Press ReleaseGoMNNo ratings yet
- National Immunization ScheduleDocument1 pageNational Immunization ScheduleSudheer100% (1)
- Cardiac Diet HandoutDocument2 pagesCardiac Diet Handoutapi-537434972No ratings yet
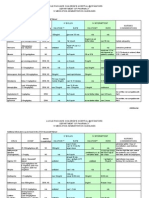
- Table 3. Treatment Regimens: F. Treatment Regimens by Category - The Following Abbreviations MeanDocument3 pagesTable 3. Treatment Regimens: F. Treatment Regimens by Category - The Following Abbreviations MeanKevin Leo Lucero AragonesNo ratings yet
- Drug Evaluation MonographDocument12 pagesDrug Evaluation MonographYodaheNo ratings yet
- Tenofovir DisoproxilDocument9 pagesTenofovir DisoproxiliftikharNo ratings yet
- Oxaliplatin Monograph 1dec2016Document9 pagesOxaliplatin Monograph 1dec2016Nadial UzmahNo ratings yet
- WHO Safe PrescribingDocument16 pagesWHO Safe PrescribingAliyah NatasyaNo ratings yet
- Annex I National Leprosy Eradication ProgrammeDocument5 pagesAnnex I National Leprosy Eradication ProgrammespmdocNo ratings yet
- Case Presentation On Systemic Lupus Erythematosus (SLE) : Presented By: Mahitha Karimsetti 616175802018 Pharm. D InternDocument35 pagesCase Presentation On Systemic Lupus Erythematosus (SLE) : Presented By: Mahitha Karimsetti 616175802018 Pharm. D Internsrija vijjapuNo ratings yet
- JINGCO - BSN 2-D - Module-6-Drug-StudyDocument16 pagesJINGCO - BSN 2-D - Module-6-Drug-StudyJashtine JingcoNo ratings yet
- CaffeineDocument2 pagesCaffeineSaini Malkeet100% (1)
- TizanidineDocument2 pagesTizanidinebhawanisrNo ratings yet
- Pcos QuizDocument12 pagesPcos QuizHimani VermaNo ratings yet
- Tranexamic AcidDocument18 pagesTranexamic AcidFatima Love Ariate-ArcasetasNo ratings yet
- Gastrointestinal DrugsDocument23 pagesGastrointestinal Drugsarifudin100% (1)
- Equivalent To Caffeine 5mg/ml Equivalent To Caffeine 5mg/mlDocument2 pagesEquivalent To Caffeine 5mg/ml Equivalent To Caffeine 5mg/mlatawa1No ratings yet
- ULIPRISTALDocument22 pagesULIPRISTALmeenakshi sundaramNo ratings yet
- Intrauterine Growth RestrictionDocument7 pagesIntrauterine Growth RestrictionNurfazlinaNo ratings yet
- JDI65eqHTQikUXfRIKaG - Schizophrenia PPT SlidesDocument24 pagesJDI65eqHTQikUXfRIKaG - Schizophrenia PPT SlidesKreshnik IdrizajNo ratings yet
- MethergineDocument3 pagesMethergineJohn AlanoNo ratings yet
- Dystocia: A Case PresentationDocument63 pagesDystocia: A Case PresentationRoxanneGailBigcasGoleroNo ratings yet
- Klinefelter SyndromeDocument15 pagesKlinefelter SyndromeصادقNo ratings yet
- Diabetes Mellitus (D9)Document92 pagesDiabetes Mellitus (D9)Alishba MushtaqNo ratings yet
- Folic Acid Presentation PDFDocument13 pagesFolic Acid Presentation PDFAngela IlustrisimoNo ratings yet
- Informed Consent PPT (Priyanka Kodule)Document8 pagesInformed Consent PPT (Priyanka Kodule)shubhamNo ratings yet
- NifedipineDocument2 pagesNifedipineapi-3797941100% (3)
- Drug Information Resources To PostDocument91 pagesDrug Information Resources To PostAhmad RjoubNo ratings yet
- Zollinger-Ellison Syndrome (Gastrinoma)Document15 pagesZollinger-Ellison Syndrome (Gastrinoma)Huy QuangNo ratings yet
- Drug AdvilDocument1 pageDrug AdvilDiana Laura LeiNo ratings yet
- Tamoxifen CitrateDocument3 pagesTamoxifen Citrateapi-3797941No ratings yet
- MisoprostolDocument2 pagesMisoprostolDr-Jagadeesh MangamooriNo ratings yet
- 2 Management of Menorrhagia (Heavy Menstrual Bleeding)Document36 pages2 Management of Menorrhagia (Heavy Menstrual Bleeding)Malak Ahmed 2295No ratings yet
