54 Shivraj Etal
54 Shivraj Etal
Download as pdf or txt
1058
Shivraj et al., Int J Med Res Health Sci. 2014;3(4):1058-1060
International Journal of Medical Research
&
Health Sciences
www.ijmrhs.com Volume 3 Issue 4 Coden: IJMRHS Copyright @2014 ISSN: 2319-5886
Received: 9
th
Aug 2014 Revised: 10
th
Sep 2014 Accepted: 18
th
Sep 2014
Case report
NEW INSIGHTS IN TO SYSTEMIC AMYLOIDOSIS: PRIMARY AMYLOIDOSIS ASSOCIATED
WITH TUBERCULAR LYMPHADENITIS
*Shivraj Meena
1
, Nirmal Ghati
2
, Rita Sood
3
, Naval Kishore Vikram
4
1
Senior Resident,
2
Junior Resident,
3
Professor,
4
Additional Professor, Department of Medicine, All India
Institute of Medical Sciences, New Delhi, India
*Corresponding author email: shivraj.aiims@gmail.com
ABSTRACT
Tuberculosis is generally followed by secondary amyloidosis. The association of primary systemic amyloidosis
with tuberculosis is very rare. There is only one case thus far reported in literature. We report such a rare case of
primary amyloidosis with tuberculous lymphadenopathy. A 45 year old woman presented at the medicine
department of all India institute of medical sciences , New Delhi with on & off erythematous rashes over both
eyes for 1 year; low grade fever, fatigue and significant weight loss for 4 months, dysphagia for solid food since 1
month. Main finding on examination were pallor, macroglossia, bilateral periorbital erythematous rashes (racoon
eyes), hepatomegaly & cardiomegaly. She had raised serum alkaline phosphatase level. Chest x-ray revealed
cardiomegaly. USG abdomen revealed multiple retroperitoneal mesenteric lymph nodes and hepatomegaly. USG
guided FNAC from mesenteric lymph node showed acid fast bacillus. Histological examination of liver biopsy
showed amyloid deposition on congo red stain. Patient was treated with DOTS category I ATT with Bortezomib
and Dexamethasone based weekly chemotherapy.
Keywords: Amyloidosis, Tubercular lymphdenopathy, Bortezomib
INTRODUCTION
The term amyloid was introduced in 1854 by the
German physician scientist Rudolph Virchow
(reviewed by Cohen, 1986).
1
Rudolf Virchow first
described amyloidosis as an extracellular deposition
of carbohydrate. What we know now is that there is
an extracellular deposition of proteinaceous material
which, when stained with Congo red gives apple
green birefringence under polarized light. In 1838,
Mathias Schleiden, a German botanist, coined the
term amyloid for the amylaceous constituents of
plants. In 1854, Rudolf Virchow adopted the term to
describe abnormal extra-cellular material that he
encountered in the liver during autopsy.
2
Divry and
associates
3
recognized that the amyloid deposits
showed apple-green birefringence when specimens
stained with Congo red were viewed under polarized
light. This observation remains the sine qua non of
the diagnosis of amyloidosis. We report a case of
uncommon association of primary AL amyloidosis
with a common disease.
CASE REPORT
A 45 year old woman presented with on & off
erythematous rashes over both eyes for 1 year; low
grade fever, fatigue and significant weight loss for 4
months, dysphagia for solid food since 1 month;
intermittent spasmodic pain at umbilical region since
20days. Her BP was 100/70 mm/Hg, PR: 102/ min,
RR:22/ min. She had pallor, macroglossia (figure1),
petechial rashes over right arm & bilateral periorbital
erythematous rashes (racoon eyes). On abdomen,
DOI: 10.5958/2319-5886.2014.00054.x
1059
Shivraj et al., Int J Med Res Health Sci. 2014;3(4):1058-1060
tenderness at right hypochondrium and enlarged firm
tender liver (24 cm) were present. CVS examination
revealed cardiomegaly only.
Fig 1: Showed macroglossia
Blood test showed Hb: 11.4g/dl, WBC: 14300/cu
mm, Platelet: 561000/ul, ESR: 05mm/hr. She had
isolated raised ALP: 840 IU/L) level. Urine routine
microscopy and 24 hr. urinary protein were normal.
