
2015 Article 15 PDF
Uploaded by
Andrei FrincuCopyright:
Available Formats
2015 Article 15 PDF
Uploaded by
Andrei FrincuOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
2015 Article 15 PDF
Uploaded by
Andrei FrincuCopyright:
Available Formats
Lafitte et al.
BMC Cardiovascular Disorders (2015) 15:23
DOI 10.1186/s12872-015-0015-3
RESEARCH ARTICLE
Open Access
High sensitivity C reactive protein, fibrinogen
levels and the onset of major depressive disorder
in post-acute coronary syndrome
Marianne Lafitte1, Sandrine Tastet1, Paul Perez2, Marie-Aime Seris1, Anne-Sophie Grandoulier2, Bruno Aouizerate3,
Igor Sibon4, Lucile Capuron5 and Thierry Couffinhal1,6,7*
Abstract
Background: Major depression disorder (MDD) is a common condition in patients suffering from acute coronary
syndrome (ACS), and depression is a risk factor for mortality following an ACS. Growing evidence suggests that
there is an intricate interplay between atherosclerosis, inflammation and depression. The aim of this study was to
investigate the role of atherosclerosis-induced inflammation in the mediation of MDD.
Methods: 87 patients without depression were recruited at the time of an ACS, evaluated at 3 and 7 days and followed
at 1, 3 and 9 months for the occurrence of a MDD as assessed by structured interviews (MINI). At each time point, they
were monitored for inflammatory markers (high sensitivity C Reactive Protein {hsCRP} and fibrinogen), cardiovascular risk
factors and atherosclerosis burden. Association between possible predictive characteristics and depression was assessed
using a multivariable logistic regression model.
Results: The overall incidence of MDD, in this population, was 28.7% [95% CI: 19.5 39.4] during the 9-month follow up
period. Elevated hsCRP was not associated with depression onset after an ACS (adjusted OR: 1.07 [0.77 - 1.48]; p = 0.70),
and similarly no association was found with fibrinogen. Furthermore, we found no association between hsCRP,
fibrinogen or atherosclerosis burden at any time-point, and the occurrence of a MDD (or HDRS-17 and MADRS).
The only factor associated with depression occurrence after an ACS was a previous personal history of depression
(adjusted OR: 11.02 [2.74 to 44.34]; p = 0.0007).
Conclusions: The present study shows that after an ACS, patients treated with optimal medications could have a
MDD independent of elevated hsCRP or fibrinogen levels. Personal history of depression may be a good marker
to select patients who should be screened for depression after an ACS.
Keywords: Depression, Inflammatory marker, CRP, Fibrinogen, Acute coronary syndrome, Atherosclerosis
Background
Major depression disorder (MDD) is a common condition
in patients suffering from acute coronary syndrome
(ACS), affecting approximately 20% of patients during
hospitalization and a similar proportion within the first
year after ACS [1,2]. Depressive symptoms, even in the absence of formal diagnosis of MDD, are strong independent
* Correspondence: thierry.couffinhal@u-bordeaux.fr
1
CHU de Bordeaux, Centre dExploration, de Prvention et de Traitement de
lAthroclrose, CEPTA, Hpital Cardiologique du Haut-Lvque, Avenue de
Magellan, 33604 PESSAC Cedex, F-33000 Bordeaux, France
6
Univ. Bordeaux, Adaptation cardiovasculaire lischmie, U1034, F-33600
Pessac, France
Full list of author information is available at the end of the article
predictors of cardiovascular morbidity and mortality after
ACS [3,4].
Understanding the mechanisms underlying the onset
of depression, and identifying early markers that predict
its occurrence in patients after ACS, could have major
clinical implications in both the optimal management of
depression and secondary prevention of coronary artery
disease (CAD) [5].
However, the mechanisms specifically involved in the
association between cardiovascular disease and depression
have not been clearly established. Growing evidence
suggests that there is an intricate interplay between
atherosclerosis, inflammation and depression [6]. These
2015 Lafitte et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the Creative
Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain
Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,
unless otherwise stated.
Lafitte et al. BMC Cardiovascular Disorders (2015) 15:23
inter-relations have been reported in the literature in different ways: depression is frequently diagnosed in patients
with CAD and MDD is a powerful risk factor for CAD
events [7-9]. Atherosclerosis is fundamentally an inflammatory disease and inflammatory markers are powerful
predictors of CAD events [10,11]. MDD is associated with
an increased level of markers of inflammation and can
be induced by pro-inflammatory treatment or cytokine
therapy in medically ill patients [12-18].
Therefore, it would be reasonable to hypothesize that
the link between CAD and depression might be mediated
by inflammation. However, the causal and temporal
mechanisms underlying the inter-relationships between
CAD, inflammation and depression have not been well
characterized.
The primary objective of the present study was to investigate the prognostic value of hsCRP or fibrinogen (as
surrogate markers of inflammation) in detecting new MDD,
after an ACS. For this purpose, we excluded patients
who had a diagnosis of depression at study entry, or were
receiving treatment for depression. We hypothesized that
high, followed by low-grade systemic inflammation, after
an ACS (as measured by serum hsCRP and fibrinogen
levels), could induce and be a biological marker able to
predict depression. The secondary objective was to investigate other factors that might predict the development of depression after an ACS.
Methods
Patients
Between May 2006 and September 2007, a total of 146
potentially eligible patients were admitted to our department 23 days after an acute coronary syndrome (ACS).
The present study enrolled patients 3075 year old with
an ACS, defined as previously reported [19]. Specific exclusion criteria with respect to depression, anti-inflammatory
drugs and inflammatory diseases, were as follows:
A previous history of either major depressive disorder
(MDD) within the last 6 months or treatment for
depression within the last 6 months; a current diagnosis
of MDD and/or ongoing treatment for depression at the
time of hospitalization for ACS. Patients who had a
major psychiatric disorder other than affective disorders
were also excluded (e.g., schizophrenia, dementia,
present psychotic episode).
A treatment by steroid, COX-2 selective inhibitor
or other non-steroidal anti-inflammatory drug
(aspirin > 325 mg) for more than 7 days before
hospitalization for ACS.
A surgery in the last month, presence of a severe
systemic or infectious disease, autoimmune disorder,
inflammatory disorder, or HIV, treatment with dialysis,
or a malignancy with decreased life expectancy.
Page 2 of 9
Other exclusion criteria included unstable medical or
neurologic condition and patients who were unable to
communicate reliably (e.g., because of cognitive dysfunction or not speaking French).
The Ethics Committee review board of the hospital
(CPP SOOM III, Bordeaux) approved the study protocol,
and all participants provided informed consent prior to participation. All standard of care cardiovascular treatments
were permitted during the trial. Concomitant medication,
including steroids, COX-2 selective inhibitors and other
non-steroidal anti-inflammatory treatments were recorded
during the study.
Acute phase management
ACS was defined and treated according to established
guidelines [20]. A coronary angiogram was performed on
each patient included in the study, allowing precise evaluation of coronary lesions, and optimized acute phase
management. The most suitable treatment was delivered
during the first week, in compliance with current guidelines [20].
