
Renal and Retinal Effects of Enalapril and Losartan in Type 1 Diabetes
Renal and Retinal Effects of Enalapril and Losartan in Type 1 Diabetes
Uploaded by
Dina Malisa Nugraha, MDCopyright:
Available Formats
Renal and Retinal Effects of Enalapril and Losartan in Type 1 Diabetes
Renal and Retinal Effects of Enalapril and Losartan in Type 1 Diabetes
Uploaded by
Dina Malisa Nugraha, MDOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Renal and Retinal Effects of Enalapril and Losartan in Type 1 Diabetes
Renal and Retinal Effects of Enalapril and Losartan in Type 1 Diabetes
Uploaded by
Dina Malisa Nugraha, MDCopyright:
Available Formats
The
n e w e ng l a n d j o u r na l
of
m e dic i n e
original article
Renal and Retinal Effects of Enalapril
and Losartan in Type 1 Diabetes
Michael Mauer, M.D., Bernard Zinman, M.D., Robert Gardiner, M.D.,
Samy Suissa, Ph.D., Alan Sinaiko, M.D., Trudy Strand, R.N.,
Keith Drummond, M.D., Sandra Donnelly, M.D., Paul Goodyer, M.D.,
Marie Claire Gubler, M.D., and Ronald Klein, M.D., M.P.H.
A BS T R AC T
Background
From the Departments of Pediatrics (M.M.,
A.S., T.S.) and Medicine (M.M.), University of Minnesota, Minneapolis; Samuel
Lunenfeld Research Institute, Mount Sinai
Hospital, University of Toronto, Toronto
(B.Z., S.D.); the Departments of Medicine
(R.G.), Epidemiology and Biostatistics
(S.S.), and Pediatrics (K.D., P.G.), McGill
University, Montreal; Hpital Necker
Enfants Malades, Paris (M.C.G.); and the
Department of Ophthalmology and Visual
Sciences, University of Wisconsin School
of Medicine and Public Health, Madison
(R.K.). Address reprint requests to Dr.
Mauer at the Department of Pediatrics,
University of Minnesota, 420 Delaware St.
SE, MMC 491, Minneapolis, MN 55455,
or at mauer002@umn.edu.
N Engl J Med 2009;361:40-51.
Copyright 2009 Massachusetts Medical Society.
Nephropathy and retinopathy remain important complications of type 1 diabetes.
It is unclear whether their progression is slowed by early administration of drugs
that block the reninangiotensin system.
Methods
We conducted a multicenter, controlled trial involving 285 normotensive patients
with type 1 diabetes and normoalbuminuria and who were randomly assigned to
receive losartan (100 mg daily), enalapril (20 mg daily), or placebo and followed for
5 years. The primary end point was a change in the fraction of glomerular volume
occupied by mesangium in kidney-biopsy specimens. The retinopathy end point was
a progression on a retinopathy severity scale of two steps or more. Intention-to-treat
analysis was performed with the use of linear regression and logistic-regression
models.
Results
A total of 90% and 82% of patients had complete renal-biopsy and retinopathy data,
respectively. Change in mesangial fractional volume per glomerulus over the 5-year
period did not differ significantly between the placebo group (0.016 units) and the
enalapril group (0.005, P=0.38) or the losartan group (0.026, P=0.26), nor were
there significant treatment benefits for other biopsy-assessed renal structural variables. The 5-year cumulative incidence of microalbuminuria was 6% in the placebo
group; the incidence was higher with losartan (17%, P=0.01 by the log-rank test)
but not with enalapril (4%, P=0.96 by the log-rank test). As compared with placebo,
the odds of retinopathy progression by two steps or more was reduced by 65% with
enalapril (odds ratio, 0.35; 95% confidence interval [CI], 0.14 to 0.85) and by 70%
with losartan (odds ratio, 0.30; 95% CI, 0.12 to 0.73), independently of changes in
blood pressure. There were three biopsy-related serious adverse events that completely resolved. Chronic cough occurred in 12 patients receiving enalapril, 6 receiving losartan, and 4 receiving placebo.
Conclusions
Early blockade of the reninangiotensin system in patients with type 1 diabetes
did not slow nephropathy progression but slowed the progression of retinopathy.
(ClinicalTrials.gov number, NCT00143949.)
40
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
Enalapril and Losartan in Type 1 Diabetes
iabetic nephropathy, responsible
for more than 45% of cases of end-stage
renal disease in the United States,1 may be
structurally advanced once albuminuria becomes
detectable.2,3 Blockers of the reninangiotensin
system are more effective than other antihypertensive agents in slowing nephropathy progression in patients who have proteinuria, diabetes
mellitus, and a reduced glomerular filtration rate
(GFR),4-6 and such blockers can also decrease
proteinuria in patients with diabetes.7 Although
the reduction of proteinuria in patients with diabetes has been associated with a reduction in the
rate of decline in GFR in small studies,8 this association has not been systematically tested; in
addition, proteinuria reduction is not a generally
accepted surrogate for hard clinical end points
such as end-stage renal disease.9 Intensive multifactorial intervention in patients with type 2 diabetes with microalbuminuria nearly halved the
progression of proteinuria but did not alter the
rate of GFR decline.10,11
In the ReninAngiotensin System Study (RASS),
we asked whether blockade of the reninangiotensin system before the onset of albuminuria in
patients with type 1 diabetes could slow progression of the early histologic lesions of diabetic
nephropathy. RASS was based on the concept
that slowing the structural changes responsible
for renal dysfunction in diabetes2,3 would delay
or prevent clinical diabetic nephropathy.