Chest x-ray revealed cardiomegaly. Her ECG
revealed low voltage QRS complex in the limb leads
with poor progression of R wave in precordial leads.
As a suspected case of infection - HIV, hepatitis viral
markers, blood & urine gram stain culture done were
negative. Though toxic granules containing
neutrophils were present, no atypical malignant cells
in the blood. Lactate dehydrogenase level was
normal. Serum & urine protein electrophoresis
showed no M band, but elevated lambda light chain
level (=152. 53 mg/L) in serum free light chain
assay. kappa & lambda light chain ratio was low
(k:=0.06). Total protein & albumin globulin ratio
were normal.
USG abdomen revealed multiple retroperitoneal
mesenteric lymph nodes, hepatomegaly, mild ascites
and bilateral mild pleural effusion. Contrast enhanced
computed tomography (CECT) of chest and abdomen
confirmed the USG finding. USG guided Fine needle
Aspiration Cytology (FNAC) from mesenteric lymph
node showed Acid Fast Bacilli (AFB). Bone marrow
biopsy showed 7% mature plasma cells, but it was
negative for lymphoma deposits or amyloids.
Abdominal fat pad biopsy was equivocal for
amyloidosis. Subsequently liver biopsy was done and
histopathologicaly revealed amyloid deposition
(figure II). Immunohistochemistry of liver biopsy
showed predominant lambda light chain deposition
around blood vessels in the background of
nonspecific lambda and kappa light chain deposition
in the sinusoids.
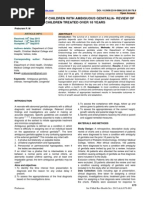
Fig 2: A Section of the liver stained with congo red
reveals pink-red deposits of amyloid (arrow) along
with sinusoids. (40x).
As the patient had progressive dysphagia, barium
swallow was showed sluggish peristalsis with tertiary
contraction in thoracic oesophagus but subsequent
upper G.I. endoscopy was normal. Autonomic
function tests revealed severe dysfunction, but the
nerve conduction test was normal. Echocardiography
showed bi-ventricular hypertrophy, bi-atrial
enlargement, thickened IVS and posterior wall,
granular sparkling of myocardium, severe left
ventricular dysfunction (EF 27%) & mild pericardial
effusion. Subsequent Holters study and BNP level
were normal.
Based on the above, a final diagnosis of primary
Amyloid Light-chain (AL) amyloidosis with
abdominal Koch was made. For tuberculosis,
category I anti tubercular treatment (ATT) and for
amyloidosis, Bortezomib and Dexamethasone based
weekly chemotherapy started. Though her symptoms
improved temporarily in the form of decreased
dizziness, fatigue, but after the third chemotherapy,
she developed decompensated chronic heart failure
(CHF) followed by diarrhoea. Appropriate treatment
started & Bortezomib based chemotherapy withheld
in the fear of drug induced diarrhoea. Later she
started having direct hyperbilirubinemia with
leucocytosis. ATT modified & broad spectrum
antibiotics started as all the investigations to localize
the infection were negative. Because of deranged
LFT, Bortezomib chemotherapy stopped and
Cyclophosphamide & Dexamethasone based weekly
chemotherapy started. But the patients condition
deteriorated rapidly and she died of septic shock with
aspiration pneumonia after 4 weeks.
1060
Shivraj et al., Int J Med Res Health Sci. 2014;3(4):1058-1060
DISCUSSION
Amyloidosis is a heterogeneous group of diseases
associated with the common pathological process of
extracellular protein deposition in various organs,
leading to organ dysfunction and death.
Inspite of the fact that hepatic involvement in
systemic amyloidosis is common histologically
occurring in 60-100% of liver specimens
4
clinically
apparent liver disease is infrequent. The patient had
markedly elevated serum alkaline phosphatase which
suggests an early phase of intrahepatic cholestasis.
Jaundice is usually a terminal feature and most
probably would have appeared if the patient had lived
long enough. Intrahepatic cholestasis secondary to
amyloidosis has been reported by several other
workers.