Psychiatric assessment
The Mini-international neuropsychiatric interview
(MINI) was used to assess the incidence of MDD.
MINI is a short structured clinical interview, which
enables researchers to make a diagnosis of psychiatric
disorders according to DSM-IV or ICD-10 [21]. Patients
were classified as having MDD or not based upon results
of the MINI.
The Hamilton Depression Rating Scale (HDRS-17), is
a clinician-administered questionnaire assessing the
severity of depressive symptoms, including low mood,
insomnia, agitation, anxiety and weight loss [22].
HDRS-17 assesses severity of, and change in, depressive
symptoms over time.
The Montgomery-sberg Depression Rating Scale
(MADRS), is a ten-item clinician-administered
questionnaire assessing the severity and evolution of
depressive symptoms [22]. The MADRS is one of the
most frequently used and validated observer-rated
depression scales.
Procedure
Patients meeting the inclusion criteria were invited to
participate as soon as they were medically stable and had
been informed of their diagnosis, on average 2 days after
their ACS (range, 24 days). After explaining the study
and obtaining written informed consent, a research psychologist (S.T.) conducted all baseline psychiatric interviews, and gathered routine demographic data, including
age, gender, education, living arrangements, current partner status, socioeconomic status and employment status
Lafitte et al. BMC Cardiovascular Disorders (2015) 15:23
(employed or unemployed). Information on history of familial and personal depression, or other psychiatric illness
was collected during hospitalization.
During the assessment period, if the MINI was positive
for a diagnosis of MDD, the patient was excluded from
the study. If it was negative, the other psychiatric interviews were performed, as well as an evaluation of hsCRP
and fibrinogen levels along with other classical risk factors.
All patients benefited from the CEPTA program with
an optimization of secondary prevention measures and
educational classes as previously described [19,23].
Patients were followed at 1, 3 and 9 months after ACS.
At each time point, cardiovascular risk factors, treatment,
levels of hsCRP and fibrinogen were recorded, and psychiatric interviews were performed. The cardiologists and the
care team were blinded to the depression status over the
9 month follow-up period. Patients with depressive symptoms were not treated with antidepressant medication,
due to the lack of evidence of a clear benefit of depression
screening, and of antidepressant medication in this patient
population, on cardiovascular disease (CVD) outcome. Instead these patients were sent to a mental health professional for psychotherapy alone.
End point
To assess the incidence of MDD, the psychologist administered the MINI at 3 days and 1, 3 and 9 months, after an
ACS. The psychologist also conducted the HDRS-17 and
MADRS interviews at 3 days, 1, 3 and 9 months, to score
the intensity and evolution of depression symptoms.
To assess the inflammatory status, hsCRP and fibrinogen levels were measured at 3 and 7 days, 1, 3 and
9 months. hsCRP was measured by immuno-turbidimetry,
with a detection limit of 0.02 mg/L (Rock Diagnoses). The
assays were performed blinded to patients depression
status; plasma samples drawn at baseline were frozen
at 70C for subsequent measurement of inflammatory
[19] markers.
The 9-month survival status was determined for all
patients after their ACS. Cause of death was established
from hospital and general practitioner records and death
certificates. Deaths were classified as cardiac or noncardiac by a consulting cardiologist blinded to baseline
data.
Statistics
Continuous variables were described by mean and standard deviation, and compared using Students t tests.
Categorical variables were described by numbers and proportions, and compared using Chi-square tests. Comparisons were considered statistically significant when the p
value was <0.05, and corrected according to the Bonferroni rule in case of multiple testing. The incidence rate
of MDD was estimated by the proportion of patients
Page 3 of 9
presenting with at least one positive MINI at any time
point divided by the total number of patients followed
during the 9-month period after an ACS. Ninety-five
percent confidence intervals (95% CI) of proportions and
incidence rates were calculated by the exact binomial
method. The association between patient characteristics
and the diagnosis of MDD was assessed by logistic regression models, using standard recommended methods. The
strength of the association between predictors and MDM
was estimated by calculating the odds ratios (OR) and
their 95% CIs. Linearity of the logit was systematically
checked for every continuous variable. A limited number
of possible predictive variables were chosen on the basis
of previous reports (age, female gender, familial and
personal history of depression, low socio-economic level,
living alone, atherosclerosis burden, LDL cholesterol, metabolic syndrome, smoking and GT). Their association with
the occurrence of depression was first tested in univariate
logistic regression analysis. Then, all variables associated
with depression with a p value < 0.20 were introduced into
the multivariable model. The variable of interest, hsCRP
level at discharge, was forced into the model. The full
model was kept without further selection, as the aim was
to obtain an estimate of the association of hsCRP with depression, adjusted based on possible confounding factors.
In cases where there was missing data for either hsCRP
or MINI, sensitivity analyses were carried out. Exploratory
analysis of the association between the evolution of
depressive symptoms, as assessed by MADRS, and the
evolution of hsCRP was carried out using a mixed linear model.
All analyses were carried out using SAS software v9.1.3
(SAS Institute Inc., Cary, North Carolina, USA).
Results
Incidence and time course of depressive symptoms
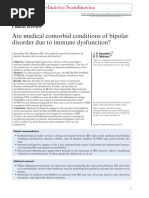
The study population flow chart is shown in Figure 1. At
the time of ACS, none of the 87 patients included in
the study had a MDD, or a history of MDD less than
6 months before their initial hospitalization. New onset
of depression was recorded in 8.0% of the patients at
1 month, 10.3% at 3 months and 10.3% at 9 months. A
patient was categorized as part of the depression group
if he or she had a MDD at any time point during follow
up, as assessed by the MINI. The overall 9-month incidence of a MDD was 28.7% [95% CI: 19.5 39.4]. At
9 months, 19.5% of patients (prevalence) still met the
criteria for diagnosis of depression.
Patients characteristics according to depressive symptoms
status
There were no significant differences in general characteristics and the risk factor profile, between patients who
remained free of MDD (non-depression group) versus
Lafitte et al. BMC Cardiovascular Disorders (2015) 15:23
Page 4 of 9
Figure 1 Flow chart of the study population.
those who developed MDD (depression group) at any of
the follow up time points, with the exception of prior
history of depression (Table 1 and Additional file 1:
Table S1). There were significantly more patients in the
depression group who reported having a prior history of
depression, than in the non-depression group (88%, vs
37.1% p < 0.0001).