Recently, the Diabetic Retinopathy Candesartan Trials (DIRECT; ClinicalTrials.gov numbers,
NCT00252733, NCT00252720, and NCT00252694)
reported that angiotensin-receptor blockade reduced the rate of retinopathy development in
normotensive patients with type 1 diabetes and
normoalbuminuria who did not have diabetic
retinopathy12 but not in patients with mild-tomoderate diabetic retinopathy. Our study was designed to assess the effect of reninangiotensin
system blockade with either an angiotensin-convertingenzyme (ACE) inhibitor or an angiotensinreceptor blocker (ARB) on both renal and retinal
morphologic features in normotensive patients
with type 1 diabetes and normoalbuminuria.13
Me thods
The authors designed the study, wrote and made
the decision to submit the manuscript for publication, and vouch for the completeness, accuracy,
and integrity of the data and data analyses. Data
gathered at the three study centers were forwarded to the data center based at McGill University,
where all analyses were done under an authors
supervision. There were no confidentiality agreements between the authors or their institutions
and the sponsors (Merck [United States] and Merck
Frosst [Canada]), who provided partial support for
this study and donated the study drugs, nor did
these sponsors have any role in the study design,
data accrual, data analysis, or manuscript preparation. The study was approved by the relevant institutional review boards, and written informed consent was obtained from each participant. The
study was overseen by a data and safety monitoring board of the National Institutes of Health.
Study Design
RASS13 was a 5-year, multicenter, randomized,
double-blind, placebo-controlled investigator-initiated trial comparing effects of the ACE inhibitor
enalapril (Vasotec, Merck) and the ARB losartan
(Cozaar, Merck) with those of placebo on early
renal structural changes from diabetic nephropathy in type 1 diabetes. The prespecified primary
study end point was a change in the fraction of
glomerular volume occupied by mesangium (the
mesangial fractional volume).2,14 Secondary renal
end points included changes in other glomerular,
vascular, tubular, and interstitial variables and
changes in the albumin excretion rate and GFR.
Shortly after RASS began, we added a study with
an a priori end point of a progression of diabetic
retinopathy of two steps or more.13 Patients were
randomly assigned to one of three groups with
the use of computer-generated blocks of six and
stratified according to center and sex: those receiving enalapril, 10 mg daily; losartan, 50 mg daily;
or daily placebo. During the study, doses were
doubled because of new data indicating greater
reduction in proteinuria with higher doses.15 Patients received the doubled dose of the study drugs
for an average of 2.90.9 years.
Study Patients
Exclusion criteria were hypertension (blood pressure exceeding 135/85 mm Hg or receipt of antihypertensive medications), an albumin excretion
rate above 20 g per minute, pregnancy, failure to
take at least 85% of placebo pills during a 2-week
run-in period, and a GFR of less than 90 ml per
minute per 1.73 m2 of body-surface area (<80 ml
per minute if the patient had a strictly vegan
diet).16 Patients for whom fundus photographs
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
41
The
n e w e ng l a n d j o u r na l
of
m e dic i n e
were taken at baseline (within 1 year after randomization) and who did not have proliferative
diabetic retinopathy were included in the diabetic
retinopathy studies.
The duration of type 1 diabetes among the
study patients ranged from 2 to 20 years. Patients
18 years of age or older were recruited from diabetes clinics and by means of local advertising;
the Minnesota and Montreal centers also enrolled
32 patients (11% of the total 285 patients enrolled) who were 15 to 17 years of age, from the
Natural History of Diabetic Nephropathy Study.17
Of the 1065 patients with type 1 diabetes screened,
707 declined to participate, 73 were ineligible,
and 285 were randomly assigned to one of the
three study groups (Fig. 1). There were no demographic differences between the patients who
agreed to participate and those who declined (see
Table 1 in the Supplementary Appendix, available
with the full text of this article at NEJM.org).13
Study drugs were withheld during 18 pregnancies
in 14 patients (with 6 pregnancies in 5 patients receiving placebo, 4 pregnancies in 4 receiving enalapril, and 8 pregnancies in 5 receiving losartan).
Glycated hemoglobin was measured with the
use of a Diamat analyzer (BioRad) until 2002,
when the Tosoh method was introduced (Tosoh
Medics). Blood pressure was measured by means
of a Dinamap monitor. If hypertension persist
ed for 2 weeks, medication that does not block
the reninangiotensin system was initiated to
achieve a blood-pressure target of less than
130/80 mm Hg.
The GFR was measured according to the iohexol plasma disappearance method.18 The baseline albumin excretion rate was expressed as the
median of three samples obtained before randomization.13 Microalbuminuria was defined as
the mean of at least two of three consecutive
values between 20 and 200 g per minute.
Follow-up Measures
Renal Biopsy and Morphometric Measurements
Patients were followed for 5 years. Pill counts and
measurements of blood pressure, albumin excretion rate, and glycated hemoglobin level were obtained quarterly; GFR was assessed annually.13
Percutaneous biopsy19 was performed before randomization and 5 years later. The presence of at
least two glomeruli, for purposes of electron microscopy, was required for randomization. One
1065 Patients were screened
707 Declined to participate
73 Were not eligible
285 Underwent randomization
32 Were excluded from retinopathy
study
4 Had baseline proliferative
diabetic retinopathy
28 Had no baseline photographs
30 Had no 5-year photographs
3 Died
20 Declined to participate
or were lost to follow-up
7 Had scheduling problems
29 Had no exit biopsy
3 Died
23 Declined to participate
or were lost to follow-up
2 Had biopsy safety contraindications
1 Had inadequate tissue
in biopsy specimens
223 Patients were analyzed for
retinopathy outcome
74 Were assigned to placebo
77 Were assigned to enalapril
72 Were assigned to losartan
256 Patients were analyzed for
biopsy outcome
85 Were assigned to placebo
86 Were assigned to enalapril
85 Were assigned to losartan
Figure 1. Enrollment, Randomization, and Follow-up of the Study Patients.