5,6
Other parameters of liver function which
reflect the integrity of the hepatic parenchymal cells,
such as bilirubin level, serum albumin and
prothrombin time were normal because hepatic
amyloidosis is primarily an infiltrative disorder.
Tuberculosis is generally followed by secondary
amyloidosis. The association of primary systemic
amyloidosis with tuberculosis is very rare. Only one
case thus far reported in literature.
7
Diagnosis of
tuberculosis in presence of systemic amyloidosis can
be challenging as Amyloid material in a lymph node
can masquerade as caseous necrosis in cytology.
8
Our
patient had AFB in the abdominal lymph nodes which
regressed completely with ATT. The present case
outlines the challenges in management of atypical
cases where liver involvement with amyloid and use
of potentially hepatotoxic drugs was required for the
treatment of the patient.
There was no identifiable chronic inflammatory,
infective or neoplastic disorder to account for
amyloid deposition. Serum protein electrophoresis
did not show abnormal band. There was no bence-
jones protein in urine and bone marrow examination,
did not show expansion of plasma cell. This suggests
that the amyloidosis is most likely to be primary, but
unrelated to any overt immunocyte dyscrasia.
Our patient had primary amyloidosis with Liver,
Cardiac, ANS and GIT involvement with abdominal
tuberculous lymphadenopathy. Bortezomib with
dexamethasone is a proven therapy for primary
amyloidosis.
9
Our patient was started on this
treatment. Since she developed side effects, therapy
was changed to cyclophosphamide. But she
succumbed to her disease.
CONCLUSION
We conclude that tuberculosis is generally followed
by secondary amyloidosis. The association of primary
systemic amyloidosis with tuberculosis is very rare,
but in this case we can also think that primary
systemic amyloidosis can be associated with
tuberculosis.
ACKNOWLEDGMENT
This work was done in the department of medicine at
AIIMS, Hospital without any additional financial
support. Authors thanks to all participants in this
study. They are also grateful to Dr A B Dey for their
advice to patient care and management.
Conflict of interest: The authors declare no conflict
of interest.
REFRENCES
1 Jean DS, Alan SC. History of the Amyloid Fibril.
Journal of Structural Biology. 2000;130:8898.
2 Virchow VR. Ueber einem Gehirn and
Rueckenmark des Menschen auf gefundene
Substanz mit chemischen reaction der Cellulose.
Virchows Arh Pathol Anat.1854;6:135-8.
3 Divry P, Florkin M. Sur les prorietes optiques de
lamyloide. CR Seances Soc Biol.1927;97:1808-
10.
4 Gertz MA, Kyle RA. hepatic amyloidosis clinical
appraisal in 77 patients. Hepatology.
1997;25:118-21
5 Mc Donald P, Usborne C, Playfer JRA. Case of
intrahepatic choestasis due to amyloidosis. Int. J.
Clin. Pract. 1988;52:201-02
6 Gornka MK, Bhasin DK, Vasisth RK,Dhawan S.
Hepatic amyloidosis presenting with severe
intraheptic cholestasis. J. Clin Gastroenterol.
1996;23:134-36
7 Fekih L, Boussoffara L, Fenniche S, Hassene H.
Enigmatic evolution of an association of
pulmonary tuberculosis and amyloidosis. Rev
Mal Respir. 2011;28(5):691-5
8 Sharma N, Sharma S, Bindra R. Plasmacytoma
with amyloidosis masquerding as tuberculosis on
cytology. J Cytol. 2009;26:161-3
9 Kastritis E, Anagnostopoulos A.Treatment of
light chain (AL) amyloidosis with the
combination of bortezomib and dexamethasone.
