Epistaxis
Epistaxis
Download as docx, pdf, or txt
You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Epistaxis: Neil Alexander Krulewitz,, Megan Leigh FixDocument11 pagesEpistaxis: Neil Alexander Krulewitz,, Megan Leigh FixSantos Pardo GómezNo ratings yet
- Epistaxis: "Bleeding From Inside The Nose"Document12 pagesEpistaxis: "Bleeding From Inside The Nose"Farrukh Mehmood100% (1)
- Jurnal EpistaksisDocument8 pagesJurnal Epistaksiskhusna wahyuniNo ratings yet
- Mona Notes - NoseDocument11 pagesMona Notes - NoseBinta BaptisteNo ratings yet
- Updates On The Management of Epistaxis: ReviewDocument11 pagesUpdates On The Management of Epistaxis: ReviewBagusPranataNo ratings yet
- Epistaxis Pic 2014 01 GDocument70 pagesEpistaxis Pic 2014 01 GJeanne d'Arc DyanchanaNo ratings yet
- Clinical Manifestation of EpistaxisDocument2 pagesClinical Manifestation of Epistaxisjaish8904100% (1)
- 32 EpistaxisDocument14 pages32 EpistaxisFadill SanjaniNo ratings yet
- Epistaxis: A Common Problem: Adil Fatakia, MD, Ryan Winters, MD, Ronald G. Amedee, MDDocument3 pagesEpistaxis: A Common Problem: Adil Fatakia, MD, Ryan Winters, MD, Ronald G. Amedee, MDaprilfitriaNo ratings yet
- Epistaxis 2-1-6Document6 pagesEpistaxis 2-1-6Nurul aina MardhiyahNo ratings yet
- Anterior Recurrent Epistaxis From Kiesselbach'S AreaDocument4 pagesAnterior Recurrent Epistaxis From Kiesselbach'S Arealukas_doniNo ratings yet
- Epistaxis 12Document29 pagesEpistaxis 12Aryan BhatNo ratings yet
- Nose BleedsDocument15 pagesNose BleedsMohaaz AbdiNo ratings yet
- Epistaxis: S. H. MDDocument14 pagesEpistaxis: S. H. MDLilia ScutelnicNo ratings yet
- Epistaxis: Çağatay Oysu, M.D. Professor of OtolaryngologyDocument35 pagesEpistaxis: Çağatay Oysu, M.D. Professor of Otolaryngologymounes dhairyNo ratings yet
- Tan1999 PDFDocument14 pagesTan1999 PDFIntan Nur HijrinaNo ratings yet
- EpistaxisDocument30 pagesEpistaxisAhlam DreamsNo ratings yet
- Lo No 1 Epistaksis - Id.enDocument17 pagesLo No 1 Epistaksis - Id.enRezi OktavianiNo ratings yet
- Assaignment Title: Causes, Work Up & Management of Epistaxis Discipline: MBBSDocument11 pagesAssaignment Title: Causes, Work Up & Management of Epistaxis Discipline: MBBSJahanzaib SaeedNo ratings yet
- Anterior Epistaxis PDFDocument9 pagesAnterior Epistaxis PDFTiara Audina DarmawanNo ratings yet
- Epistaxis: Dr. Wachuka G. Thuku Tutorial Fellow-ENT RegistrarDocument32 pagesEpistaxis: Dr. Wachuka G. Thuku Tutorial Fellow-ENT RegistrarAlexNo ratings yet
- EPISTAXIS LectureDocument30 pagesEPISTAXIS LectureDhienWhieNo ratings yet
- EPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Document34 pagesEPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Julliza Joy PandiNo ratings yet
- Approach To The Adult With Epistaxis - UpToDateDocument29 pagesApproach To The Adult With Epistaxis - UpToDateAntonella Angulo CruzadoNo ratings yet
- EpistaxisDocument39 pagesEpistaxisAbubakar JallohNo ratings yet
- EPISTAXISDocument38 pagesEPISTAXISVandit JainNo ratings yet
- Postgrad Med J 2005 Pope 309 14Document9 pagesPostgrad Med J 2005 Pope 309 14Steven LiaNo ratings yet
- Nasal Polyp MedscapeDocument30 pagesNasal Polyp MedscapeMonissa ArrianiNo ratings yet