42
n engl j med 361;1 nejm.org july 2, 2009
RETAKE
AUTHOR: Mauer
REG F FIGURE: 1 of 2
ICM
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009
CASE
ARTIST: ts
Line
H/T
1st
2nd
3rd
Massachusetts Medical
Revised
4-C
H/T
SIZE
Society. All rights reserved.
Enalapril and Losartan in Type 1 Diabetes
baseline biopsy and three 5-year biopsies were
repeated because of inadequate tissue; one patient had inadequate tissue twice. Five 5-year biopsy specimens had fixation problems; biopsy
was repeated for four of these. Electron microscopy was performed on 3.140.53 glomeruli per
biopsy (range, 1 through 6; only one biopsy contained just a single glomerulus). All measurements
were performed by one observer, who was unaware of the study-drug assignments. Mesangial
fractional volumes per glomerulus were estimated by means of point counting, as reported
elsewhere.3,19,20 The surface area of peripheral
glomerular basement membrane per glomerulus
and the width of glomerular basement membrane were estimated as previously described.3,19
Two observers who were unaware of the studydrug assignments estimated the fraction of each
cortical arteriolar wall that was replaced by hyaline, on random light-microscopy slides, and the
index of arteriolar hyalinosis was calculated.21
The fraction of the volume of the cortex that was
interstitium and the fraction of the volume of the
cortical tubules that were atrophic were estimated
by means of point counting22 by one observer who
was unaware of the study-drug assignments.
Grading of Retinopathy
Stereoscopic fundus photographs were taken at
30 degrees for seven standard Early Treatment
Diabetic Retinopathy Study (ETDRS) fields,23 at
baseline and 5 years. These were graded by observers, unaware of the study-drug assignments,
at the University of Wisconsin Ocular Epidemiology Reading Center who used the modified Airlie
House Classification and the ETDRS severity
scale24 (see the Supplementary Appendix). For each
eye, the maximum grade in any of the standard
fields for each lesion was used in classifying the
severity of diabetic retinopathy (see the Supplementary Appendix).19 If the severity of diabetic retinopathy in an eye could not be graded (as in three
instances), the eye was assigned the same grade
as the other eye. The diabetic retinopathy grade
was derived by concatenating the grades of the
two eyes of a patient, with the eye with the
higher grade given greater weight. This provided
a 15-step diabetic retinopathy severity scale.19,23
The primary and secondary analyses reflected an
increase on this scale of two or three steps or
more, respectively both clinically meaningful
amounts of diabetic retinopathy progression.25
Statistical Analysis
Baseline characteristics were compared with the
use of chi-square tests and analysis of variance.
Glycated hemoglobin levels and clinic blood pressures during the 5-year follow-up period were
compared by means of analysis of variance.
The difference between the 5-year and baseline values of the prespecified primary study end
point, mesangial fractional volume, was used to
compute change over time. Mean changes between the enalapril or losartan group and the
placebo group were first compared by simple linear regression. Multiple linear regression analyses
accounted for the baseline mesangial fractional
volume, duration of type 1 diabetes, age at diabetes onset, sex, glycated hemoglobin level, systol
ic blood pressure, diastolic blood pressure, GFR,
and albumin excretion rate as covariates. Such
analyses, used to improve precision of the estimates, were the prespecified approach to analysis. They were also used to assess all secondary
structural outcomes.13
For the secondary outcomes related to albumin excretion rate and GFR, the value at the time
of the 5-year biopsy and the mean of all values
over the 5-year period were analyzed with the use
of multiple linear regression, with the baseline
value of each end point as the only covariate. The
KaplanMeier approach and the log-rank test
were used to estimate and compare the cumulative incidences of microalbuminuria.
Logistic-regression analysis was used to estimate the odds ratios of the secondary outcomes
of diabetic retinopathy progression by two or three
steps or more. Odds ratios were estimated separately for the losartan and enalapril groups, relative to the placebo group, and were adjusted for
baseline characteristics, center, and baseline grade
of diabetic retinopathy according to the 15-step
severity scale. To assess the independent effect
of blood pressure, we used blood-pressure measurements during the 5-year period as a post hoc
predictor of the odds of having a progression of
diabetic nephropathy by two steps or more or by
three steps or more, after adjustment for age,
sex, and center. Study group was added to the
model to quantify the change in the odds ratio
in association with blood pressure.
A sensitivity analysis was performed for the
primary renal and the diabetic retinopathy end
points, with the use of multiple imputation techniques to assess effects of patients excluded for
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
43
The
n e w e ng l a n d j o u r na l
Table 1. Baseline Characteristics of All 285 Patients, According to Study Group.*
Characteristic
Enalapril
(N=94)
Losartan
(N=96)
Placebo
(N=95)
Age (yr)
30.610.0
29.310.2
29.19.1
Diabetes duration (yr)
11.74.9
10.74.8
11.24.5
BMI
25.63.4
26.14.0
25.43.7
Male sex (%)
48
46
45
White race (%)
98
96
100
8.61.6
8.71.7
8.31.4
Systolic
12013
12011
11911
Diastolic
718
708
708
5.1
5.5
4.8
12920
13118
12622
Glycated hemoglobin (%)
Blood pressure (mm Hg)
Median albumin excretion rate
(g/min)
Glomerular filtration rate
(ml/min/1.73 m2 of
body-surface area)
* Plusminus values are means SD. GFR denotes glomerular filtration rate.
The body-mass index (BMI) is the weight in kilograms divided by the square
of the height in meters.
Race was self-reported.
not having both the baseline and 5-year biopsy
data or diabetic retinopathy grades, respectively.
Assessment of the effect of doubling the dose
during the study was performed by adding a term
in the multiple regression analysis for the time
from randomization to dose doubling, as well as
for the time from randomization to the first
fundus photography, the latter only for diabetic
retinopathy analyses.