Haematologica. 2007;92(10):1351-58
You might also like
- Archer USMLE Step 3 Question BankDocument116 pagesArcher USMLE Step 3 Question Bankrolpf garri50% (4)
- Autoimmune Hepatitis - SLE Overlap SyndromeDocument2 pagesAutoimmune Hepatitis - SLE Overlap SyndromeMulyono Aba AthiyaNo ratings yet
- Trousseau's Syndrome in CholangiocarcinomaDocument7 pagesTrousseau's Syndrome in CholangiocarcinomaAnna MariaNo ratings yet
- Case Report: Tuberculosis Liver Abscess in Alcoholism Male PatientDocument4 pagesCase Report: Tuberculosis Liver Abscess in Alcoholism Male PatientWidya Prawirani SiahaanNo ratings yet
- Pancytopenia Secondary To Bacterial SepsisDocument16 pagesPancytopenia Secondary To Bacterial Sepsisiamralph89No ratings yet
- Al12 1 JuvenileDocument24 pagesAl12 1 JuvenileDiego Alberto Hernández CatalánNo ratings yet
- Systemic Sarcoidosis Mimicking Malignant Metastatic DiseaseDocument5 pagesSystemic Sarcoidosis Mimicking Malignant Metastatic Diseasee.elshikh2008No ratings yet
- Prevalence of Anaemia in Decompensated Chronic Liver DiseaseDocument5 pagesPrevalence of Anaemia in Decompensated Chronic Liver DiseaseElang SudewaNo ratings yet
- Pleural Effusion in A Patient With End-Stage Renal Disease - PMCDocument5 pagesPleural Effusion in A Patient With End-Stage Renal Disease - PMCCasemix rsudwaledNo ratings yet
- 2014 Kabir Et Al. - Chronic Eosinophilic Leukaemia Presenting With A CDocument4 pages2014 Kabir Et Al. - Chronic Eosinophilic Leukaemia Presenting With A CPratyay HasanNo ratings yet
- 1 PDFDocument5 pages1 PDFalejandrovesgaNo ratings yet
- Rounds: GrandDocument7 pagesRounds: GrandHưng Nguyễn KiềuNo ratings yet
- Caso QX 1Document4 pagesCaso QX 1smendozabrNo ratings yet
- Efusi Pleural in MassDocument4 pagesEfusi Pleural in MassRofi IrmanNo ratings yet
- 8156 29309 1 PBDocument5 pages8156 29309 1 PBEden LacsonNo ratings yet
- Tyro CR Saudi ArabiaDocument4 pagesTyro CR Saudi ArabiaMelanie Pad-ayNo ratings yet
- 10clinical VignettespdfDocument71 pages10clinical VignettespdfKerin Ardy100% (1)
- Gi 4Document3 pagesGi 4Syifa' FauziyahNo ratings yet
- Crim Em2013-948071Document2 pagesCrim Em2013-948071m.fahimsharifiNo ratings yet
- Leptospirosis CasosDocument2 pagesLeptospirosis CasosfelipeNo ratings yet
- A Case of Lupus Pneumonitis Mimicking As Infective PneumoniaDocument4 pagesA Case of Lupus Pneumonitis Mimicking As Infective PneumoniaIOSR Journal of PharmacyNo ratings yet
- Systemic AmiloidosisDocument4 pagesSystemic AmiloidosisioannesturrisoricisNo ratings yet
- Whipple S DiseaseDocument12 pagesWhipple S DiseaseGrifanda HumairahNo ratings yet
- Acute Pancreatitis Case PresDocument29 pagesAcute Pancreatitis Case Preskristine keen buan100% (1)
- AIHADocument4 pagesAIHAKristine Mae AbrasaldoNo ratings yet
- Delay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportDocument5 pagesDelay in Diagnosis of Extra-Pulmonary Tuberculosis by Its Rare Manifestations: A Case ReportSneeze LouderNo ratings yet
- Falciparum Malaria Complicated With Acute Pancreatitis: A Report of Case SeriesDocument3 pagesFalciparum Malaria Complicated With Acute Pancreatitis: A Report of Case SeriesMuhammad Taufik AdhyatmaNo ratings yet
- Patient Case Presentation IIDocument7 pagesPatient Case Presentation IILangat IsaacNo ratings yet
- More Itching: Diagnosis and ReasoningDocument4 pagesMore Itching: Diagnosis and ReasoningSYED SHAZIYANo ratings yet
