Outpatient Resume
Outpatient Resume
Download as pdf or txt
You might also like
- Disability Support Pension Claim FormsDocument11 pagesDisability Support Pension Claim Formscurtisbrown89No ratings yet
- Raheel OSCE Notes January 2023Document453 pagesRaheel OSCE Notes January 2023KamleshKumar100% (2)
- Medical CertificateDocument2 pagesMedical Certificatelaxman28975% (4)
- Letter of Medical Necessity TemplateDocument2 pagesLetter of Medical Necessity TemplateEmily SchechterNo ratings yet
- Lemko Experiences As Recalled by Teodor DokliaDocument31 pagesLemko Experiences As Recalled by Teodor DokliaTheLemkoProjectNo ratings yet
- The Importance of PlayDocument6 pagesThe Importance of PlayMarcelo TorresNo ratings yet
- 22 Tips For Learning A Foreign LanguageDocument4 pages22 Tips For Learning A Foreign LanguageRadu RadionNo ratings yet
- Gendering Humanoid Robots: Robo-Sexism in JapanDocument36 pagesGendering Humanoid Robots: Robo-Sexism in JapanThePoliticalHat100% (1)
- Raul Moncayo Lalangue Sinthome Jouissance and Nomination A Reading Companion and Commentary On Lacans Seminar Xxiii On The SinthomeDocument1 pageRaul Moncayo Lalangue Sinthome Jouissance and Nomination A Reading Companion and Commentary On Lacans Seminar Xxiii On The SinthomeVa KhoNo ratings yet
- Medication Management FormDocument3 pagesMedication Management FormOlrac AgairdamNo ratings yet
- DD Intro For MsDocument54 pagesDD Intro For MsZuhaib AhmedNo ratings yet
- Unit 2bDocument3 pagesUnit 2bapi-242363297No ratings yet
- MH Case StudyDocument17 pagesMH Case StudyS. JacobsNo ratings yet
- Clinical Guideline Adjustment Disorders DescriptionDocument4 pagesClinical Guideline Adjustment Disorders DescriptionprabhaNo ratings yet
- palliative care and Pain managementDocument85 pagespalliative care and Pain managementaliabubakr20021229No ratings yet
- Health DeclarationDocument1 pageHealth DeclarationJayson VitaNo ratings yet
- NCPDocument18 pagesNCPChristian Karl B. LlanesNo ratings yet
- Physiotherapy BookDocument86 pagesPhysiotherapy BookAreeba HasnainNo ratings yet
- New Query LetterDocument13 pagesNew Query LettersyawalNo ratings yet
- Amerigroup Auth Form- April 2022Document2 pagesAmerigroup Auth Form- April 2022Dilip Kumar RNo ratings yet
- 12 11 22 ITC - Form - Support Services ReferralDocument7 pages12 11 22 ITC - Form - Support Services Referralrhu silagoNo ratings yet
- Health Assessment Record: State of Connecticut Department of EducationDocument3 pagesHealth Assessment Record: State of Connecticut Department of EducationVishwanath SinduvadiNo ratings yet
- MedicalCertificate (4)Document2 pagesMedicalCertificate (4)himanshushrivastava802No ratings yet
- Proposal For Psychology OPDocument6 pagesProposal For Psychology OPneerajgr2005No ratings yet
- Patient Information Prescriber Information: Male FemaleDocument2 pagesPatient Information Prescriber Information: Male Femaleroohan AdeelNo ratings yet
- Case History and Mental State Examination (1) GarimaDocument36 pagesCase History and Mental State Examination (1) GarimaAditi SainiNo ratings yet
- Your Health PlanDocument9 pagesYour Health PlanMaggie FornaroNo ratings yet
- Cognitive-Behavioral Therapy For Somatization Disorder: A Randomized Controlled TrialDocument7 pagesCognitive-Behavioral Therapy For Somatization Disorder: A Randomized Controlled TrialMuhammad Bayu WNo ratings yet
- Fit To Work Certificate DocxDocument3 pagesFit To Work Certificate DocxBlood ViernesNo ratings yet
- Danielle Doberman Geriatric Palliative CareDocument46 pagesDanielle Doberman Geriatric Palliative CareArsya Wina100% (1)
- SCHIZOPHRENIADocument20 pagesSCHIZOPHRENIALuzelle Joy A. DemingoyNo ratings yet