- Risk Factors of Cesarean Delivery Due To Cephalopelvic Disproportion in Nulliparous Women at Sisaket HospitalDocument7 pagesRisk Factors of Cesarean Delivery Due To Cephalopelvic Disproportion in Nulliparous Women at Sisaket HospitalManangioma ManNo ratings yet
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocument9 pagesDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoNo ratings yet
- Prepared By: Manisha Thapa Leeza ShresthaDocument12 pagesPrepared By: Manisha Thapa Leeza ShresthaManjesh Mishra XettriNo ratings yet
- Research On Breast Self ExaminationDocument46 pagesResearch On Breast Self ExaminationDISNEY CYBERNo ratings yet
- 4 THROMBOLYTIC DRUGS by DR Azmat AliDocument90 pages4 THROMBOLYTIC DRUGS by DR Azmat AliAhmed YTNo ratings yet
- FlagylDocument3 pagesFlagylAdrianne BazoNo ratings yet
- Heparin LitigationDocument34 pagesHeparin LitigationjvalgalNo ratings yet
- FON (Subj) 2009-2022 GNM 1st YrDocument20 pagesFON (Subj) 2009-2022 GNM 1st YrgrowandreformNo ratings yet
- Prevention of Dental Caries: Name:Huda Khan ROLL #: 753Document33 pagesPrevention of Dental Caries: Name:Huda Khan ROLL #: 753Hudh HudNo ratings yet
- Isoprenaline Infusion 2016Document3 pagesIsoprenaline Infusion 2016Glory Claudia KarundengNo ratings yet
- Antepartum & Postpartum Hemorrhage (APH &PPH) : Anita DeodharDocument81 pagesAntepartum & Postpartum Hemorrhage (APH &PPH) : Anita DeodharAnjali Rahul AjmeriNo ratings yet
- Web KFOG-jan-11Document16 pagesWeb KFOG-jan-11kutra3000No ratings yet
- NonStress TestDocument2 pagesNonStress TestRama_ichiNo ratings yet
- History and Objectives of Post Marketing SurveillanceDocument14 pagesHistory and Objectives of Post Marketing SurveillanceSohit Gupta100% (1)
- Respiratory ArrestDocument4 pagesRespiratory Arrestbrain_warming25No ratings yet
- Generic Name: VORICONAZOLE Brand Name: Vfend Classification: Azole Antifungal Dosage/frequency and RouteDocument26 pagesGeneric Name: VORICONAZOLE Brand Name: Vfend Classification: Azole Antifungal Dosage/frequency and Routeanne marieNo ratings yet
- Pyridoxine 50mg Tablets - Summary of Product Characteristics (SMPC)Document3 pagesPyridoxine 50mg Tablets - Summary of Product Characteristics (SMPC)OdunlamiNo ratings yet
- Prostaglandin Drugs 1Document19 pagesProstaglandin Drugs 1darkmagicdrakeNo ratings yet
- Name of Drug Mechanism of Action Indications Contra-Indications Side Effects Nursing ConsiderationsDocument10 pagesName of Drug Mechanism of Action Indications Contra-Indications Side Effects Nursing ConsiderationsmidskiescreamzNo ratings yet
- PonstanDocument5 pagesPonstanYou know whoNo ratings yet
- Mesna: Mesna, Sold Under The BrandDocument17 pagesMesna: Mesna, Sold Under The BrandAndry HamdaniNo ratings yet
- Deep Vein ThrombosisDocument22 pagesDeep Vein ThrombosisEznal MahidinNo ratings yet
- G.2 Cannabis Use and Misuse PPT 2019Document50 pagesG.2 Cannabis Use and Misuse PPT 2019Echipa SiposNo ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- NTP MOP 6th ED Patient-Centered Approach To TB CareDocument24 pagesNTP MOP 6th ED Patient-Centered Approach To TB CarebambangtaguighcNo ratings yet
- Patient Adherence To Tuberculosis Treatment: U.S. Department of Health and Human Services Public Health ServiceDocument126 pagesPatient Adherence To Tuberculosis Treatment: U.S. Department of Health and Human Services Public Health ServicePriscilia FooNo ratings yet