- Gastroentrology LastDocument48 pagesGastroentrology LastAbdallah K. RamadanNo ratings yet
- Acutepancreatitis Withanemphasis Oninfection: Lutz Schneider,, Markus W. Büchler,, Jens WernerDocument21 pagesAcutepancreatitis Withanemphasis Oninfection: Lutz Schneider,, Markus W. Büchler,, Jens WernerTapas Kumar SahooNo ratings yet
- Case Study For Colon CancerDocument2 pagesCase Study For Colon Cancerrhimineecat7150% (2)
- Budd-Chiari Syndrome: A Clinical ApproachDocument5 pagesBudd-Chiari Syndrome: A Clinical ApproachTrisNo ratings yet
- Liver Abscess DissertationDocument4 pagesLiver Abscess DissertationPayForAPaperAtlanta100% (2)
- Hepatology - November December 1985 - Rolfes - Acute fatty liver of pregnancy A clinicopathologic study of 35 casesDocument10 pagesHepatology - November December 1985 - Rolfes - Acute fatty liver of pregnancy A clinicopathologic study of 35 casesPrahladRao KulkarniNo ratings yet
- The Patient With Rhabdomyolysis: Have You Considered Quail Poisoning?Document2 pagesThe Patient With Rhabdomyolysis: Have You Considered Quail Poisoning?andriopaNo ratings yet
- Hepatology - 1983 - Viola - Exudative Ascites in The Course of Acute Type B HepatitisDocument3 pagesHepatology - 1983 - Viola - Exudative Ascites in The Course of Acute Type B HepatitisAudryaNo ratings yet
- BRCU23_Practice_Questions_Answer_Key_All_1-489 2Document296 pagesBRCU23_Practice_Questions_Answer_Key_All_1-489 2uzma.malikNo ratings yet
- Idiopathic HypoparathyroidismDocument7 pagesIdiopathic HypoparathyroidismChokri MAKTOUFNo ratings yet
- Awuku 1552016 BJMMR26166Document4 pagesAwuku 1552016 BJMMR26166Kush GuptaNo ratings yet
- Autoimmune Hepatitis - Primary Biliary Cirrhosis Overlap SyndromeDocument3 pagesAutoimmune Hepatitis - Primary Biliary Cirrhosis Overlap Syndromesusanto kusumaNo ratings yet
- Artigo8Document5 pagesArtigo8genetica2024leonelNo ratings yet
- Acute Pancreatitis With Normal Serum Lipase: A Case SeriesDocument4 pagesAcute Pancreatitis With Normal Serum Lipase: A Case SeriesSilvina VernaNo ratings yet
- Fped 07 00310Document6 pagesFped 07 00310Fariz HidayatNo ratings yet
- Diagnostic and Therapeutic Approach To Hypercalcemia A Minireview and Discussion of CasesDocument5 pagesDiagnostic and Therapeutic Approach To Hypercalcemia A Minireview and Discussion of CasesScivision PublishersNo ratings yet
- Fmge MCQDocument4 pagesFmge MCQgrreddy8364320No ratings yet
- Case Report and Literature Review On Good's Syndrome, A Form of Acquired Immunodeficiency Associated With ThymomasDocument7 pagesCase Report and Literature Review On Good's Syndrome, A Form of Acquired Immunodeficiency Associated With ThymomasMudassar SattarNo ratings yet
- Hypomagnesemia and Prolonged Hospital Stay: A Case Report and Literature ReviewDocument6 pagesHypomagnesemia and Prolonged Hospital Stay: A Case Report and Literature ReviewIJAR JOURNALNo ratings yet
- Jaundice As A Presentation of Thyrotoxic CrisisDocument3 pagesJaundice As A Presentation of Thyrotoxic CrisisRizki AmeliaNo ratings yet
- Whipple DiseaseDocument10 pagesWhipple DiseaseRania Medhat SleemNo ratings yet
- A Case of HypercalcemiaDocument7 pagesA Case of HypercalcemiaWitrisyah PutriNo ratings yet
- Hypokalemic Periodic Paralysis A Case ReportDocument2 pagesHypokalemic Periodic Paralysis A Case ReportEditor IJTSRDNo ratings yet