We calculated that a sample size of 86 patients
per group would be required for the study to have
a statistical power of 80% to detect a 50% reduction in the change in mesangial fractional volume
over the 5-year period, with a significance level
of 5% that was reduced to 2.5% to allow for the
two contrasts of the primary analysis (losartan vs.
placebo and enalapril vs. placebo).13 The samplesize calculation was based on available data from
21 patients meeting the studys entry criteria, in
whom the mean change in mesangial fractional
volume per glomerulus over the 5-year period was
0.0533 and the standard deviation was 0.0557
after regression on the baseline values of mesangial fractional volume, GFR, albumin excretion
rate, and diabetes duration. In anticipation of a
10% dropout rate, we enrolled 95 patients per
group. Data were entered at the data center based
44
of
m e dic i n e
at McGill University, managed with the use of
Paradox software, and analyzed with SAS software (version 9.1), with investigators and participants kept unaware of the results until the final
analyses were completed.
R e sult s
Of the 285 patients who underwent randomization, 256 (90%) had renal biopsy completed at
both baseline and 5 years (Fig. 1). There were no
differences in baseline characteristics between the
three groups (Table 1) among the patients who
had data from both biopsies (Table 2 in the Supplementary Appendix), or between those with and
those without data from both biopsies (Table 3 in
the Supplementary Appendix). The overall rate of
medication adherence was approximately 85%,
and the overall rate of visit attendance exceeded
93%, with both rates being similar across all three
groups (P=0.87 and P=0.92, respectively).
The three study groups had similar glycated
hemoglobin levels (P=0.54) (Fig. 1 in the Supplementary Appendix) and insulin doses (P=0.29)
during the 5-year period. The clinic-obtained systolic and diastolic blood pressures (mean SD)
during the study were lower in the enalapril group
(1139/666 mm Hg) and the losartan group
(1158/666 mm Hg) than in the placebo group
(1178/685 mm Hg) (P<0.001 for the two systolic
and P0.02 for the two diastolic comparisons,
respectively). (See Table 4 in the Supplementary
Appendix for further details on blood pressure.)
Hypertension developed in nine patients in the
placebo group, three in the enalapril group, and
four in the losartan group (P=0.04).
The prespecified primary study end point,
change in mesangial fractional volume between
baseline and 5 years, increased by 0.016 units in
the placebo group (P=0.004) and 0.026 units in
the losartan group (P<0.001) but did not change
significantly (0.005 units) in the enalapril group
(Table 2). The change associated with placebo
was not significantly different from that with either enalapril (P=0.16) or losartan (P=0.17). Nor
did the findings change after inclusion of the time
to the doubling of the study drug and after the
use of multiple imputation to account for patients
with missing second biopsy specimens. The results
for secondary renal structural end points were
generally similar (Table 5 in the Supplementary
Appendix).
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
Enalapril and Losartan in Type 1 Diabetes
Table 2. Effects of Enalapril and Losartan on Change in the Mesangial Fractional Volume, Albumin Excretion Rate,
and Glomerular Filtration Rate, According to Study Group.*
End Point
Enalapril
Losartan
Placebo
Mean at baseline
0.2010.044
0.1890.041
0.1870.045
Mean change at 5 yr
0.0050.050
0.0260.054
0.0160.048
0.011
0.010
0 (reference)
0.16
0.17
Mesangial fractional volume
Change vs. placebo
Mean difference
P value
Adjusted change vs. placebo
Mean difference
P value
0.006
0.008
0.38
0.26
0 (reference)
Albumin excretion rate (g/min)
Mean at baseline
6.34.6
6.56.7
6.46.2
Mean over 5-yr period
7.715.5
10.617.6
6.55.9
Change vs. placebo
Mean difference
1.3
4.0
P value
0.47
0.03
Mean at 5 yr
6.97.8
14.036.1
0 (reference)
5.33.9
Change vs. placebo
Mean difference
1.0
8.0
P value
0.74
0.007
0 (reference)
GFR (ml/min/1.73 m2 of body-surface area)
Mean at baseline
12920
13118
12622
Mean over 5-yr period
12418
12517
12518
2.6
2.4
Change vs. placebo
Mean difference
P value
Mean at 5 yr
0.11
0.14
12320
12121
0 (reference)
12022
Change vs. placebo
Mean difference
0.4
P value
0.88
1.5
0 (reference)
0.54
* Plusminus values are means SD. The change in the mesangial fractional volume is the fraction of glomerular volume
occupied by mesangium at 5 years minus that at baseline, calculated for 86 patients receiving enalapril, 85 receiving
losartan, and 85 receiving placebo. The adjusted difference was calculated with the use of data adjusted for mesangial
fractional volume at baseline, blood pressure, glycated hemoglobin value, glomerular filtration rate (GFR), albumin excretion rate, age at diabetes onset, diabetes duration, and sex. The albumin excretion rate and glomerular filtration rate
were assessed during the 5-year period and at 5 years, for 94 patients receiving enalapril, 96 receiving losartan, and 95
receiving placebo.
These analyses were adjusted for the baseline albumin excretion rate.
These analyses were adjusted for the baseline GFR.
The albumin excretion rate increased significantly from baseline only in the losartan group
(P=0.04). As compared with placebo, the 5-year
average rate was higher by 4.0 g per minute with
losartan (P=0.03) but was not significantly higher
with enalapril (P=0.47) (Table 2). The albumin
excretion rate at 5 years was higher with losartan
than with placebo, by 8.0 g per minute (P=0.007),
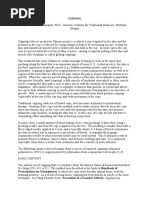
but not with enalapril (P=0.74). The microalbuminuria 5-year cumulative incidence was higher
with losartan than with placebo (17% vs. 6%,
P=0.01 by the log-rank test) but was not signifi-
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
45
The
n e w e ng l a n d j o u r na l
cantly higher with enalapril (4% vs. 6%, P=0.96
by the log-rank test) (Fig. 2). The GFR decreased
similarly in all three groups over the 5 years: by
6.6 to 8.9 ml per minute (P<0.002 for all three)
(Table 2, and Fig. 2 in the Supplementary Appendix).