- Introduction To Psychiatry Practical Lesson N 1 Varianta NouaDocument35 pagesIntroduction To Psychiatry Practical Lesson N 1 Varianta NouaUlaim UsmanNo ratings yet
- KWESTIYONEYRDocument7 pagesKWESTIYONEYRKyle CortezNo ratings yet
- Connect Health QuestionnairesDocument1 pageConnect Health Questionnairesraj6912377No ratings yet
- PT As Patient Client ManagerDocument39 pagesPT As Patient Client Managerpihabo3594No ratings yet
- CGH Earth Ayurveda - PAF - EditableDocument6 pagesCGH Earth Ayurveda - PAF - EditableerosemottaNo ratings yet
- Periodic Health Exam Form UP Manila Students Rev May 31 2020Document2 pagesPeriodic Health Exam Form UP Manila Students Rev May 31 2020Piss DrunxNo ratings yet
- Example Healthcare PlanDocument6 pagesExample Healthcare Plansesaeedhaniyah.dNo ratings yet
- Dr Letter Template - NDIS ParticipantsDocument1 pageDr Letter Template - NDIS ParticipantssupportNo ratings yet
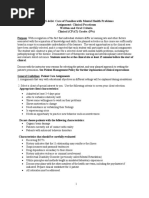
- NURS 4414: Care of Families With Mental Health Problems Assignment: Clinical Practicum Written and Oral Criteria Clinical (CPAT) Grade: (5%)Document13 pagesNURS 4414: Care of Families With Mental Health Problems Assignment: Clinical Practicum Written and Oral Criteria Clinical (CPAT) Grade: (5%)Lj GabayanNo ratings yet
- 3 PST - 2018Document16 pages3 PST - 2018yekunoNo ratings yet
- Differential Diagnosis and Clinical Decision MakingDocument26 pagesDifferential Diagnosis and Clinical Decision MakingbkdfiesefllNo ratings yet
- Attending Physicians Statement FormDocument3 pagesAttending Physicians Statement Formdennis gamisNo ratings yet
- Doctors Note Template 34Document2 pagesDoctors Note Template 34Christopher Gregory-DustinNo ratings yet
- Reading Test - 3 Clinical Depression Text ADocument17 pagesReading Test - 3 Clinical Depression Text AJisha JanardhanNo ratings yet
- ImtinanDocument4 pagesImtinandekaali20No ratings yet
- Gravida: Para: Ab:: Mark N/a If Not Applicable)Document11 pagesGravida: Para: Ab:: Mark N/a If Not Applicable)heahou8716No ratings yet
- Naturalpath Intake Form - ADULTDocument5 pagesNaturalpath Intake Form - ADULTcms_gcoles100% (1)
- Client Intake FormDocument3 pagesClient Intake FormR SalehNo ratings yet
- Asthma Nursing Care Plans - LippincottDocument45 pagesAsthma Nursing Care Plans - LippincottDyllanoNo ratings yet
- Patient PerspectivesDocument2 pagesPatient Perspectiveshydra89No ratings yet
- 1 History Taking (المرحله الثالثه (1) 2 - ltDocument34 pages1 History Taking (المرحله الثالثه (1) 2 - ltمحمد نزار غياث الدينNo ratings yet
- Reflexology: Grinberg MethodDocument2 pagesReflexology: Grinberg MethodHannah CheethamNo ratings yet
- Critical Thinking and Nursing ProcessDocument49 pagesCritical Thinking and Nursing Processjeorj100% (2)
- Case History and Mental State Examination Case HistoryDocument37 pagesCase History and Mental State Examination Case HistoryAditi SainiNo ratings yet
- Msii Pat 2Document22 pagesMsii Pat 2api-300946501No ratings yet
- OLDCARTS SOAP Note ReferenceDocument6 pagesOLDCARTS SOAP Note ReferenceMengqi LiNo ratings yet
- Medical Certificate of Fitness: To Be Filled by CandidateDocument2 pagesMedical Certificate of Fitness: To Be Filled by CandidatevenkatNo ratings yet
- CWHH Referral Form Wboxes v1Document1 pageCWHH Referral Form Wboxes v1carrie.e.hall03No ratings yet
- Hypertension Questionnaire-Applicant: Policy NumberDocument2 pagesHypertension Questionnaire-Applicant: Policy NumberMariane Tabor VelezNo ratings yet
- 1 NoncomplianceDocument4 pages1 Noncomplianceprincess_uy_2No ratings yet
- Draft Palliative Care Needs Assessment - A Guide For Health Care ProfessionalsDocument10 pagesDraft Palliative Care Needs Assessment - A Guide For Health Care ProfessionalsSenja TsamrotulNo ratings yet
