MSDS Asparginase
MSDS Asparginase
Download as pdf or txt
You might also like
- BLS Instructor Candidate WorkbookDocument34 pagesBLS Instructor Candidate WorkbookKristaMaeC.LazoNo ratings yet
- EW Smooth Muscle ProtocolDocument11 pagesEW Smooth Muscle ProtocolSoledad Vega Delgado0% (1)
- Michael Jai White PDFDocument7 pagesMichael Jai White PDFFrank Ramírez ParedesNo ratings yet
- Elspar Dosage Info DB00023Document8 pagesElspar Dosage Info DB00023vedi786No ratings yet
- Blood 2014Document9 pagesBlood 2014cdsaludNo ratings yet
- 3 - Erwinia Asparaginase - Drug Information - UpToDateDocument14 pages3 - Erwinia Asparaginase - Drug Information - UpToDateKellyKKSNo ratings yet
- Tugas Farmakologi ToksikologiDocument55 pagesTugas Farmakologi ToksikologilucyanaNo ratings yet
- Leunase InjDocument14 pagesLeunase InjLiaWahyuniNo ratings yet
- Ind. Sem. - ALL OncasparDocument40 pagesInd. Sem. - ALL OncasparBrianhernzNo ratings yet
- Buffered Aspirin ProductsDocument7 pagesBuffered Aspirin ProductsKimsha ConcepcionNo ratings yet
- Asparaginase Toxicity PDFDocument10 pagesAsparaginase Toxicity PDFyakanismNo ratings yet
- Asparaginase therapy in patients with acute lymphoblastic leukemia expert opinion on use and toxicity managementDocument13 pagesAsparaginase therapy in patients with acute lymphoblastic leukemia expert opinion on use and toxicity managementXue-ping HanNo ratings yet
- Avifavir LabelDocument5 pagesAvifavir LabelChristian PuenteNo ratings yet
- Review STDDocument6 pagesReview STDDr Anand VibhuteNo ratings yet
- S 022 LBLDocument4 pagesS 022 LBLkutafoaklilu5No ratings yet
- Bookshelf_NBK1159Document20 pagesBookshelf_NBK1159giovanaribeiro.driveNo ratings yet
- AGALSIDASE ALFA 1 MG-ML (Replagal Solution For Injection)Document10 pagesAGALSIDASE ALFA 1 MG-ML (Replagal Solution For Injection)ddandan_2No ratings yet
- Dacarbazine Monograph 1june2013 FormattedDocument7 pagesDacarbazine Monograph 1june2013 FormattedRobert ChristevenNo ratings yet
- S 017 LBLDocument4 pagesS 017 LBLsanjaykv981No ratings yet
- New Oral Anticoagulants For Stroke Prevention in Atrial FibrillationDocument1 pageNew Oral Anticoagulants For Stroke Prevention in Atrial FibrillationmngalaxyNo ratings yet
- CirrosisDocument8 pagesCirrosisMauricio Lopez MejiaNo ratings yet
- Enalapril MaleateDocument4 pagesEnalapril Maleatetaner_soysurenNo ratings yet
- Areviewofacetaminophen Poisoning: Michael J. Hodgman,, Alexander R. GarrardDocument18 pagesAreviewofacetaminophen Poisoning: Michael J. Hodgman,, Alexander R. Garrardأحمد علي حبيبNo ratings yet
- Refero - Rifaximina 550mgDocument13 pagesRefero - Rifaximina 550mgJosé Rui SoaresNo ratings yet
- JPP-7-62Document10 pagesJPP-7-62Xue-ping HanNo ratings yet
- CARMABAZEPINE (Bauer)Document5 pagesCARMABAZEPINE (Bauer)Ela chawNo ratings yet
- Buy Xanax (Alprazolam) OnlineDocument26 pagesBuy Xanax (Alprazolam) OnlineBuy Xanax online at chemworldstore.netNo ratings yet
- Full Prescribing Information: Contents : Reference ID: 4533779Document14 pagesFull Prescribing Information: Contents : Reference ID: 4533779vbx963No ratings yet
- Pieters 2010Document12 pagesPieters 2010Agniya Ali FahmiNo ratings yet
- Acarbose: Drug Information: Brand Names: USDocument9 pagesAcarbose: Drug Information: Brand Names: USAnonymous wmF9p2ejNo ratings yet
- Analgesic: Mefenamic AcidDocument5 pagesAnalgesic: Mefenamic Acidmegazhang94No ratings yet