There was no association found between depressive
symptom status and atherosclerosis burden (Table 1), or
major cardiovascular events (such as reinfarction, stroke
Lafitte et al. BMC Cardiovascular Disorders (2015) 15:23
Page 5 of 9
Table 1 General characteristics, atherosclerosis burden,
acute phase management and medical treatments at
discharge, grouped according to the depression status
over a 9-month follow-up after ACS
No Depression
71.3%
Depression
28.7%
49.0 8.8
52.2 9.2
General characteristics
Mean Age sd (years)
Female gender (%)
6.4
16.0
Personal history of CV disease (%)
8.1
16.0
Family history of CV disease (%)
17.7
28.0
Personal history of depression (%)
37.1
88.0 **
Familial history of depression (%)
25.8
20.0
Live alone (%)
17.7
24.0
Widow(er)/divorcee/separated (%)
45.1
48.0
Low Socio-economic level (%)
8.0
16.0
Mean number of coronary vessels
>50% stenosis
1.4+/0.8
1.6+/0.6
ABI < 0.9 (%)
11
Carotid stenosis >20% (%)
18.6
22.2
IMT > 0.7 mm (%)
63
60
Revascularisation (%)
91.9
92.0
Conventional Treatment (%)
8.1
8.0
Beta-blocker and/or calcium antagonist
96.7%
96.0%
Cholesterol-lowering medication
93.5%
100.0%
Antiplatelet therapy or warfarin
100.0%
100.0%
ACE inhibitor or Angiotensin II receptor
agonist
100.0%
96.0%
Combination of anti-ischemic/
antiplatelet/Lipid-lowering drug
90.3%
96.0%
Atherosclerosis Burden
ACS treatment
Post ACS medications at discharge
*p values of tests comparing the No depression and Depression groups
(Students t test for age, Chi square tests for proportions). * p < 0.05;
** p < 0.01.
or death) during the 9 months follow-up period (3 ACS
and 1 stroke occurred in the non-depression group vs.
no event in the depression group).
Acute phase management and optimal medical treatment were similar in both groups of patients (MDD vs.
no depression) at discharge (Table 1) and during the
follow-up period (not shown).
Association between hsCRP and occurrence of major
depressive disorder
According to HDRS-17 and MADRS scales, the majority
of these MDD patients were classified as having mild
to moderate depression (Table 2). No difference in
hsCRP levels was detected between the depression and
non-depression groups at any time-point (Table 2). The
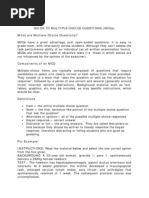
evolution of mean hsCRP levels was similar in the two
groups and even individual values did not show any trend
(Figure 2 and Additional file 1: Figures S1 and S2). In univariate, unadjusted analysis, hsCRP measured at day 7 was
not associated with the occurrence of a MDD during the
9-month follow-up period after the ACS. The odds ratio
for a MDD during the first 3 months was 0.96 (95% CI:
0.88 - 1.05; p = 0.37) and the odds ratio for a MDD during
the first 9 months was 1.02 (95% CI: 0.97 - 1.07; p = 0.53)
(Table 3). We also estimated the association between
hsCRP measured at 1 and 3 months and the occurrence of
a MDD during the first 3 or 9 months, but all odds ratios
were close to 1 and not statistically significant (Table 3).
In multivariable analysis, i.e. when taking into account
other characteristics, hsCRP was not associated with the
occurrence of MDD during the first nine months period
after ACS. The adjusted OR was 1.07 (95% CI: 0.77 -1.48;
p = 0.70) (Table 4).
Statistics were done on 87 of 98 patients originally included. Eleven patients were not analysed because at
least one MINI was missing at a time point. Sensitivity
analyses were carried out by replacing missing values on
MINI and hsCRP according to different strategies. All
11 missing depression statuses were replaced by absence,
then by presence of depression, without generating a
significant association between hsCRP D7 and 9-month
Table 2 Depression severity and intensity, as measured with HDRS-17 and MADRS scales (mean sd) and evolution of
the inflammatory profile, as measured by hsCRP and fibrinogen levels, according to the depression status over a
9-month follow-up period after an ACS
D7
No Depression
71.3%
M1
Depression
28.7%
No Depression
71.3%
M3
Depression
28.7%
No Depression
71.3%
M9
Depression
28.7%
No Depression
71.3%
Depression
28.7%
MADRS
5.5 3
6.9 4
5.7 4
13.9 8*
6.2 4
18.2 8**
5.5 5
21.0 8**
HDRS-17
6.7 3
9.2 4
9.0 5
14.0 7*
8.6 5
17.2 7*
7.5 5
20.1 5**
hs-CRP (mg/l)
8.7 8.0
10.1 11.0
2.30 2.3
3.05 4.2
2.12 2.5
2.27 3.8
2.65 6.4
2.46 3.4
Fibrinogen (g/l)
5.22 1.1
5.62 1.2*
3.97 0.7
4.18 1.1
3.65 0.6
3.62 1.0
3.69 0.8
4.16 0.8*
*p values of tests comparing the No depression and Depression groups (Students t test for age, Chi square tests for proportions). *p < 0.05; **p < 0.01.
Lafitte et al. BMC Cardiovascular Disorders (2015) 15:23
Page 6 of 9
Table 4 Multivariable analysis of association between the
depression status over a 9-month follow-up period after
ACS and variables recorded at day 7
Variables measured at D7
OR [95% CI]
hsCRP at D7
1.07 [0.77 - 1.48]
Gender (women)
1.55 [0.21 11.35]
Personal history of depression
11.02 [2.74 - 44.34]*
GT > = 50
2.30 [0.67 7.89]
HDRS-17
1.08 [0.92 - 1.26]
*p < 0.001.
Figure 2 Comparison of hsCRP evolution (mean+/ SD) in the
group of patient with no depression versus patients with
depression.
depression occurrence. When the 9 missing values of
hsCRP D7 were replaced by the highest hsCRP value
(46.3) for the patients of the depressed group and the
lowest hsCRP value (0.3) for the patients of the nondepressed group, no significant association was found.
Moreover, we found no association between hsCRP at
day 7 and either HDRS-17 or MADRS scores at months
1, 3 and 9 (not shown). We also used a mixed linear
model for studying the association between the evolution
of depressive symptoms, as assessed by MADRS, and the
evolution of hsCRP, between inclusion and one-month
follow-up. No association was found (p = 0.69). The
evolution of hsCRP values was quite similar after the
one-month follow-up (Figure 2).
Table 3 Univariate association between hsCRP or fibrinogen
measured at 3 or 7 days, 1 and 3 months (as indicated) and
the occurrence of a MDD during the first 3 or 9 months
Variable
Time of depression
OR
IC 95%
p-value
hsCRP D7
In the first 3 months
0.96
[0.88 ; 1.05]
0.37
hsCRP D7
In the first 9 months
1.02
[0.97 ; 1.07]
0.53
hsCRP M1
In the first 3 months
0.90
[0.67 ; 1.20]
0.46
hsCRP M1
In the first 9 months
1.08
[0.93 ; 1.26]
0.32
hsCRP M3
In the first 3 months
0.85
[0.61 ; 1.20]
0.36
hsCRP M3
In the first 9 months
1.02
[0.86 ; 1.20]
0.84
Variable
Time of depression
OR
IC 95%
p-value
Fibrinogen D3
In the first 3 months
1.01
[0.60 ; 1.69]
0.97
Fibrinogen D3
In the first 9 months
1.38
[0.92 ; 2.08]
0.12
Fibrinogen M1
In the first 3 months
0.78
[0.39 ; 1.56]
0.49
Fibrinogen M1
In the first 9 months
1.22
[0.72 ; 2.09]
0.46
Fibrinogen M3
In the first 3 months
0.70
[0.33 ; 1.51]
0.37
Fibrinogen M3
In the first 9 months
0.89
[0.48 ; 1.66]
0.71
Patients diagnosed as depressed at any time point, had
higher fibrinogen levels at baseline and at their 9 months
assessment, than their non-depressed counterparts, but
this difference was not statistically significant at 1 and
3 month assessment (Table 2). Moreover, there was no
significant association between fibrinogen values and the
occurrence of depression during different periods of time,
as analyzed by univariate logistic regression (Table 3).