Of the 285 patients who underwent randomization, 32 were excluded from the diabetic retinopathy study (Fig. 1): 28 had photos taken too
late to qualify as baseline photos (>1 year after
randomization), and 4 had proliferative diabetic
retinopathy. Of the remaining 253 participants,
223 (88%) completed the diabetic retinopathy
studies; 122 had baseline photographs taken before randomization and 101 had them taken
within 4.84.8 months after randomization. There
were no significant differences at baseline between the patients with and those without both
baseline and 5-year photographs (Table 6 in the
Supplementary Appendix) or among the patients
that had both (Table 7 in the Supplementary Appendix). At baseline, 34% of patients had no diabetic retinopathy (level 10 in both eyes), 40% had
minimal nonproliferative diabetic retinopathy (level 21 in one or both eyes), 18% had early nonproliferative diabetic retinopathy (levels 31 through
37 in the worse eye), and 9% had moderate-tosevere nonproliferative diabetic retinopathy (levels 41 through 53 in the worse eye). Baseline distributions of diabetic retinopathy severity scores
among groups were not significantly different
(Fig. 3 in the Supplementary Appendix). A total
of 94% of the patients with diabetic retinopathy
progression of two steps or more or three steps
or more had no or minimal nonproliferative dia0.20
Cumulative Proportion
with Microalbuminuria
0.18
0.16
0.14
Losartan
0.12
0.10
0.08
Placebo
0.06
0.04
Enalapril
0.02
0.00
m e dic i n e
betic retinopathy (levels 10 through 37) at baseline,
with 7% occurring in patients with more severe
retinopathy (levels 40 through 53). This pattern
did not vary significantly among groups. One patient in the placebo group and one in the enalapril group required laser therapy.
A progression in diabetic retinopathy of two
steps or more occurred in 38% of patients receiving placebo but only 25% of those receiving
enalapril (P=0.02) and 21% of those receiving
losartan (P=0.008) (Table 3). The odds of progression of two steps or more was reduced by
65% with enalapril (odds ratio vs. placebo, 0.35;
95% confidence interval [CI], 0.14 to 0.85) and
by 70% with losartan (odds ratio vs. placebo, 0.30;
95% CI, 0.12 to 0.73) (Table 3). Results were
similar for progression of three steps or more
(Table 4). These effects remained even after adjustment for the mean of all blood-pressure measurements obtained during the 5-year study, time
to first retinal photograph, and time to doubled
drug dose and also after multiple imputation
analyses accounting for patients lacking second
photographs.
Adverse Events
Serious adverse events were few and similar
among the three groups (Table 4). There were
three deaths: one from ketoacidosis in the enalapril group, one from traumatic cerebral hemorrhage in the losartan group, and one from hypoglycemia in the placebo group. There were two
perinephric hematomas and one large bladder
clot, but no permanent sequelae. Similar numbers
of participants had hypoglycemia or ketoacidosis,
or both, in the three groups. Chronic cough occurred in 12 patients receiving enalapril, 6 receiving losartan, and 4 receiving placebo (Table 4);
2 of the patients in the enalapril group discontinued the drug for this reason. Transient hyperkalemia occurred in one patient in the enalapril
group, and transient elevation of the serum creatinine level occurred in one patient in the losartan group, with neither requiring discontinuation
of the study medication (Table 4).
Discussion
0
12
24
36
48
60
Months
Figure 2. KaplanMeier Estimates of Time to Microalbuminuria.
ICM
REG F
AUTHOR: Mauer
RETAKE
FIGURE: 2 of 2
CASE
46
of
EMail
Enon
ARTIST: ts
Line
H/T
Combo
4-C
H/T
AUTHOR, PLEASE NOTE:
1st
2nd
3rd
Mesangial fractional volume, the primary prespecified renal end point in RASS, is the variable
most closely correlated with reduction of GFR in
diabetic nephropathy.14 Despite normal blood
Revised
SIZE
n
engl j med 361;1 nejm.org july 2, 2009
22p3
Downloaded
www.nejm.org
on has
Julybeen
17,reset.
2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
Figurefrom
has been
redrawn and type
Please check carefully.
Enalapril and Losartan in Type 1 Diabetes
Table 3. Effects of Enalapril and Losartan on Retinopathy, as Measured by the Odds Ratio of Progression,
during the Five-Year Follow-up Period.
Progression
No. of Events
Adjusted Odds Ratio (95% CI)*
P Value
no./total no. (%)
By two steps or more
Placebo
28/74 (38)
Reference
Reference
Enalapril
19/77 (25)
0.35 (0.140.85)
0.02
Losartan
15/72 (21)
0.30 (0.120.73)
0.008
Placebo
21/74 (28)
Reference
Reference
Enalapril
15/77 (19)
0.41 (0.161.05)
0.06
Losartan
9/72 (12)
0.21 (0.070.62)
0.005
By three steps or more
* The odds ratio was adjusted for baseline characteristics, center, and baseline grade on the 15-point diabetic retinopathy
severity scale.