- Saf - Eular 2019Document9 pagesSaf - Eular 2019Pablo OlivoNo ratings yet
- PRIMAQUINE PHOSPHATE-primaquine Phos Phate Tablet Bays Hore Pharmaceuticals, LLCDocument8 pagesPRIMAQUINE PHOSPHATE-primaquine Phos Phate Tablet Bays Hore Pharmaceuticals, LLCKulfi BarfiNo ratings yet
- Rafassal Caplets, Suppositories, Enemas CompositionDocument6 pagesRafassal Caplets, Suppositories, Enemas Compositionddandan_2No ratings yet
- Primaquine: Phosphate Tablets, UspDocument6 pagesPrimaquine: Phosphate Tablets, UspEphenk PunkNo ratings yet
- Deep Vein ThrombosisDocument4 pagesDeep Vein ThrombosisStefania CristinaNo ratings yet
- Group Two Presentation PharmacologyDocument29 pagesGroup Two Presentation PharmacologyShaibu AwalNo ratings yet
- PREVPAC Drug StudyDocument7 pagesPREVPAC Drug StudyAngela ReyesNo ratings yet
- Aranesp (Darbepoetin Alfa) For InjectionDocument21 pagesAranesp (Darbepoetin Alfa) For InjectionKhalil saterNo ratings yet
- Egy 1.1.2 Api Augmentin 1 GM Tabs Ipi11 1Document3 pagesEgy 1.1.2 Api Augmentin 1 GM Tabs Ipi11 1magdNo ratings yet
- In Vitro, Sucralfate Adsorbs Bile SaltsDocument5 pagesIn Vitro, Sucralfate Adsorbs Bile SaltsZarbakht AliNo ratings yet
- Napsec: Composition: IndicationsDocument1 pageNapsec: Composition: Indicationszillur1195No ratings yet
- Antineoplastico PDFDocument9 pagesAntineoplastico PDFkaren margarita pacheco castillaNo ratings yet
- New Test Guide.doc · إصدار ١Document124 pagesNew Test Guide.doc · إصدار ١ayman aghaNo ratings yet
- Antipyretics: Instiaty Tropical Infection Module 2017-2018 Dept of Pharmacology and Therapeutics FkuiDocument22 pagesAntipyretics: Instiaty Tropical Infection Module 2017-2018 Dept of Pharmacology and Therapeutics Fkuisalsa2506No ratings yet
- NapsecDocument1 pageNapseczillur1195No ratings yet
- Drug Study Arthritis DrugDocument9 pagesDrug Study Arthritis DrugIrene Grace BalcuevaNo ratings yet
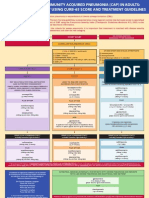
- CAP CURB-65 GuidelinesDocument1 pageCAP CURB-65 GuidelinesAndy LoakNo ratings yet
- Lamivudine: in Vitro Studies Indicate That Zidovudine-Resistant Virus Isolates Can Become ZidovudineDocument7 pagesLamivudine: in Vitro Studies Indicate That Zidovudine-Resistant Virus Isolates Can Become ZidovudineKirtikrushna Suresh Prasad OjhaNo ratings yet
- 3.E.2-Caspofungin Guideline 2003Document3 pages3.E.2-Caspofungin Guideline 2003damondouglasNo ratings yet
- Tishk International University: ApixabanDocument4 pagesTishk International University: ApixabanDyar MzafarNo ratings yet
- Plaquenil SPCDocument20 pagesPlaquenil SPCMinas ParisisNo ratings yet
- Acarbose 50 MG Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document7 pagesAcarbose 50 MG Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)GadNo ratings yet
- AcetazolamideDocument4 pagesAcetazolamideAnkit RuhilNo ratings yet
- MEFENAMIC-ACID-mefenamic Acid Caps Ule Sciele Pharma IncDocument14 pagesMEFENAMIC-ACID-mefenamic Acid Caps Ule Sciele Pharma IncIrma DamayantiNo ratings yet
- Pi Is 1548559519301661Document5 pagesPi Is 1548559519301661dhirajkishNo ratings yet
- Cablivi Epar Product Information - enDocument39 pagesCablivi Epar Product Information - enSuh TeixeiraNo ratings yet
- Alirocumab-75mg Per ML InjectionDocument8 pagesAlirocumab-75mg Per ML InjectionMd. Abdur RahmanNo ratings yet
- MEFTAL P Suspension PIDocument10 pagesMEFTAL P Suspension PIpiyush patelNo ratings yet