- Medical Fitness CertificateDocument2 pagesMedical Fitness Certificatesen25428No ratings yet
- Physician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideFrom EverandPhysician Assistant PANCE & PANRE: a QuickStudy Laminated Reference GuideNo ratings yet
- Engineering Mechanics: Course Code: DME-205Document16 pagesEngineering Mechanics: Course Code: DME-205HaradipMahilaryNo ratings yet
- Career Guidance Program 2024 Activity GuidelinesDocument3 pagesCareer Guidance Program 2024 Activity GuidelinesIricel BuenoNo ratings yet
- Globalization, Evolution and Emergence of Direct-To-Consumer Advertising: Are Emerging Markets The Next Pharmaceutical Marketing Frontier?Document1 pageGlobalization, Evolution and Emergence of Direct-To-Consumer Advertising: Are Emerging Markets The Next Pharmaceutical Marketing Frontier?Dede PriyantiNo ratings yet
- Journal of Power Sources: Anja Lund, Yuan Tian, Sozan Darabi, Christian MüllerDocument11 pagesJournal of Power Sources: Anja Lund, Yuan Tian, Sozan Darabi, Christian Müllerlion walrusNo ratings yet
- 3) Sop For Cleaning & Sanitation of Microbiolgy LaboratoryDocument4 pages3) Sop For Cleaning & Sanitation of Microbiolgy LaboratoryEnam HaqNo ratings yet
- William Valve Catalogue Ball ValveDocument24 pagesWilliam Valve Catalogue Ball ValveVinayNo ratings yet
- Dir Lower: Application Form Original Challan ReceiptDocument3 pagesDir Lower: Application Form Original Challan ReceiptwaheedNo ratings yet
- Women PeacekeepersDocument3 pagesWomen PeacekeepersNabeel A K JadoonNo ratings yet
- Taxonomy: Marjoe Visoc John Ritz Tampos Marvy RevillaDocument5 pagesTaxonomy: Marjoe Visoc John Ritz Tampos Marvy RevillaSheila DominguezNo ratings yet
- The Tuition and Miscellaneous Fee Charging StandardsDocument1 pageThe Tuition and Miscellaneous Fee Charging StandardsDipta Divakara Pius PurwadariaNo ratings yet
- DCF Vs Multiple PDFDocument4 pagesDCF Vs Multiple PDFveda20100% (1)
- China City PPT 2Document29 pagesChina City PPT 2Tayrel Rafael Rodríguez MeléndezNo ratings yet
- Assingment 1 - Case StudyDocument23 pagesAssingment 1 - Case StudyMUHAMMAD NASRUN NAJMI LEHASROMNo ratings yet
- Activity 4. Identification of Different Organic CompoundsDocument6 pagesActivity 4. Identification of Different Organic CompoundstuanijoshuaNo ratings yet
- Engineering Manual Spate Irrigation Small-1Document112 pagesEngineering Manual Spate Irrigation Small-1Eba AjemaNo ratings yet
- Info SectionDocument68 pagesInfo Sectionnewcomersguide100% (1)
- 5 An Introduction To Popular Literature 2Document12 pages5 An Introduction To Popular Literature 2Renz MostazaNo ratings yet
- Shelf Life of ChemicalsDocument6 pagesShelf Life of ChemicalsbrokentoeNo ratings yet
- System Cheat Sheet - GADocument2 pagesSystem Cheat Sheet - GAhadene.randolphNo ratings yet
- Literature Review On 3d PrintingDocument6 pagesLiterature Review On 3d Printingguzxwacnd100% (1)
- Erco Outdoor Lighting Facades enDocument6 pagesErco Outdoor Lighting Facades enAnirban1987No ratings yet
- Ethics, Legal Liability, and Client Acceptance: Third Canadian EditionDocument49 pagesEthics, Legal Liability, and Client Acceptance: Third Canadian EditionRajNo ratings yet
- Outsiders Digital Journal 2Document7 pagesOutsiders Digital Journal 2api-206371564No ratings yet
- RonNielsen NuclearReactionsDocument471 pagesRonNielsen NuclearReactionsr_nielsenNo ratings yet
- Bise Lahore Examination Result Status SheetDocument1 pageBise Lahore Examination Result Status SheetAfzaal AhmadNo ratings yet
- Cisco SD-Access - Integrating With Your Existing Network - Vedran HafnerDocument91 pagesCisco SD-Access - Integrating With Your Existing Network - Vedran HafnerMaheshBangera100% (1)