- Today's: Diseases of The AlimentaryDocument3 pagesToday's: Diseases of The AlimentaryArix BakaNo ratings yet
- ArchIntSurg Adult IntuDocument5 pagesArchIntSurg Adult IntusinghalbmNo ratings yet
- Evans Syndrome - A Study of Six Cases With Review of LiteratureDocument6 pagesEvans Syndrome - A Study of Six Cases With Review of Literaturedrrome01No ratings yet
- Patient With Familial Multiple Lipomatosis and ReviewDocument5 pagesPatient With Familial Multiple Lipomatosis and Reviewalinutza_childNo ratings yet
- Bazo Errante 2016 REVISED Ijtra1601084Document4 pagesBazo Errante 2016 REVISED Ijtra1601084luisalfredo_montesNo ratings yet
- Cirrhosis of LiverDocument6 pagesCirrhosis of LiverpakdejackNo ratings yet
- Alert Medical Series: USMLE Alert I, II, IIIFrom EverandAlert Medical Series: USMLE Alert I, II, IIIRating: 2 out of 5 stars2/5 (1)
- 48 MakrandDocument2 pages48 MakrandeditorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 3Document271 pagesIjmrhs Vol 3 Issue 3editorijmrhsNo ratings yet
- Ijmrhs Vol 4 Issue 4Document193 pagesIjmrhs Vol 4 Issue 4editorijmrhs0% (1)
- Ijmrhs Vol 4 Issue 3Document263 pagesIjmrhs Vol 4 Issue 3editorijmrhsNo ratings yet
- Ijmrhs Vol 4 Issue 2Document219 pagesIjmrhs Vol 4 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 4Document294 pagesIjmrhs Vol 3 Issue 4editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 1Document110 pagesIjmrhs Vol 2 Issue 1editorijmrhs100% (1)
- Ijmrhs Vol 2 Issue 2Document197 pagesIjmrhs Vol 2 Issue 2editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 3Document399 pagesIjmrhs Vol 2 Issue 3editorijmrhs100% (1)
- Ijmrhs Vol 3 Issue 1Document228 pagesIjmrhs Vol 3 Issue 1editorijmrhsNo ratings yet
- Ijmrhs Vol 2 Issue 4Document321 pagesIjmrhs Vol 2 Issue 4editorijmrhsNo ratings yet
- Ijmrhs Vol 3 Issue 2Document281 pagesIjmrhs Vol 3 Issue 2editorijmrhsNo ratings yet
- 47serban Turliuc EtalDocument4 pages47serban Turliuc EtaleditorijmrhsNo ratings yet
- Ijmrhs Vol 1 Issue 1Document257 pagesIjmrhs Vol 1 Issue 1editorijmrhsNo ratings yet
- 41anurag EtalDocument2 pages41anurag EtaleditorijmrhsNo ratings yet
- 45mohit EtalDocument4 pages45mohit EtaleditorijmrhsNo ratings yet
- Pernicious Anemia in Young: A Case Report With Review of LiteratureDocument5 pagesPernicious Anemia in Young: A Case Report With Review of LiteratureeditorijmrhsNo ratings yet
- Recurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoDocument2 pagesRecurrent Cornual Ectopic Pregnancy - A Case Report: Article InfoeditorijmrhsNo ratings yet
- Williams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdultDocument3 pagesWilliams-Campbell Syndrome-A Rare Entity of Congenital Bronchiectasis: A Case Report in AdulteditorijmrhsNo ratings yet
- 40vedant EtalDocument4 pages40vedant EtaleditorijmrhsNo ratings yet
- 38vaishnavi EtalDocument3 pages38vaishnavi EtaleditorijmrhsNo ratings yet
- 37poflee EtalDocument3 pages37poflee EtaleditorijmrhsNo ratings yet
- 35krishnasamy EtalDocument1 page35krishnasamy EtaleditorijmrhsNo ratings yet
- 31tushar EtalDocument4 pages31tushar EtaleditorijmrhsNo ratings yet
- 36rashmipal EtalDocument6 pages36rashmipal EtaleditorijmrhsNo ratings yet
- 34tupe EtalDocument5 pages34tupe EtaleditorijmrhsNo ratings yet
- 28nnadi EtalDocument4 pages28nnadi EtaleditorijmrhsNo ratings yet