Predictive factors of a major depressive disorder during
the 9 months following an ACS
We evaluated the association between quantitative and
non-quantitative characteristics and CV risk factors of
the population, as well as parameters of atherosclerosis
burden, with MDD occurrence. A limited number of possible predictive variables were chosen on the basis of previous reports in the literature. In univariate (Additional
file 1: Table S2) as well as in the above-mentioned multivariable analyses (Table 4), only the personal history of
depression (more than 6 month before ACS) was significantly associated with the onset of a depressive episode during the 9-month follow-up period, with an OR
of 11.02 (95% confidence interval [CI], 2.74 to 44.34; p =
0.0009) adjusted for gender, hsCRP, Gamma-GT at day 7
and HDRS-17 score at inclusion (Table 4).
Discussion
The aim of this study was to determine whether or not
atherosclerosis-induced inflammation plays a role in the
mediation of MDD and, to examine predictive markers
of depression after an ACS. To our knowledge, this is
the first study to assess the prognostic importance of
hsCRP (and fibrinogen) in the development of MDD after
an ACS. This study included only patients without a
current, or recent (within 6-months) past history, of depression, as determined by a structured clinical interview.
All patients were provided with optimal treatment for
their cardiovascular disease.
Although the incidence of depression was high, we found
no association between hsCRP or fibrinogen and MDD
after an ACS. Therefore, the present data do not support
the hypothesis that hsCRP or fibrinogen (as surrogates of
Lafitte et al. BMC Cardiovascular Disorders (2015) 15:23
inflammation) are an indispensable trigger of depression
after ACS in a population treated with optimal medication
nor that the reported prognostic impact of depression can
be explained by these markers. The only factor associated
with depression occurrence after an ACS was a previous
personal history of depression.
Time course and incidence of depression
A comprehensive literature review of hospitalized post-MI
patients, revealed a prevalence rate for MDD of approximately 20%, when measured using clinical interviews
[24,25]. Our results show that, in the 9 months following
an ACS, 28.7% of patients developed MDD. We chose to
exclude patients with a history of depression within the
last six months and those who were depressed at the time
of initial hospitalization for their ACS [26]. Therefore, this
study highlights the high incidence of new cases of MDD
after an ACS and the long delay in occurrence after the
onset of ACS.
Inflammation as assessed by levels of hsCRP and
fibrinogen is not likely to be the mechanism underlying
depression
Depression can be a risk factor for the development of
CAD, and often exacerbates the outcome, when present
in patients with established CAD [7-9]. Atherosclerosis is
fundamentally an inflammatory disease and inflammatory
markers are powerful predictors of CAD events [10,11].
Depression and inflammation have each been independently associated with CAD [6,12,13,15,17,18,27-33]. The
interplay between depression, inflammation, and CVD or
mortality is complex, and may be analyzed in several different ways based on literature [6-13,15,17,18,27-32] : (i)
depression may induce inflammation, and the latter
mediate independently the relationship between depression and CVD; (ii) both depression and inflammation may cause CVD but through separate pathways,
being synergistic or not; (iii) depression and inflammation may have a common precursor that is linked to
CVD; or (iv) inflammation may cause depression and
each may or may not have a causal role on CVD [6].
The primary focus of this study was to determine whether
or not inflammation may cause depression, because of the
importance of inflammation in atherosclerosis. In this study,
we found no significant association between atherosclerosis
burden, hsCRP or fibrinogen levels at any time point and
depressive symptoms after an ACS. The point estimation of the OR was close to one (1.07), favoring the
conclusion of an absence of association. However, due
to the limited number of patients, the precision of the
estimate was low (95% confidence interval: 0.77 - 1.48).
Various sensitivity analyses were conducted by imputing
extreme values for missing data but none resulted in an association between hsCRP and MDD. Exploratory analyses
Page 7 of 9
did not show an association between the evolution of
hsCRP and the evolution of depression scales. These arguments reinforce the confidence in this null result.
Therefore, this study supports the hypothesis that patients after an ACS may have a MDD independent of
an elevated hsCRP or fibrinogen level.
These data are in contrast to epidemiological and clinical studies which have suggested that inflammation precedes the occurrence of depression as in patients with
cancer treated with immunotherapy [17,18,27,29,33,34].
Previous studies on atherosclerosis, inflammation and
depression [6] have been limited to selected clinical samples and/or have failed to control for important confounding factors [12]. It is not clear to what extent these
associations are due to coexisting cardiovascular risk
factors and comorbidity, or the greater severity of atherosclerotic disease among patients with depression [6].
There are several factors which may explain why our
results are not consistent with these previous reports of
the association between ACS, depression, and biomarkers
of inflammation.
In our study, we used a structured diagnostic interview,
the gold standard for defining clinical depression, while
very few reports in the literature have used an interviewbased study to examine the relationships between CVD,
depression and inflammation. The majority of studies have
used self-reported questionnaires such as the Beck
Depression Inventory, to define depression, which are
not specific for clinical depression. Thus, an elevated
score may reflect transient sadness, anxiety, other psychiatric
disorders, general distress secondary to a life-threatening experience, or even the symptoms of the medical illness [35].
In our study, patients who had a diagnosis of depression
at study entry were excluded. If individuals with a known
diagnosis of depression were not excluded, the cohorts
would have had a greater prevalence of depression, than
those where only individuals without clinically recognized
depression were screened, and the relationship with inflammation could be skewed [26].
We also assessed depression at four time points, where
as in the majority of studies examining the interaction of
depressive symptoms with inflammation in patients with
ACS have measured depressive symptoms only at the
time of the hospitalization for ACS. Depressive symptoms
at this stage may reflect transient reactive depression
that may undergo spontaneous remission [5].
Finally, the association between depression and inflammation reported in the literature could be explained by
inconsistencies in monitoring risk factors for CVD, comorbidity, and CAD severity [6]. In our study we were
able to control these factors, which could confound the
association between depression and inflammation [6].
One difficulty in interpretation of reports in the literature, is the impact of medication such as statins [36]. In
Lafitte et al. BMC Cardiovascular Disorders (2015) 15:23
Page 8 of 9
addition to their effects on cholesterol synthesis, statins
also act as immunomodulators with pronounced antiinflammatory properties [37]. Because of the optimal
medical treatment provided to all patients during the
9 month follow-up period, we were able to minimize these
confounding factors.
Identifying a marker of depression onset after ACS to
improve screening
Due to the negative impact of depression on CVD outcome, in patients with CAD, identifying the onset of a
MDD is particularly relevant for prevention and intervention [25,26,38-40].