- ACE I ToxicityDocument6 pagesACE I ToxicityAyodele EmmanuelNo ratings yet
- Pentaspan en PMDocument14 pagesPentaspan en PMVictoria SurugiuNo ratings yet
- Product MonographDocument33 pagesProduct Monographعبدالعزيز بدرNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Final - PDM - Form - Shelter and NFIsDocument2 pagesFinal - PDM - Form - Shelter and NFIsBassam AlmadhjiNo ratings yet
- MAPEH Grade 8: Objective SDocument6 pagesMAPEH Grade 8: Objective SBonifacio LeddaNo ratings yet
- Cavity Search Produces 50 Bags of Heroin in Northeastern Pennsylvania COMMENTS ARE The BESTDocument6 pagesCavity Search Produces 50 Bags of Heroin in Northeastern Pennsylvania COMMENTS ARE The BESTKAWNo ratings yet
- HijamaDocument10 pagesHijamaGendale Am-isNo ratings yet
- E WasteDocument27 pagesE WasteSuresh Khaleri0% (1)
- Green RevolutionDocument14 pagesGreen Revolutionarunbestudent100% (1)
- Confined Space EntryDocument48 pagesConfined Space Entryadammzjin100% (2)
- NCP1300Document6 pagesNCP1300Mhaiyne EndearingNo ratings yet
- RA GL HAL PPS 404 (Dewatering)Document6 pagesRA GL HAL PPS 404 (Dewatering)BalasubramanianNo ratings yet
- Instant download Health Informatics Practical G Robert E. Hoyt pdf all chapterDocument24 pagesInstant download Health Informatics Practical G Robert E. Hoyt pdf all chapterbilottalicxt100% (2)
- ĐỀ ĐỀ XUẤT 10 2022Document20 pagesĐỀ ĐỀ XUẤT 10 2022nguyencuongphanhungNo ratings yet
- FSR 109 - Farm Hygiene Audit Questionnaire - KIRIMIDocument4 pagesFSR 109 - Farm Hygiene Audit Questionnaire - KIRIMInderijohnsonNo ratings yet
- TP 200Document852 pagesTP 200Laney SommerNo ratings yet
- MEP Brochure Movix 4 8 Dream GB BRDocument5 pagesMEP Brochure Movix 4 8 Dream GB BRRomuald Eric TefongNo ratings yet
- Homeroom Guidance: Quarter 4 - Module 17: I in The CommunityDocument14 pagesHomeroom Guidance: Quarter 4 - Module 17: I in The CommunityRj Vergara MarticioNo ratings yet
- English 8 Week 1 and 2Document10 pagesEnglish 8 Week 1 and 2Reynalyn estreraNo ratings yet
- DBL 8585 - E - 2010-09 EnglishDocument47 pagesDBL 8585 - E - 2010-09 EnglishPaul RedaiNo ratings yet
- National Ambient Air Quality StandardsDocument3 pagesNational Ambient Air Quality StandardsAji GumelarNo ratings yet
- Doctors' Rights - Health and LifestyleDocument6 pagesDoctors' Rights - Health and LifestyleJuan Rafael SilvaNo ratings yet
- Introduction To SurveillanceDocument9 pagesIntroduction To SurveillanceMuhammad ZikraNo ratings yet
- 6 SCENAR AnalgesiaDocument14 pages6 SCENAR Analgesiabetfort.christopheNo ratings yet
- Internship Report: I Hili P PR L HDocument74 pagesInternship Report: I Hili P PR L HRakibul IslamNo ratings yet
- Data Narko, Psiko, Preku, Oot, Pulv, VaksinDocument2 pagesData Narko, Psiko, Preku, Oot, Pulv, VaksinSega STTIFNo ratings yet
- SL NO Complaint # Type Date & Time Description Location StatusDocument2 pagesSL NO Complaint # Type Date & Time Description Location StatusRaziKhanNo ratings yet
- Social Competence and Social Skills - A Theoretical and Practical GuideDocument182 pagesSocial Competence and Social Skills - A Theoretical and Practical GuideMariana GaluppoNo ratings yet
- Vet Anesthesia and SedationDocument11 pagesVet Anesthesia and Sedationcgw47No ratings yet
- Facility Requirements For Biotech PlantsDocument8 pagesFacility Requirements For Biotech PlantsKhushman AsodariyaNo ratings yet