- EpistaksisDocument3 pagesEpistaksisyudishannaNo ratings yet
- Epistaxis: Neil Alexander Krulewitz,, Megan Leigh FixDocument3 pagesEpistaxis: Neil Alexander Krulewitz,, Megan Leigh FixNurul aina MardhiyahNo ratings yet
- Systemic Infection Is An Infection That Is in The BloodstreamDocument4 pagesSystemic Infection Is An Infection That Is in The BloodstreamninaNo ratings yet
- Special Sense1Document16 pagesSpecial Sense1ziyadkhatta1No ratings yet
- Epistaxis: Ms. Shital BhutkarDocument37 pagesEpistaxis: Ms. Shital BhutkarSuhas Ingale0% (1)
- Epistaxis 130329165831 Phpapp02Document26 pagesEpistaxis 130329165831 Phpapp02MAMA LALANo ratings yet
- Definition: Anatomy:: Little's AreaDocument5 pagesDefinition: Anatomy:: Little's AreaFransisca YustikaNo ratings yet
- Atrial Septal Defect: Go ToDocument10 pagesAtrial Septal Defect: Go ToanisNo ratings yet
- 381 - Treatment of Dural Arteriovenous Malformations and FistulaeDocument13 pages381 - Treatment of Dural Arteriovenous Malformations and FistulaeИван ДимитровNo ratings yet
- Epistaxis: Anatomical TypesDocument8 pagesEpistaxis: Anatomical TypesMohamad AtefNo ratings yet
- Capp&Dwe TomeldenfinalDocument74 pagesCapp&Dwe Tomeldenfinaltomeldenalyssa13No ratings yet
- Untitled 1Document17 pagesUntitled 1Jennifer Catahimican Dela RosaNo ratings yet
- Neuroradiologi EpistaksisDocument12 pagesNeuroradiologi EpistaksisAndikaSetionoNo ratings yet
- 6 EpistaxisDocument19 pages6 EpistaxissuciNo ratings yet
- Updates On The Management of EpistaxisDocument9 pagesUpdates On The Management of EpistaxisIlham NoeryosanNo ratings yet
- Nose and Paranasal Sinuses According To New Reference 2Document121 pagesNose and Paranasal Sinuses According To New Reference 2Victor EnachiNo ratings yet
- Brain Abscess and SepsisDocument32 pagesBrain Abscess and SepsisSanjeet SahNo ratings yet
- 01 EpistaxisDocument23 pages01 Epistaxiswissam salimNo ratings yet
- Bilateral Hemotympanum As A Result of Spontaneous Epistaxis: Casereport Open AccessDocument3 pagesBilateral Hemotympanum As A Result of Spontaneous Epistaxis: Casereport Open AccessYuna WidjajaNo ratings yet
- Congenital Heart Defect-VsdDocument53 pagesCongenital Heart Defect-VsdAuni Akif AleesaNo ratings yet
- Personal DataDocument2 pagesPersonal DataSheenaGuinoCullaNo ratings yet
- Epistaxis 2019Document20 pagesEpistaxis 2019dr MohammedNo ratings yet
- Epistaxis and TumorDocument20 pagesEpistaxis and TumorTri Ayu WdNo ratings yet
- Tetralogy of FallotDocument7 pagesTetralogy of FallotAshok Kumar JangirNo ratings yet
- An Update On EpistaxisDocument5 pagesAn Update On EpistaxisDartalina SidaurukNo ratings yet
- 1) Dental Management in Children With Heart DiseaseDocument13 pages1) Dental Management in Children With Heart DiseaseAJPEDO LIFENo ratings yet
- Approach To The Adult With EpistaxisDocument18 pagesApproach To The Adult With EpistaxisTP RMad100% (1)
- Cerebral Venous Sinus ThrombosisDocument34 pagesCerebral Venous Sinus ThrombosisNeurologia homicNo ratings yet
- Cavernous Sinus Thrombosis: Clinical FeaturesDocument4 pagesCavernous Sinus Thrombosis: Clinical FeaturesStefanus ChristianNo ratings yet
- JR THTDocument4 pagesJR THTbintang dwiNo ratings yet