pressures and albumin excretion rates, at baseline
our patients had structural abnormalities characteristic of diabetic nephropathy.19 Increased mesangial fractional volume in type 1 diabetes, as
confirmed in RASS, results primarily from an increase in mesangial matrix, with a lesser contribution from an increase in the mesangial cellular
component.20 Thus, the mesangial fractional volume increased, and all glomerular structural features of diabetic nephropathy, except for mesangial-cell fractional volume, progressed in the
placebo group, and neither enalapril nor losartan
significantly reduced these rates of progression
(Table 5 in the Supplementary Appendix). These
structural features do not vary according to age,
within the age range of the RASS patients.26
There were also no significant benefits of treatment on albuminuria or reduction of GFR. However, the albumin excretion rate was higher in the
losartan group than in the placebo group, during
and at the end of the study, and more patients in
the losartan group had progression to microalbuminuria. DIRECT also found no benefit of 4.7
years of ARB treatment with candesartan on microalbuminuria incidence in patients with normoalbuminuria and type 1 diabetes or type 2 diabetes
but did not find a higher incidence of microalbuminuria among patients receiving candesartan
as compared with those receiving placebo.27 Thus,
our unexpected and unexplained finding of an increase in microalbuminuria incidence in the losartan group currently lacks confirmation in other
randomized controlled trials. Nonetheless, careful
monitoring of the albumin excretion rate is rec-
ommended if ARBs are prescribed to such patients. The rate of reduction of GFR was approximately twice that expected among normal people
in the age range of our patients,28 but it did not
differ significantly among the three study groups.
The observed early declines in GFR may be important; a low GFR in patients with type 1 diabetes
and normoalbuminuria is associated with worse
lesions,29 and progressive reduction of GFR in patients with type 1 diabetes and microalbuminuria
is predictive of an increasing albumin excretion
rate over time.30
Blockers of the reninangiotensin system appear to be more effective than other antihypertensive agents in reducing the time to doubling
of the serum creatinine level, to dialysis, or to
death in patients with elevated serum creatinine
levels who also have type 1 diabetes and protein
uria4 or type 2 diabetes.5,6 Although an ACE inhibitor slowed interstitial expansion in protein
uric type 2 diabetes,31 RASS showed that the
fractional volume of the interstitium increased by
more than 50% in all three study groups (Table 4
in the Supplementary Appendix). Thus, it may be
misleading to extrapolate from more advanced
stages of diabetic nephropathy to early stages or
from type 2 diabetes to type 1 diabetes, especially given the substantial differences in the
relation of renal structure to albuminuria32 and
the frequent presence of hypertension, obesity,
and other risk factors for albuminuria in patients
with type 2 diabetes.2 Decreased progression of
microalbuminuria to proteinuria in patients with
diabetes could result from direct effects of ACE
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
47
The
n e w e ng l a n d j o u r na l
of
m e dic i n e
Table 4. Adverse Events, According to Study Group.*
Event
Enalapril
Losartan
Placebo
No. of
Events
No. of
Patients
No. of
Events
No. of
Patients
No. of
Events
No. of
Patients
Biopsy-related
Whole body
Cardiovascular system
10
13
11
Serious adverse events
Digestive system
Endocrine
Hemolymphatic system
Metabolic or nutritional
23
Musculoskeletal system
Nervous system
Respiratory system
Skin and appendages
Special senses
Urogenital system
Adverse events
Biopsy-related
Whole body
Cardiovascular system
Digestive system
Endocrine
26
21
36
26
35
32
24
19
42
32
23
21
104
57
106
52
90
54
Hemolymphatic system
16
12
Metabolic or nutritional
125
37
137
48
133
44
Musculoskeletal system
79
49
89
48
63
41
Nervous system
34
24
36
23
23
17
Respiratory system
158
72
148
60
112
59
Skin and appendages
40
29
49
34
53
37
Special senses
27
25
42
26
45
32
Urogenital system
74
34
88
41
70
36
* Serious adverse events and adverse events are mutually exclusive. The events are classified according to the Coding
Symbols for Thesaurus of Adverse Reaction Terms, fifth edition, of the Food and Drug Administration.
Among metabolic or nutritional events, for serious adverse events, 12 episodes of hyperglycemia and ketoacidosis occurred in a single patient, and for adverse events, transient hyperkalemia occurred in one patient receiving enalapril
and transient elevation of the serum creatinine level occurred in one patient receiving losartan, with neither requiring
discontinuation of the study drug.
Among respiratory-system events, chronic cough occurred in 12 patients receiving enalapril (2 of whom discontinued
enalapril for this reason), 6 receiving losartan, and 4 receiving placebo.
inhibitors on proteinuria.11,33 Thus, despite 8 years
of treatment with an ACE inhibitor, 2 months
after its discontinuation, the levels of albuminuria no longer differed significantly from that associated with a placebo,33 suggesting masking of
progression of underlying injury. In a small study
of patients with type 1 diabetes, measurements of
48
structural changes from diabetic nephropathy in
renal-biopsy specimens were similar in the seven
patients receiving an ARB and the three receiving
placebo.34
Our large, randomized, double-blind, placebocontrolled trial examined the effects of renin
angiotensin system blockade on early renal struc-
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
Enalapril and Losartan in Type 1 Diabetes
tural changes in normotensive patients with
type 1 diabetes and normoalbuminuria. Thus,
although the failure to detect benefits of such
blockade on structural or functional outcomes
from diabetic nephropathy may initially seem at
odds with results of other studies, RASS is not
comparable to earlier work. Since the patients in
our study were selected to have no clinically detectable renal disease at baseline, they most likely
included patients who are at low risk for diabetic
nephropathy. Moreover, although the rate of
change in mesangial fractional volume in the
placebo group, 0.016, was significant, the rate
was less than the expected rate of 0.053 that was
computed on the basis of data from 21 patients
with type 1 diabetes who met our entry criteria
and had participated in an earlier study.21 The
effect on the statistical power of the study can
be seen from the lower bound of the 95% confidence interval for the difference in the rate of
change in mesangial fractional volume, suggesting that the use of enalapril and losartan result
in, at most, a reduction in progression of 0.026
and 0.005 units, respectively, as compared with
placebo. We estimate that the benefits we may
have missed would be at most half to one tenth
the rate of increase in mesangial fractional volume required to regularly result in protein
uria.3,14 There was no significant influence of
the duration of type 1 diabetes on the primary
outcome.
