Antibody Detection
Antibody Detection
Download as docx, pdf, or txt
You might also like
- Tooth by ToothDocument4 pagesTooth by Toothrakhee karNo ratings yet
- Troubleshooting in CXMDocument3 pagesTroubleshooting in CXMquerokeropi100% (1)
- B Blab 7 Panel Spring 2012Document16 pagesB Blab 7 Panel Spring 2012pzaballero7063No ratings yet
- Urinalysis and Body Fluids for Cls & MltFrom EverandUrinalysis and Body Fluids for Cls & MltNo ratings yet
- Study Stack - ASCP Coag Hematology Table ReviewDocument2 pagesStudy Stack - ASCP Coag Hematology Table Review장주연100% (1)
- Detection of AntibodiesDocument7 pagesDetection of AntibodiesJezreeljeanne Largo Caparoso100% (1)
- Wallis Budge Book of Am TuatDocument120 pagesWallis Budge Book of Am TuatRCEB100% (5)
- Phil Iri English 4 and 6Document6 pagesPhil Iri English 4 and 6JM GalvezNo ratings yet
- Wiki Abdomen Mcqs ExplainedDocument9 pagesWiki Abdomen Mcqs Explainedchemptnk100% (2)
- SPEAKER: Dr. Subhajit Das MODERATOR: Prof. Jyoti ShuklaDocument25 pagesSPEAKER: Dr. Subhajit Das MODERATOR: Prof. Jyoti Shuklaswaraj sharma100% (2)
- 2.5 Antibody ScreeningDocument5 pages2.5 Antibody ScreeningBALAJI100% (1)
- Antibody Screening - Kupang - 2016Document59 pagesAntibody Screening - Kupang - 2016yuni.kartika.ndoen92No ratings yet
- Antibody Detection and IdentificationDocument19 pagesAntibody Detection and IdentificationErika Leah ManaloNo ratings yet
- The Antiglobulin Test (Coomb's Test) Direct & Indirect: Group 1Document23 pagesThe Antiglobulin Test (Coomb's Test) Direct & Indirect: Group 1Marj Mendez100% (1)
- New Microsoft Word DocumentDocument7 pagesNew Microsoft Word DocumentDocAxi Maximo Jr AxibalNo ratings yet
- BB - Detection and Identification of AntibodiesDocument10 pagesBB - Detection and Identification of AntibodiesWayne VillalunaNo ratings yet
- Blood Component PreparationDocument24 pagesBlood Component PreparationLaiba ArshadNo ratings yet
- Blood Bank TypingDocument34 pagesBlood Bank TypingSkylarNo ratings yet
- Gel TechnologyDocument2 pagesGel TechnologyJai Carungay100% (1)
- Minor Blood Groups Part 1Document15 pagesMinor Blood Groups Part 1Mary Shikha ShaikeNo ratings yet
- Antibody Identification - IIDocument50 pagesAntibody Identification - IISimon Onsongo50% (2)
- Antibody ScreeningDocument57 pagesAntibody ScreeningSebastian Jake John100% (1)
- Abs Elu HandoutDocument6 pagesAbs Elu HandoutSiti Fadhilla TsabithaNo ratings yet
- Blood Group Systems ISBTDocument25 pagesBlood Group Systems ISBTkusumahpratiwi100% (1)
- Definitions: CLS 422 Clinical Immunohematology I Absorption and ElutionDocument6 pagesDefinitions: CLS 422 Clinical Immunohematology I Absorption and ElutionTrang HuynhNo ratings yet
- Miner Blood Group SystemDocument44 pagesMiner Blood Group SystemArshad RazaqNo ratings yet
- Immunohematology ASCPi Review Booklet (Part 1)Document22 pagesImmunohematology ASCPi Review Booklet (Part 1)Mark Justin OcampoNo ratings yet
- Antibody Screening and Identification ObjectivesDocument3 pagesAntibody Screening and Identification ObjectivesApril Sudario100% (1)
- Adverse Reaction Blood BankDocument10 pagesAdverse Reaction Blood BankyourfamilydoctorNo ratings yet
- Chapter 14 - Routine and Point of Care Testing in HematologyDocument10 pagesChapter 14 - Routine and Point of Care Testing in HematologyNathaniel Sim100% (1)
- Flashcards in Abo Blood GroupDocument10 pagesFlashcards in Abo Blood GroupVincent ReyesNo ratings yet