- EGA Factsheet 01Document1 pageEGA Factsheet 01Rajeeb Chandra ShahaNo ratings yet
- Drug CounterfeitingDocument19 pagesDrug CounterfeitingmacamareNo ratings yet
- An Open-Label, Randomized, Cross-Over Bioequivalence Study of Lafutidine 10 MG Under Fasting ConditionDocument7 pagesAn Open-Label, Randomized, Cross-Over Bioequivalence Study of Lafutidine 10 MG Under Fasting ConditionRaghu ChimsNo ratings yet
- Training-Module-MERS - (Manual Reporting)Document23 pagesTraining-Module-MERS - (Manual Reporting)Farmasi KKPDNo ratings yet
- NCLEX Review ExamplefinalDocument52 pagesNCLEX Review Examplefinalisapatrick8126100% (1)
- Ethics in Pharmaceutical Marketing PDFDocument2 pagesEthics in Pharmaceutical Marketing PDFKevinNo ratings yet
- Rencana Kebutuhan Obat 2019 Puskesmas Banyumas: 01. Anti InfektivesDocument11 pagesRencana Kebutuhan Obat 2019 Puskesmas Banyumas: 01. Anti Infektivespkm baturradenNo ratings yet
- MucoLoxSpecSheet PRACTDocument2 pagesMucoLoxSpecSheet PRACTfrancisNo ratings yet
- Buspirone Hydrochloride (Drug Study)Document2 pagesBuspirone Hydrochloride (Drug Study)Franz.thenurse6888100% (1)
- Aluminum HydroxideDocument3 pagesAluminum HydroxideCay SevillaNo ratings yet
- Medication DilutionDocument22 pagesMedication DilutionYaser Salman100% (1)
- Marri Laxman Reddy Institute of Pharmacy: Patient Medication History Interview FormDocument3 pagesMarri Laxman Reddy Institute of Pharmacy: Patient Medication History Interview FormRaghu VenkatNo ratings yet
- Essential Drug List Updated For L1, L2 & L3 PDFDocument4 pagesEssential Drug List Updated For L1, L2 & L3 PDFAjay PandeyNo ratings yet
- A Clinical Guide To URINE DRUG TESTING PDFDocument26 pagesA Clinical Guide To URINE DRUG TESTING PDFTavo ANo ratings yet
- International Journal of Research in Pharmacy and ScienceDocument10 pagesInternational Journal of Research in Pharmacy and ScienceAat Prayoga MuhtarNo ratings yet
- Alcaine 0.5% Eye Drops: What Is in This LeafletDocument3 pagesAlcaine 0.5% Eye Drops: What Is in This Leafletdarla ryanNo ratings yet
- SeroquelDocument2 pagesSeroquelNinoska Garcia-Ortiz100% (2)
- Daftar Obat Aman Dan Bahaya Ibu HamilDocument8 pagesDaftar Obat Aman Dan Bahaya Ibu HamilAnnida Nurul Haq80% (5)
- Safe Paediatric and Obstetric Book 2015Document66 pagesSafe Paediatric and Obstetric Book 2015Maaida MuzaffarNo ratings yet
- Price List Dos Ni Roha Update Jan 2017Document100 pagesPrice List Dos Ni Roha Update Jan 2017wayan trisna erawatiNo ratings yet
- EyeDocument12 pagesEyePatziedawn GonzalvoNo ratings yet
- Drug ListDocument8 pagesDrug ListpeachandmintsNo ratings yet
- PP8 Launch1995 1997Document107 pagesPP8 Launch1995 1997Gabriel MontagniniNo ratings yet
- Final - GSK Vs Ranbaxy-2012Document14 pagesFinal - GSK Vs Ranbaxy-2012Nikhil B MNo ratings yet
- The Common Cold GuideDocument27 pagesThe Common Cold Guidehappyscottlee3438No ratings yet
- OxytocinDocument1 pageOxytocinSubbie OutlierNo ratings yet
- Tabel Obat ObatanDocument7 pagesTabel Obat ObatanMega Suciati100% (1)
- New Prescription For Drug Makers - Update The Plants - WSJDocument5 pagesNew Prescription For Drug Makers - Update The Plants - WSJStacy Kelly100% (1)
- Anti-Diabetic Medication - Wikipedia, The Free EncyclopediaDocument12 pagesAnti-Diabetic Medication - Wikipedia, The Free Encyclopediaumesh123patilNo ratings yet