Among all the markers tested in our model only personal history of depression was strongly associated with
the occurrence of a MDD during the 9 months following
an ACS. Personal history of depression identified patients
with a greater vulnerability that were prone to depression.
This marker is easy to assess, and may allow physicians to
determine which patients could benefit from depression
screening.
Limitation of the study
We acknowledge that this study has a limited number of
patients that limit the power of some of statistical analyses
and conclusions, namely in showing associations between
clinical parameters and MDD occurrence (i.e. interaction
between CRP and depression depending on the gender).
It is worth noting that levels of hsCRP and fibrinogen
may not recapitulate all inflammatory processes, namely
central nervous system inflammation. On the other hand,
most often an increase in the levels of TNF-, IL-1 or
IL-6 will result in an increase in hsCRP or fibrinogen
levels. However, it may be interesting to introduce other
inflammatory markers in future studies.
This study is an exploratory study that may generate
new knowledge and hypothesis, but it needs to be
replicated.
Conclusions
The present study demonstrates that after an ACS, patients treated with optimal medication can have a MDD
independent of elevated levels of hsCRP or fibrinogen.
Our data does not support the hypothesis that inflammation is a trigger for depression after ACS. Personal history
of depression may be a good marker to select patients
who should be screened for depression after an ACS.
Additional file
Additional file 1: Table S1. Cardiovascular risk factor profile of the
population. Patients were classified according to their depressive disorder
status. A patient was considered as depression if they had a major
depression disorder at any time point during the follow up. (* p<.05,
comparison between depression and non depression group for each
time point). Table S2: Univariate analysis of the association between the
depression status over a 9-month follow-up after ACS and variables recorded
at day 7. Figure S1: hsCRP evolution in patients with no depression, during
the 9-month follow-up period. Figure S2: hsCRP evolution in patients with at
least one MINI positive, during the 9-month follow-up period.
Abbreviations
ACS: Acute coronary syndrome; CVD: Cardiovascular disease; CAD: Coronary
artery disease; hsCRP: High sensitivity C reactive protein; MDD: Major depression
disorder; MINI: Mini-international neuropsychiatric interview; HDRS-17: Hamilton
depression rating scale; MADRS: Montgomery-sberg depression rating scale.
Competing interests
The authors declare that they have no competing interests.
Authors contributions
TC, PP, LC conceived of the study, and its design and coordination. ML, ST,
MAS, TC carried out the study. BA, IS participated in the design of the study
and helped to draft the manuscript. TC, PP, ASG performed the statistical
analysis. TC, PP drafted the manuscript. All authors read and approved the
final manuscript.
Acknowledgments
The authors wish to thank Sandrine Lapouge for her assistance in data
collection, and Catherine Maldonado (USMR, University Hospital Bordeaux)
for data management.
Author details
CHU de Bordeaux, Centre dExploration, de Prvention et de Traitement de
lAthroclrose, CEPTA, Hpital Cardiologique du Haut-Lvque, Avenue de
Magellan, 33604 PESSAC Cedex, F-33000 Bordeaux, France. 2CHU de
Bordeaux, Unit de Soutien Mthodologique la Recherche Clinique et
Epidmiologique, F-33000 Bordeaux, France. 3CHU de Bordeaux, Ple
Universitaire de Psychiatrie, F-33000 Bordeaux, France. 4CHU de Bordeaux,
Unit Neurovasculaire, F-33000 Bordeaux, France. 5INRA, Nutrition et
Neurobiologie intgre, UMR 1286, F-33000 Bordeaux, France. 6Univ.
Bordeaux, Adaptation cardiovasculaire lischmie, U1034, F-33600 Pessac,
France. 7INSERM, Adaptation cardiovasculaire lischmie, U1034, F-33600
Pessac, France.
1
Received: 6 October 2014 Accepted: 27 February 2015
References
1. Lesperance F, Frasure-Smith N, Talajic M. Major depression before and after
myocardial infarction: its nature and consequences. Psychosom Med.
1996;58:99110.
2. Schleifer SJ, Macari-Hinson MM, Coyle DA, Slater WR, Kahn M, Gorlin R, et al.
The nature and course of depression following myocardial infarction. Arch
Intern Med. 1989;149:17859.
3. van Melle JP, de Jonge P, Spijkerman TA, Tijssen JG, Ormel J, van Veldhuisen DJ,
et al. Prognostic association of depression following myocardial infarction
with mortality and cardiovascular events: a meta-analysis. Psychosom Med.
2004;66:81422.
4. Frasure-Smith N, Lesperance F, Talajic M. Depression following myocardial
infarction. Impact on 6-month survival. JAMA. 1993;270:181925.
5. Parashar S, Rumsfeld JS, Spertus JA, Reid KJ, Wenger NK, Krumholz HM, et al.
Time course of depression and outcome of myocardial infarction. Arch
Intern Med. 2006;166:203543.
6. Vaccarino V, Johnson BD, Sheps DS, Reis SE, Kelsey SF, Bittner V, et al.
Depression, inflammation, and incident cardiovascular disease in women
with suspected coronary ischemia: the National Heart, Lung, and Blood
Institute-sponsored WISE study. J Am Coll Cardiol. 2007;50:204450.
7. Frasure-Smith N, Lesperance F, Gravel G, Masson A, Juneau M, Talajic M,
et al. Social support, depression, and mortality during the first year after
myocardial infarction. Circulation. 2000;101:191924.
8. Lesperance F, Frasure-Smith N, Talajic M, Bourassa MG. Five-year risk of cardiac
mortality in relation to initial severity and one-year changes in depression
symptoms after myocardial infarction. Circulation. 2002;105:104953.
Lafitte et al. BMC Cardiovascular Disorders (2015) 15:23
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
Frasure-Smith N, Lesperance F, Habra M, Talajic M, Khairy P, Dorian P, et al.
Elevated depression symptoms predict long-term cardiovascular mortality in
patients with atrial fibrillation and heart failure. Circulation. 2009;120:13440.
133p following 140.
Libby P, Theroux P. Pathophysiology of coronary artery disease. Circulation.
2005;111:34818.
Ridker PM. C-reactive protein and the prediction of cardiovascular events
among those at intermediate risk: moving an inflammatory hypothesis
toward consensus. J Am Coll Cardiol. 2007;49:212938.
Danner M, Kasl SV, Abramson JL, Vaccarino V. Association between depression
and elevated C-reactive protein. Psychosom Med. 2003;65:34756.
Empana JP, Sykes DH, Luc G, Juhan-Vague I, Arveiler D, Ferrieres J, et al.
Contributions of depressive mood and circulating inflammatory markers
to coronary heart disease in healthy European men: the Prospective
Epidemiological Study of Myocardial Infarction (PRIME). Circulation.
2005;111:2299305.
Berk M, Wadee AA, Kuschke RH, ONeill-Kerr A. Acute phase proteins in
major depression. J Psychosom Res. 1997;43:52934.
Miller GE, Stetler CA, Carney RM, Freedland KE, Banks WA. Clinical
depression and inflammatory risk markers for coronary heart disease. Am J
Cardiol. 2002;90:127983.