- 13 Other Blood Group SystemsDocument56 pages13 Other Blood Group SystemsCarinaJongLeeNo ratings yet
- Compatibility Testing: Week 5Document33 pagesCompatibility Testing: Week 5Bridgette100% (1)
- Coombs Test FreddyDocument11 pagesCoombs Test FreddyFreddy Vallejo LeonNo ratings yet
- Blood Bank2Document85 pagesBlood Bank22131443No ratings yet
- Compatibility Testing: Dr. Mohammed H Saiem Aldahr Blood Bank 3 Medical TechnologyDocument44 pagesCompatibility Testing: Dr. Mohammed H Saiem Aldahr Blood Bank 3 Medical TechnologyAnne Lorraine Margarette DulayNo ratings yet
- ABOsystemDocument52 pagesABOsystemJasmine HannahNo ratings yet
- Transfusion Training Checklist May 2015Document5 pagesTransfusion Training Checklist May 2015dhe100% (1)
- Lesson 07 PDFDocument14 pagesLesson 07 PDFIhsan UllahNo ratings yet
- Gel Card TechnologyDocument21 pagesGel Card TechnologyDominic BernardoNo ratings yet
- ABO Discrepancies - RahulDocument47 pagesABO Discrepancies - RahulNyxa AbdullaNo ratings yet
- ImmunohematologyDocument4 pagesImmunohematologyosama1381971100% (1)
- Blood Bak Process MapDocument1 pageBlood Bak Process MapspanwzNo ratings yet
- Antibody IdentificationDocument27 pagesAntibody Identificationhamaada100% (2)
- Red Cell and White Cell Counting, BloodDocument89 pagesRed Cell and White Cell Counting, BloodJovel Gangcuangco100% (1)
- ImmunohematologyDocument67 pagesImmunohematologyRainbow SherbetNo ratings yet
- Blood Bank EbookDocument14 pagesBlood Bank EbookNomer Formeloza BarlisNo ratings yet
- Resolution of Abo DiscrepanciesDocument4 pagesResolution of Abo DiscrepanciesPatrick MabugatNo ratings yet
- Antibody TitrationDocument14 pagesAntibody Titrationalibayaty1No ratings yet
- Blood Component TherapyDocument13 pagesBlood Component Therapymcbenze1607No ratings yet
- Lesson 22 PDFDocument5 pagesLesson 22 PDFfaeNo ratings yet
- Pocket Guide On Red Cells 2012Document8 pagesPocket Guide On Red Cells 2012Dave OrlandoNo ratings yet
- Blood Bank 4 DiscpDocument20 pagesBlood Bank 4 DiscpHector de la Cruz100% (1)
- Blood BankDocument84 pagesBlood Bankmanni1001100% (4)
- 1 Edited My Class Note 1 On Blood BankDocument42 pages1 Edited My Class Note 1 On Blood Bankmatewos100% (1)
- Correctly: IncorrectlyDocument70 pagesCorrectly: IncorrectlyDjdjjd Siisus100% (1)
- Blood Banking - Component PreparationDocument34 pagesBlood Banking - Component PreparationLentoOt EksDiiNo ratings yet
- Blood Bank IDocument136 pagesBlood Bank IPerlie CNo ratings yet
- Kursus IH ABO GROUPING v19082015 PDFDocument84 pagesKursus IH ABO GROUPING v19082015 PDFIlyasHasanNo ratings yet
- Blood BankingDocument7 pagesBlood BankingRoiland Atienza BaybayonNo ratings yet
- Tietz's Applied Laboratory MedicineFrom EverandTietz's Applied Laboratory MedicineMitchell G. ScottRating: 3 out of 5 stars3/5 (1)
- Special tests:) ١) ﺕﺎﻧﻮﺑﺮﻜﻴﺒﻟﺍ (Bicarbonate (Document4 pagesSpecial tests:) ١) ﺕﺎﻧﻮﺑﺮﻜﻴﺒﻟﺍ (Bicarbonate (hamaadaNo ratings yet
- Nilai University College Diploma in Medical Laboratory Technology MPAD 1221 Practical 5Document2 pagesNilai University College Diploma in Medical Laboratory Technology MPAD 1221 Practical 5hamaadaNo ratings yet
- ABO Grouping ProcedureDocument2 pagesABO Grouping ProcedurehamaadaNo ratings yet
- How To Use A BalanceDocument1 pageHow To Use A BalancehamaadaNo ratings yet
- Chitungwiza Central Hospital Laboratory DepartmentDocument2 pagesChitungwiza Central Hospital Laboratory DepartmenthamaadaNo ratings yet