- 33 Prabu RamDocument5 pages33 Prabu RameditorijmrhsNo ratings yet
- Unit 7, Cognition Reading Guide-1Document7 pagesUnit 7, Cognition Reading Guide-1Asian PersonNo ratings yet
- Sounds in PoetryDocument5 pagesSounds in Poetryapi-276005643No ratings yet
- Plasticity - End Sem QNDocument4 pagesPlasticity - End Sem QNVarun Teja VaddamaniNo ratings yet
- LA 100 Coagulation Analyzer User Manual 2Document17 pagesLA 100 Coagulation Analyzer User Manual 2john02 deanNo ratings yet
- Mado Kara Mieru (Through The Window I See) : Hattori Ransetsu (Author)Document1 pageMado Kara Mieru (Through The Window I See) : Hattori Ransetsu (Author)andyNo ratings yet
- LittleWorldofWhimsy Pumpkin Bear Amigurumi PatternDocument9 pagesLittleWorldofWhimsy Pumpkin Bear Amigurumi PatternPiggydo GamingNo ratings yet
- Chemical Composition of The EarthDocument58 pagesChemical Composition of The EarthPutik Nurul ArasyNo ratings yet
- Bill of Quantities: ExcavationDocument2 pagesBill of Quantities: ExcavationDasun IsharaNo ratings yet
- NSO Class 4 Paper 2018 Part 1Document3 pagesNSO Class 4 Paper 2018 Part 1Rajesh RNo ratings yet
- I WonderDocument13 pagesI WonderNoor HayatiNo ratings yet
- Recent Trends in OperationsDocument7 pagesRecent Trends in Operationsgag90No ratings yet
- Application Form Garudafood GroupDocument4 pagesApplication Form Garudafood GroupReinhard DavidNo ratings yet
- Notation (For Chapter 10) Foreword The Authors: VII Ix XDocument4 pagesNotation (For Chapter 10) Foreword The Authors: VII Ix XShabbir Lokhandwala0% (1)
- STE-Micro ProjectDocument15 pagesSTE-Micro ProjectJai MalharNo ratings yet
- Smiletrack: Similarity Learning For Occlusion-Aware Multiple Object TrackingDocument12 pagesSmiletrack: Similarity Learning For Occlusion-Aware Multiple Object TrackingneojasstariiiNo ratings yet
- Invitation To Respected M. Venkaiah NaiduDocument1 pageInvitation To Respected M. Venkaiah NaiduDaniel 0009No ratings yet
- Weber's LawDocument2 pagesWeber's LawSteven John EbreoNo ratings yet
- About WheelsDocument2 pagesAbout Wheelsgyro470No ratings yet
- Rinac Banana Ripening ChamberDocument4 pagesRinac Banana Ripening Chambermep sbcuNo ratings yet
- 2023 EQUIS Process ManualDocument66 pages2023 EQUIS Process Manualrichard.brunnquellNo ratings yet
- Why Study ReligionDocument2 pagesWhy Study ReligionNetworkNo ratings yet
- ENITV12D 01.01.algebra Part4Document45 pagesENITV12D 01.01.algebra Part4MARITHE ROJIANNE MERCADONo ratings yet
- Escort PDFDocument13 pagesEscort PDFKripashankar MauryaNo ratings yet
- 6-ICT Technician NOV 23Document4 pages6-ICT Technician NOV 23mickyraycon45No ratings yet
- Pink, 2015 - Engaging The Senses in Ethnographic PracticeDocument8 pagesPink, 2015 - Engaging The Senses in Ethnographic PracticeLMC UdMNo ratings yet
- Mist Collectors: Item Frequency ProcedureDocument2 pagesMist Collectors: Item Frequency ProcedureALI TAVAKOLINIANo ratings yet
- Antibiotics in Periodental TreatmentDocument29 pagesAntibiotics in Periodental TreatmentJana AliNo ratings yet
- (1976 Casagrande) Liquefaction and Cyclic Deformation of Sands - A Critical ReviewDocument55 pages(1976 Casagrande) Liquefaction and Cyclic Deformation of Sands - A Critical Reviewsanpaz75100% (4)
- MidTerm Test English 4Document2 pagesMidTerm Test English 4tlinh1768No ratings yet
- VLSM ExerciseDocument3 pagesVLSM ExerciseRon NecesitoNo ratings yet