Capuron L, Ravaud A, Neveu PJ, Miller AH, Maes M, Dantzer R. Association
between decreased serum tryptophan concentrations and depressive
symptoms in cancer patients undergoing cytokine therapy. Mol Psychiatry.
2002;7:46873.
Raison CL, Capuron L, Miller AH. Cytokines sing the blues: inflammation and
the pathogenesis of depression. Trends Immunol. 2006;27:2431.
Dantzer R, OConnor JC, Freund GG, Johnson RW, Kelley KW. From inflammation
to sickness and depression: when the immune system subjugates the brain. Nat
Rev. 2008;9:4656.
Riedel M, Lafitte M, Pucheu Y, Latry K, Couffinhal T. Prognostic value of
high-sensitivity C-reactive protein in a population of post-acute coronary
syndrome patients receiving optimal medical treatment. Eur J Prev Cardiol.
2012;19:112837.
Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK,
et al. 2007 Focused Update of the ACC/AHA 2004 Guidelines for the
Management of Patients With ST-Elevation Myocardial Infarction: a report of
the American College of Cardiology/American Heart Association Task Force
on Practice Guidelines. Circulation. 2008;117:296329.
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al.
The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development
and validation of a structured diagnostic psychiatric interview for DSM-IV
and ICD-10. J Clin Psychiatry. 1998;59 Suppl 20:2233. quiz 3457.
Demyttenaere K, De Fruyt J. Getting what you ask for: on the selectivity of
depression rating scales. Psychother Psychosom. 2003;72:6170.
Lafitte M, Pucheu Y, Latry K, Dijos M, Casassus E, Couffinhal T. Predictors of
cardiovascular prognosis in patients receiving optimized secondary prevention
measures after acute coronary syndrome. Eur J Prev Cardiol. 2013;20:28390.
Thombs BD, Bass EB, Ford DE, Stewart KJ, Tsilidis KK, Patel U, et al. Prevalence
of depression in survivors of acute myocardial infarction. J Gen Intern Med.
2006;21:308.
Thombs BD, de Jonge P, Coyne JC, Whooley MA, Frasure-Smith N, Mitchell
AJ, et al. Depression screening and patient outcomes in cardiovascular care:
a systematic review. JAMA. 2008;300:216171.
Thombs BD, Arthurs E, El-Baalbaki G, Meijer A, Ziegelstein RC, Steele RJ. Risk
of bias from inclusion of patients who already have diagnosis of or are
undergoing treatment for depression in diagnostic accuracy studies of
screening tools for depression: systematic review. BMJ. 2011;343:d4825.
Poole L, Dickens C, Steptoe A. The puzzle of depression and acute coronary
syndrome: reviewing the role of acute inflammation. J Psychosom Res.
2011;71:618.
Howren MB, Lamkin DM, Suls J. Associations of depression with C-reactive
protein, IL-1, and IL-6: a meta-analysis. Psychosom Med. 2009;71:17186.
Gimeno D, Kivimaki M, Brunner EJ, Elovainio M, De Vogli R, Steptoe A, et al.
Associations of C-reactive protein and interleukin-6 with cognitive symptoms
of depression: 12-year follow-up of the Whitehall II study. Psychol Med.
2009;39:41323.
Frasure-Smith N, Lesperance F, Irwin MR, Talajic M, Pollock BG. The
relationships among heart rate variability, inflammatory markers and
depression in coronary heart disease patients. Brain Behav Immun.
2009;23:11407.
Page 9 of 9
31. Frasure-Smith N, Lesperance F, Irwin MR, Sauve C, Lesperance J, Theroux P.
Depression, C-reactive protein and two-year major adverse cardiac events in
men after acute coronary syndromes. Biol Psychiatry. 2007;62:3028.
32. Lesperance F, Frasure-Smith N, Theroux P, Irwin M. The association between
major depression and levels of soluble intercellular adhesion molecule 1,
interleukin-6, and C-reactive protein in patients with recent acute coronary
syndromes. Am J Psychiatry. 2004;161:2717.
33. Capuron L, Ravaud A, Gualde N, Bosmans E, Dantzer R, Maes M, et al.
Association between immune activation and early depressive symptoms
in cancer patients treated with interleukin-2-based therapy.
Psychoneuroendocrinology. 2001;26:797808.
34. Capuron L, Miller AH. Cytokines and psychopathology: lessons from
interferon-alpha. Biol Psychiatry. 2004;56:81924.
35. Strik JJ, Honig A, Lousberg R, Denollet J. Sensitivity and specificity of observer
and self-report questionnaires in major and minor depression following
myocardial infarction. Psychosomatics. 2001;42:4238.
36. Otte C, Zhao S, Whooley MA. Statin use and risk of depression in patients
with coronary heart disease: longitudinal data from the heart and soul
study. J Clin Psychiatry. 2012;73:6105.
37. Bonnet J, McPherson R, Tedgui A, Simoneau D, Nozza A, Martineau P, et al.
Comparative effects of 10-mg versus 80-mg Atorvastatin on high-sensitivity
C-reactive protein in patients with stable coronary artery disease: results of
the CAP (Comparative Atorvastatin Pleiotropic effects) study. Clin Ther.
2008;30:2298313.
38. Lichtman JH, Bigger Jr JT, Blumenthal JA, Frasure-Smith N, Kaufmann PG,
Lesperance F, et al. Depression and coronary heart disease: recommendations
for screening, referral, and treatment: a science advisory from the American
Heart Association Prevention Committee of the Council on Cardiovascular
Nursing, Council on Clinical Cardiology, Council on Epidemiology and
Prevention, and Interdisciplinary Council on Quality of Care and Outcomes
Research: endorsed by the American Psychiatric Association. Circulation.
2008;118:176875.
39. Ziegelstein RC, Thombs BD, Coyne JC, de Jonge P. Routine screening for
depression in patients with coronary heart disease never mind. J Am Coll
Cardiol. 2009;54:88690.
40. National Institute for Health and Clinical Excellence: Guidance. National
Collaborating Centre for Mental Health (UK).: Depression: The Treatment
and Management of Depression in Adults (Updated Edition). 2010.