- ABO Subgroups and Bombay GroupDocument15 pagesABO Subgroups and Bombay GrouphamaadaNo ratings yet
- ABO Forward TestingDocument2 pagesABO Forward TestinghamaadaNo ratings yet
- Cross-Matching: To Meet Wikipedia'sDocument5 pagesCross-Matching: To Meet Wikipedia'shamaadaNo ratings yet
- ABO Grouping ProcedureDocument2 pagesABO Grouping ProcedurehamaadaNo ratings yet
- Present VidasDocument24 pagesPresent Vidashamaada100% (1)
- Antibody IdentificationDocument27 pagesAntibody Identificationhamaada100% (2)
- 11-16 PaginaDocument40 pages11-16 Paginaclaudia ballester martinNo ratings yet
- Health Assessment: by Dr. Hala YehiaDocument115 pagesHealth Assessment: by Dr. Hala YehiaRazaCreciaLastrillaMenesesNo ratings yet
- 5 Living Things in Their Environment - 6 - People and Planet - QueDocument9 pages5 Living Things in Their Environment - 6 - People and Planet - Querashmi_harry100% (1)
- Biology - Local Heritage ThemesDocument5 pagesBiology - Local Heritage ThemesJerrycoNo ratings yet
- D D 5E Bestiary Journey Into The Realms PDFDocument7 pagesD D 5E Bestiary Journey Into The Realms PDFConnor GreenNo ratings yet
- Topic 4 Bio Peer Buddies AnsDocument3 pagesTopic 4 Bio Peer Buddies Ansamirahteaching95No ratings yet
- Manok Mabuhay (FINAL PAIR CASE)Document12 pagesManok Mabuhay (FINAL PAIR CASE)Eldon CalambaNo ratings yet
- MycologyDocument72 pagesMycologyDesa Refuerzo100% (1)
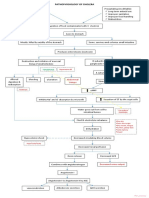
- Pathophysiology of Cholera PDFDocument1 pagePathophysiology of Cholera PDFRameshKrishnanNo ratings yet
- Bab Ii Tinjauan Teori: Benigna Prostatic Hyperplasia Adalah Pembesaran Jinak Kelenjar ProstatDocument27 pagesBab Ii Tinjauan Teori: Benigna Prostatic Hyperplasia Adalah Pembesaran Jinak Kelenjar Prostatdedi kurniawanNo ratings yet
- A Rough Guide To Drosophila Mating SchemesDocument39 pagesA Rough Guide To Drosophila Mating SchemesKirubes WaranNo ratings yet
- Anatomy of The Horse PDFDocument80 pagesAnatomy of The Horse PDFzemidahsalazarNo ratings yet
- Ujian Selaras 2 BI Paper 1Document9 pagesUjian Selaras 2 BI Paper 1Farah Anis IsmailNo ratings yet
- Evs Class 4 MDDocument3 pagesEvs Class 4 MDRohan DeopaNo ratings yet
- (The Natural History of The Crustacea) Les Watling, Martin Thiel (Eds.) - Functional Morphology and Diversity. 1-Oxford University Press (2013)Document515 pages(The Natural History of The Crustacea) Les Watling, Martin Thiel (Eds.) - Functional Morphology and Diversity. 1-Oxford University Press (2013)Yamaly Barragán MarínNo ratings yet
- Cell As A Unit of LifeDocument18 pagesCell As A Unit of LifeMohamad Abdul WahabNo ratings yet
- Teddy BearsDocument4 pagesTeddy BearsanaNo ratings yet
- Six Stages Four Levels San Jiao: ACR Class 5Document43 pagesSix Stages Four Levels San Jiao: ACR Class 5anon_70777627No ratings yet
- MenuDocument2 pagesMenuAlex ShparberNo ratings yet
- Coin 2023Document3 pagesCoin 2023samco.hienlvNo ratings yet
- A Detailed Lesson Plan in English 3Document10 pagesA Detailed Lesson Plan in English 3Mary Cres Deguma OtazaNo ratings yet
- BX Essentials - Cleric and Magic-User SpellsDocument37 pagesBX Essentials - Cleric and Magic-User SpellsArda Emirgeloğlu100% (2)
- GERUNDIODocument3 pagesGERUNDIOAntonio Javier Estaca AlarcónNo ratings yet
- DLL - English 4 - Q2 - W1Document5 pagesDLL - English 4 - Q2 - W1Allyza Fae DavidNo ratings yet
- BIP39 WordlistDocument1 pageBIP39 Wordlistcabal2979No ratings yet
- S1 1407010079 2018 JurnalDocument18 pagesS1 1407010079 2018 JurnalDaily Alman&momNo ratings yet