Important secondary structural variables, such
as interstitial fractional volume,22 also showed
no benefit of treatment, despite large increases
from baseline in the placebo group. Currently,
there are no accurate predictors of diabetic
nephropathy risk for patients meeting the entry
criteria of the present study. Thus, although a
study involving only normotensive patients with
type 1 diabetes and normoalbuminuria who were
at high risk for nephropathy might have provided
different results, such a study is not feasible at
present.
Treatment with enalapril and losartan were
both associated with a reduction in the progression of diabetic retinopathy by two or three steps
or more of approximately 65% and 70%, respective
ly. These reductions, which are unrelated to glycemia, might be from blood-pressure lowering or
direct effects of blockage of the retinal renin
angiotensin system. Earlier trials35,36 showed lesser progression of diabetic retinopathy in patients
with type 2 diabetes who underwent tight blood-
pressure control, independent of the use of an
ACE inhibitor. The severity of diabetic retinopathy at baseline in the normotensive RASS patients
correlated with the nighttime systolic blood pressure.37 Although the benefit with regard to diabetic retinopathy remained after adjustment for
the lower blood pressures recorded during the
study in the enalapril group and the losartan
group, as compared with the placebo group, we
cannot rule out effects of blood pressure on
these diabetic retinopathy outcomes.
Our findings are consistent with those of
DIRECTPrevent 112 of patients with type 1 diabetes who did not have diabetic retinopathy, in
which diabetic retinopathy was less likely to develop in those receiving an ARB (candesartan)
than in those receiving placebo (hazard ratio,
0.82; 95% CI, 0.67 to 1.00; P=0.051). However,
our findings are inconsistent with those of the
DIRECTProtect 1,12 in which there was no benefit of candesartan in patients with nonproliferative diabetic retinopathy (hazard ratio for the development of diabetic retinopathy, vs. placebo
group, 1.02; 95% CI, 0.80 to 1.31; P=0.85). The
reasons for these differences in diabetic retinopathy progression are unknown and not easily explainable by the differences between the RASS
and DIRECT-Protect 1 patients in their severity
of diabetic retinopathy, blood pressure, glycemia,
or diabetes duration at baseline.12
The reninangiotensin system has been implicated in the pathogenesis of diabetic retinopathy.38 Angiotensin II synthesis occurs in ocular
areas susceptible to diabetic retinopathy.39 Vitreous levels of vascular endothelial growth factor
are increased in the eyes of patients with proliferative diabetic retinopathy40 and are correlated
with vitreous activity of ACE.41 Thus, the benefits of enalapril and losartan on diabetic retinopathy in the present study may represent direct
effects on the eye, independent of effects of systemic blood pressure.
In summary, we did not detect structural or
functional benefits on nephropathy from the
blockade of the reninangiotensin system with
an ACE inhibitor or an ARB in normotensive patients with type 1 diabetes and normoalbuminuria. Given the current status of our ability to
predict the risk of nephropathy, blockade of the
reninangiotensin system for the primary prevention of diabetic nephropathy in patients with
type 1 diabetes is not supported by the present
evidence. In contrast, we found beneficial effects
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
49
The
n e w e ng l a n d j o u r na l
of the ACE inhibitor enalapril and the ARB losartan in reducing the risk of progression of diabetic retinopathy.
Supported by research grants from the National Institutes of
Health (NIH), the National Institute of Diabetes and Digestive
and Kidney Diseases (DK51975), Merck (in the United States),
Merck Frosst (in Canada), and the Canadian Institutes of Health
Research (CIHR) (DCT 14281). RASS was supported in part by a
grant from the National Center for Research Resources of the
NIH, to the University of Minnesota General Clinical Research
Center (GCRC) (M01-RR00400). Dr. Suissa was the recipient of a
Distinguished Investigator Award from the CIHR.
Dr. Mauer reports receiving consulting and lecture fees from
Genzyme and research grants from Merck and Genzyme; Dr.
Zinman, lecture fees, consulting fees, and research grants from
Merck; Dr. Gardiner, lecture fees, consulting fees, and research
grants from AstraZeneca; and Dr. Suissa, lecture fees from
Boehringer Ingelheim and Pfizer, consulting fees from Merck,
and research grants from Boehringer Ingelheim, Organon, and
Wyeth. Dr. Klein reports being an advisory board member for
AstraZeneca (through the DIRECT study), Pfizer, Lilly, and Novartis. No other potential conflict of interest relevant to this article was reported.
of
m e dic i n e
We thank the dedicated staff of the RASS trial in Minneapolis
J. Basgen (morphometry laboratory supervisor), J. Bucksa (central biochemistry laboratory manager), B. Chavers (central albumin laboratory director), M. Cohen and P. Stanaitis (fundus photographers), T. Groppoli, A. Palmer, and S. Rozen (electron
microscopists), K. Johnson (pharmacist), S. Kupcho (central albumin laboratory supervisor), B. Lohr (pharmacy clinical specialist),
D. Luke (pharmacy coordinator), M. Nowicki (central laboratory
lead technician), K. Sawyer (central albumin laboratory junior scientist), S. Sisson-Ross (light-microscopy morphometrist), J. Stein
(assistant project manager), and the GCRC staff; in Montreal B.
Maruca (trial coordinator), G. Carro-Ciampi (pharmacy coordinator), L. Marcon (fundus photographer), A. Roy (research nurse),
and the GCRC staff; in Toronto A. Barnie (trial coordinator), A.