Submit your next manuscript to BioMed Central
and take full advantage of:
Convenient online submission
Thorough peer review
No space constraints or color gure charges
Immediate publication on acceptance
Inclusion in PubMed, CAS, Scopus and Google Scholar
Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
You might also like
- Aerobic Exercise in Several Mental Illness - Requirement From The Perspective of Sports MedicineNo ratings yetAerobic Exercise in Several Mental Illness - Requirement From The Perspective of Sports Medicine36 pages
- Depression and 18-Month Prognosis After Myocardial InfarctionNo ratings yetDepression and 18-Month Prognosis After Myocardial Infarction12 pages
- Depression and Cardiovascular Disease: A Clinical ReviewNo ratings yetDepression and Cardiovascular Disease: A Clinical Review11 pages
- Comorbid Depression in Medical DiseasesNo ratings yetComorbid Depression in Medical Diseases22 pages
- The Impact of Personality Factors On Delay in Seeking Treatment of Acute Myocardial InfarctionNo ratings yetThe Impact of Personality Factors On Delay in Seeking Treatment of Acute Myocardial Infarction7 pages
- Characteristics of Depression in Hemodialysis Patients: Symptoms, Quality of Life and Mortality RiskNo ratings yetCharacteristics of Depression in Hemodialysis Patients: Symptoms, Quality of Life and Mortality Risk7 pages
- Depression and Cardiovascular Disease A ClinicalNo ratings yetDepression and Cardiovascular Disease A Clinical11 pages
- Research Article: The Effect of Antidepressants On The Course of Inflammatory Bowel DiseaseNo ratings yetResearch Article: The Effect of Antidepressants On The Course of Inflammatory Bowel Disease11 pages
- Associations between biomarkers of inflammation and depressive symptoms—potential differences between diabetes types and symptom clusters of depression - Translational Psychiatry - 11.01.2025No ratings yetAssociations between biomarkers of inflammation and depressive symptoms—potential differences between diabetes types and symptom clusters of depression - Translational Psychiatry - 11.01.20259 pages
- Persistent Depressive Disorder Across The Adult Lifespan: Results From Clinical and Population-Based Surveys in GermanyNo ratings yetPersistent Depressive Disorder Across The Adult Lifespan: Results From Clinical and Population-Based Surveys in Germany13 pages
- Crump2016 Article StressResilienceAndSubsequentRNo ratings yetCrump2016 Article StressResilienceAndSubsequentR6 pages
- 2015 - State of The Art Review - Depression, Stress, Anxiety and Cardiovascular DiseaseNo ratings yet2015 - State of The Art Review - Depression, Stress, Anxiety and Cardiovascular Disease8 pages
- Weight change and risk of depression in DKDNo ratings yetWeight change and risk of depression in DKD12 pages
- Association of Comorbid Mental Disorders With Cardiovascula - 2022 - General HosNo ratings yetAssociation of Comorbid Mental Disorders With Cardiovascula - 2022 - General Hos9 pages
- A Risk Prediction Model For Heart Failure Hospitalization JuroanlNo ratings yetA Risk Prediction Model For Heart Failure Hospitalization Juroanl20 pages
- Longitudinal Observation of Anxiety and Depression Among Palliative Care Cancer PatientsNo ratings yetLongitudinal Observation of Anxiety and Depression Among Palliative Care Cancer Patients14 pages
- The Association Between Major Depressive Disorder and Outcomes in Older Veterans Hospitalized With Pneumonia PDFNo ratings yetThe Association Between Major Depressive Disorder and Outcomes in Older Veterans Hospitalized With Pneumonia PDF6 pages
- Anxiety and Cardiovascular Disease Risk A ReviewNo ratings yetAnxiety and Cardiovascular Disease Risk A Review8 pages
- Association Between Comorbid Anxiety Diabetes Control and Overall Medical Burden in Population With Serious Mental Illness and DiabetesNo ratings yetAssociation Between Comorbid Anxiety Diabetes Control and Overall Medical Burden in Population With Serious Mental Illness and Diabetes12 pages
- IndianJEndocrMetab Diabetes y Trastornos MentalesNo ratings yetIndianJEndocrMetab Diabetes y Trastornos Mentales4 pages
- Cardiovascular Risk Assessment and Screening in Diabetes: Yanglu ZhaoNo ratings yetCardiovascular Risk Assessment and Screening in Diabetes: Yanglu Zhao6 pages
- Disability Worsening Among Persons With Multiple Sclerosis and DepressionNo ratings yetDisability Worsening Among Persons With Multiple Sclerosis and Depression9 pages
- Rosenblat2015 Disfunción Inmune BipolarNo ratings yetRosenblat2015 Disfunción Inmune Bipolar12 pages
- Clinical Features and Diagnosis of Myalgic Encephalomyelitis - Chronic Fatigue Syndrome - UpToDateNo ratings yetClinical Features and Diagnosis of Myalgic Encephalomyelitis - Chronic Fatigue Syndrome - UpToDate23 pages
- Depression in Cancer Patients: Pathogenesis, Implications and Treatment (Review)No ratings yetDepression in Cancer Patients: Pathogenesis, Implications and Treatment (Review)6 pages
- Is There Time For Management of Patients With Chronic Diseases in Primary Care?No ratings yetIs There Time For Management of Patients With Chronic Diseases in Primary Care?6 pages
- Risk Factors For Post-Stroke Depression in Sohag University HospitalNo ratings yetRisk Factors For Post-Stroke Depression in Sohag University Hospital5 pages
- JPTC Exploring The Connection Between Chronic Stress and Cardiovascular Diseases Insights From The Mediterranean DietNo ratings yetJPTC Exploring The Connection Between Chronic Stress and Cardiovascular Diseases Insights From The Mediterranean Diet6 pages
- Predictors Psychological Distress Among Post Operative Cardiac SurgeryNo ratings yetPredictors Psychological Distress Among Post Operative Cardiac Surgery21 pages
- Health and Quality of Life Outcomes Impairment of Quality of Life in Type 2 Diabetes Mellitus: A Cross-Sectional StudyNo ratings yetHealth and Quality of Life Outcomes Impairment of Quality of Life in Type 2 Diabetes Mellitus: A Cross-Sectional Study7 pages
- Factors Associated With Post-Stroke Depression and Fatigue: Lesion Location and Coping StylesNo ratings yetFactors Associated With Post-Stroke Depression and Fatigue: Lesion Location and Coping Styles8 pages
- Improvement in Quality of Life of Chinese Chronic.68No ratings yetImprovement in Quality of Life of Chinese Chronic.685 pages
- Anxiety and depression in patients with end-stage renal disease (1)No ratings yetAnxiety and depression in patients with end-stage renal disease (1)10 pages
- Poststroke Depression: Prevalence and Determinants in Brazilian Stroke PatientsNo ratings yetPoststroke Depression: Prevalence and Determinants in Brazilian Stroke Patients10 pages
- Etiología Comorbilidad Depresión y ECVNo ratings yetEtiología Comorbilidad Depresión y ECV26 pages
- Studyprotocol Open Access: Gian Mauro Manzoni, Gianluca Castelnuovo and Enrico MolinariNo ratings yetStudyprotocol Open Access: Gian Mauro Manzoni, Gianluca Castelnuovo and Enrico Molinari8 pages
- Patients With Cancer - Overview of The Clinical Features and Diagnosis of Psychiatric Disorders - UpToDateNo ratings yetPatients With Cancer - Overview of The Clinical Features and Diagnosis of Psychiatric Disorders - UpToDate36 pages