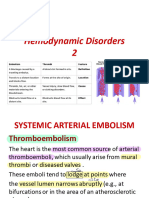
- Lec 11 hemodynamic 2Document23 pagesLec 11 hemodynamic 21stfallujaNo ratings yet
- Some Ideas To Improve Health With VastuDocument46 pagesSome Ideas To Improve Health With VastuKs SenthilKumarNo ratings yet
- Blood Pressure 911Document7 pagesBlood Pressure 911Judith J. LaneNo ratings yet
- IPHO AR For FY 2023Document38 pagesIPHO AR For FY 2023EVANGELISTA REYMUND V.No ratings yet
- Telemetry Recognition WorkbookDocument29 pagesTelemetry Recognition WorkbookQueenNo ratings yet
- PreeclampsiaDocument14 pagesPreeclampsiaHenny NovitasariNo ratings yet
- CRS Report For Congress: Life Expectancy in The United StatesDocument33 pagesCRS Report For Congress: Life Expectancy in The United StatesAdrian Saporta100% (1)
- HypertensionDocument11 pagesHypertensionArmina LagumbayNo ratings yet
- Cardio History TakingDocument4 pagesCardio History Takingwaleed sonbolNo ratings yet
- Hypertension in Dialysis PatientsDocument16 pagesHypertension in Dialysis PatientsSaad Anwar GujjarNo ratings yet
- Competency Based Learning Module: Hilot Wellness Massage Ncii Issued By: Page 1 of 61Document24 pagesCompetency Based Learning Module: Hilot Wellness Massage Ncii Issued By: Page 1 of 61Menchue AyudivNo ratings yet
- Product Includes:: Model BP765 Instruction ManualDocument40 pagesProduct Includes:: Model BP765 Instruction ManualMadhuritha RajapakseNo ratings yet
- Lippincot Price List 2023Document8 pagesLippincot Price List 2023vmags822No ratings yet
- Administering Metoprolol IV Push 1Document22 pagesAdministering Metoprolol IV Push 1api-357388170No ratings yet
- CHN Idb QuestionnaireDocument19 pagesCHN Idb QuestionnaireVincent Del ArthNo ratings yet
- Qi 42 PDFDocument38 pagesQi 42 PDFnambaccuc100% (2)
- Maternal and ChildDocument204 pagesMaternal and Childmj Canilang100% (1)
- Hipertensi Pregnancy PICODocument31 pagesHipertensi Pregnancy PICOarcita hanjaniNo ratings yet
- Endocrine HypertensionDocument43 pagesEndocrine HypertensionAlessia GuerraNo ratings yet
- Jurnal 2Document6 pagesJurnal 2IrdaniatiNo ratings yet
- GSIS v. CalumpianoDocument16 pagesGSIS v. CalumpianoHelenErasmo0% (1)
- Medical - Surgical Nursing QuestionDocument20 pagesMedical - Surgical Nursing QuestionChy ChyNo ratings yet
- Principles of SurgeryDocument87 pagesPrinciples of SurgeryfiansisNo ratings yet
- Practice OSCE StationsDocument4 pagesPractice OSCE StationsAemelia MelloyNo ratings yet
- Alternative System of MedicineDocument13 pagesAlternative System of MedicineDebipriya Mistry100% (2)
- The Most Effective Natural Cures On Earth - Johnny BowdenDocument257 pagesThe Most Effective Natural Cures On Earth - Johnny BowdenLewis John50% (4)
- DNP Cohort 5 Capstone AbstractsDocument26 pagesDNP Cohort 5 Capstone AbstractsAntónio AlmeidaNo ratings yet
- Prioritization of ProblemsDocument4 pagesPrioritization of Problemsaron frondaNo ratings yet
- CVS History TakingDocument1 pageCVS History Takingdrdrahmood709No ratings yet
- Hypertension - PPT RKDocument31 pagesHypertension - PPT RKseetaramanath100% (3)
- Interna Prof. Djanggan - Kapita SelektaDocument53 pagesInterna Prof. Djanggan - Kapita SelektaNur Laily MardianaNo ratings yet