- AP Biology Lab Ten: Physiology of The Circulatory System75% (4)AP Biology Lab Ten: Physiology of The Circulatory System8 pages
- Nursing Care Plan (NCP) For SchizophreniformNo ratings yetNursing Care Plan (NCP) For Schizophreniform8 pages
- Medicinal Plants in The Treatment of Arthritis: A. Subramoniam, V. Madhavachandran and A. GangaprasadNo ratings yetMedicinal Plants in The Treatment of Arthritis: A. Subramoniam, V. Madhavachandran and A. Gangaprasad35 pages
- Aerosolized Antibiotics and Ventilator-Associated Tracheobronchitis in The Intensive Care UnitNo ratings yetAerosolized Antibiotics and Ventilator-Associated Tracheobronchitis in The Intensive Care Unit6 pages
- MENTAL HEALTH AND MENTAL DISORDERS WordNo ratings yetMENTAL HEALTH AND MENTAL DISORDERS Word12 pages
- Suspension Trauma Orthostatic Intolerance OSHANo ratings yetSuspension Trauma Orthostatic Intolerance OSHA4 pages
- The Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyNo ratings yetThe Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled Study8 pages
























































































- Aerobic Exercise in Several Mental Illness - Requirement From The Perspective of Sports MedicineAerobic Exercise in Several Mental Illness - Requirement From The Perspective of Sports Medicine
- Depression and 18-Month Prognosis After Myocardial InfarctionDepression and 18-Month Prognosis After Myocardial Infarction
- Depression and Cardiovascular Disease: A Clinical ReviewDepression and Cardiovascular Disease: A Clinical Review
- The Impact of Personality Factors On Delay in Seeking Treatment of Acute Myocardial InfarctionThe Impact of Personality Factors On Delay in Seeking Treatment of Acute Myocardial Infarction
- Characteristics of Depression in Hemodialysis Patients: Symptoms, Quality of Life and Mortality RiskCharacteristics of Depression in Hemodialysis Patients: Symptoms, Quality of Life and Mortality Risk
- Research Article: The Effect of Antidepressants On The Course of Inflammatory Bowel DiseaseResearch Article: The Effect of Antidepressants On The Course of Inflammatory Bowel Disease
- Associations between biomarkers of inflammation and depressive symptoms—potential differences between diabetes types and symptom clusters of depression - Translational Psychiatry - 11.01.2025Associations between biomarkers of inflammation and depressive symptoms—potential differences between diabetes types and symptom clusters of depression - Translational Psychiatry - 11.01.2025
- Persistent Depressive Disorder Across The Adult Lifespan: Results From Clinical and Population-Based Surveys in GermanyPersistent Depressive Disorder Across The Adult Lifespan: Results From Clinical and Population-Based Surveys in Germany
- 2015 - State of The Art Review - Depression, Stress, Anxiety and Cardiovascular Disease2015 - State of The Art Review - Depression, Stress, Anxiety and Cardiovascular Disease
- Association of Comorbid Mental Disorders With Cardiovascula - 2022 - General HosAssociation of Comorbid Mental Disorders With Cardiovascula - 2022 - General Hos
- A Risk Prediction Model For Heart Failure Hospitalization JuroanlA Risk Prediction Model For Heart Failure Hospitalization Juroanl
- Longitudinal Observation of Anxiety and Depression Among Palliative Care Cancer PatientsLongitudinal Observation of Anxiety and Depression Among Palliative Care Cancer Patients
- The Association Between Major Depressive Disorder and Outcomes in Older Veterans Hospitalized With Pneumonia PDFThe Association Between Major Depressive Disorder and Outcomes in Older Veterans Hospitalized With Pneumonia PDF
- Association Between Comorbid Anxiety Diabetes Control and Overall Medical Burden in Population With Serious Mental Illness and DiabetesAssociation Between Comorbid Anxiety Diabetes Control and Overall Medical Burden in Population With Serious Mental Illness and Diabetes
- Cardiovascular Risk Assessment and Screening in Diabetes: Yanglu ZhaoCardiovascular Risk Assessment and Screening in Diabetes: Yanglu Zhao
- Disability Worsening Among Persons With Multiple Sclerosis and DepressionDisability Worsening Among Persons With Multiple Sclerosis and Depression
- Clinical Features and Diagnosis of Myalgic Encephalomyelitis - Chronic Fatigue Syndrome - UpToDateClinical Features and Diagnosis of Myalgic Encephalomyelitis - Chronic Fatigue Syndrome - UpToDate
- Depression in Cancer Patients: Pathogenesis, Implications and Treatment (Review)Depression in Cancer Patients: Pathogenesis, Implications and Treatment (Review)
- Is There Time For Management of Patients With Chronic Diseases in Primary Care?Is There Time For Management of Patients With Chronic Diseases in Primary Care?
- Risk Factors For Post-Stroke Depression in Sohag University HospitalRisk Factors For Post-Stroke Depression in Sohag University Hospital
- JPTC Exploring The Connection Between Chronic Stress and Cardiovascular Diseases Insights From The Mediterranean DietJPTC Exploring The Connection Between Chronic Stress and Cardiovascular Diseases Insights From The Mediterranean Diet
- Predictors Psychological Distress Among Post Operative Cardiac SurgeryPredictors Psychological Distress Among Post Operative Cardiac Surgery
- Health and Quality of Life Outcomes Impairment of Quality of Life in Type 2 Diabetes Mellitus: A Cross-Sectional StudyHealth and Quality of Life Outcomes Impairment of Quality of Life in Type 2 Diabetes Mellitus: A Cross-Sectional Study
- Factors Associated With Post-Stroke Depression and Fatigue: Lesion Location and Coping StylesFactors Associated With Post-Stroke Depression and Fatigue: Lesion Location and Coping Styles
- Improvement in Quality of Life of Chinese Chronic.68Improvement in Quality of Life of Chinese Chronic.68
- Anxiety and depression in patients with end-stage renal disease (1)Anxiety and depression in patients with end-stage renal disease (1)
- Poststroke Depression: Prevalence and Determinants in Brazilian Stroke PatientsPoststroke Depression: Prevalence and Determinants in Brazilian Stroke Patients
- Studyprotocol Open Access: Gian Mauro Manzoni, Gianluca Castelnuovo and Enrico MolinariStudyprotocol Open Access: Gian Mauro Manzoni, Gianluca Castelnuovo and Enrico Molinari
- Patients With Cancer - Overview of The Clinical Features and Diagnosis of Psychiatric Disorders - UpToDatePatients With Cancer - Overview of The Clinical Features and Diagnosis of Psychiatric Disorders - UpToDate
- Multiple Sclerosis And You: Tame This DiseaseFrom EverandMultiple Sclerosis And You: Tame This Disease
- AP Biology Lab Ten: Physiology of The Circulatory SystemAP Biology Lab Ten: Physiology of The Circulatory System
- Medicinal Plants in The Treatment of Arthritis: A. Subramoniam, V. Madhavachandran and A. GangaprasadMedicinal Plants in The Treatment of Arthritis: A. Subramoniam, V. Madhavachandran and A. Gangaprasad
- Aerosolized Antibiotics and Ventilator-Associated Tracheobronchitis in The Intensive Care UnitAerosolized Antibiotics and Ventilator-Associated Tracheobronchitis in The Intensive Care Unit
- The Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyThe Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled Study