Roode and E. Vivero (research nurses), and Drs. Hertzel Gerstein
and Ronnie Aronson (physicians); the Madison Ocular Epidemiology Reading Center staff S. Meuer (grader), T. Jan (coordinator), and S. Moss (biostatistician); and the Montreal Data Center
staff D. Gaudreau (administrative assistant), V. Lucas (dataentry technician), C. Delaney, S. Vahey, and S. DellAniello (statisticians), Dr. Michael Kramer (advisor), as well as Joyce Stein, Patricia Erickson, Sandy Cragg, and Katie Tabaka for manuscript
preparation; Drs. Maria Luiza Caramori and Paola Fioretto for
critical reading of a previous draft of this manuscript; and especially the patients who volunteered for these demanding studies.
References
1. Foley RN, Collins AJ. End-stage renal
disease in the United States: an update
from the United States Renal Data System.
J Am Soc Nephrol 2007;18:2644-8.
2. Parving H-H, Mauer M, Ritz E. Diabetic nephropathy. 8th ed. Philadelphia:
Saunders, 2008.
3. Caramori ML, Kim Y, Huang C, et al.
Cellular basis of diabetic nephropathy. 1.
Study design and renal structural-functional relationships in patients with longstanding type 1 diabetes. Diabetes 2002;
51:506-13. [Erratum, Diabetes 2002;51:
1294.]
4. Lewis EJ, Hunsicker LG, Bain RP,
Rohde RD. The effect of angiotensin-convertingenzyme inhibition on diabetic
nephropathy. N Engl J Med 1993;329:145662. [Erratum, N Engl J Med 1993;330:
152.]
5. Lewis EJ, Hunsicker LG, Clarke WR,
et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in
patients with nephropathy due to type 2
diabetes. N Engl J Med 2001;345:851-60.
6. Brenner BM, Cooper ME, de Zeeuw D,
et al. Effects of losartan on renal and cardiovascular outcomes in patients with
type 2 diabetes and nephropathy. N Engl J
Med 2001;345:861-9.
7. Parving H-H, Persson F, Lewis JB,
Lewis EJ, Hollenberg NK. Aliskiren combined with losartan in type 2 diabetes and
nephropathy. N Engl J Med 2008;358:243346.
8. Rossing P, Hommel E, Smidt UM,
Parving HH. Reduction in albuminuria
predicts a beneficial effect on diminish-
50
ing the progression of human diabetic
nephropathy during antihypertensive treat
ment. Diabetologia 1994;37:511-6.
9. Calvo G, de Andres-Trelles F. Albuminuria as a surrogate marker for drug
development: a European Regulatory perspective. Kidney Int Suppl 2004;92:S126S127.
10. Gde P, Vedel P, Larsen N, Jensen
GVH, Parving H-H, Pedersen O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes.
N Engl J Med 2003;348:383-93.
11. Jerums G, Panagiotopoulos S, Premaratne E, Power DA, MacIsaac RJ. Lowering of proteinuria in response to antihypertensive therapy predicts improved
renal function in late but not in early diabetic nephropathy: a pooled analysis. Am
J Nephrol 2008;28:614-27.
12. Chaturvedi N, Porta M, Klein R, et
al. Effect of candesartan on prevention
(DIRECT-Prevent1) and progression
(DIRECT-Protect 1) of retinopathy in type 1
diabetes: randomised, placebo-controlled
trials. Lancet 2008;372:1394-402.
13. Mauer M, Zinman B, Gardiner R, et al.
ACE-I and ARBs in early diabetic nephropathy. J Renin Angiotensin Aldosterone
Syst 2002;3:262-9.
14. Mauer SM, Steffes MW, Ellis EN,
Sutherland DE, Brown DM, Goetz FC.
Structural-functional relationships in diabetic nephropathy. J Clin Invest 1984;74:
1143-55.
15. Andersen S, Tarnow L, Rossing P,
Hansen BV, Parving HH. Renoprotective
effects of angiotensin II receptor block-
ade in type 1 diabetic patients with diabetic nephropathy. Kidney Int 2000;57:
601-6.
16. Wiseman MJ, Hunt R, Goodwin A,
Gross JL, Keen H, Viberti GC. Dietary
composition and renal function in healthy
subjects. Nephron 1987;46:37-42.
17. Mauer M, Drummond K. The early
natural history of nephropathy in type 1
diabetes. I. Study design and baseline
characteristics of the study participants.
Diabetes 2002;51:1572-9.
18. Gaspari F, Perico N, Matalone M, et al.
Precision of plasma clearance of iohexol
for estimation of GFR in patients with renal disease. J Am Soc Nephrol 1998;9:
310-3.
19. Klein R, Zinman B, Gardiner R, et al.
The relationship of diabetic retinopathy to
preclinical diabetic glomerulopathy lesions
in type 1 diabetic patients: the ReninAngiotensin System Study. Diabetes 2005;
54:527-33.
20. Steffes MW, Bilous RW, Sutherland
DE, Mauer SM. Cell and matrix components of the glomerular mesangium in
type I diabetes. Diabetes 1992;41:679-84.
21. Drummond K, Mauer M. The early
natural history of nephropathy in type 1
diabetes. II. Early renal structural changes
in type 1 diabetes. Diabetes 2002;51:
1580-7.
22. Katz A, Caramori ML, Sisson-Ross S,
Groppoli T, Basgen JM, Mauer M. An increase in the cell component of the cortical interstitium antedates interstitial fibrosis in type 1 diabetic patients. Kidney Int
2002;61:2058-66.
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
Enalapril and Losartan in Type 1 Diabetes
23. Fundus photographic risk factors for
progression of diabetic retinopathy: ETDRS
report number 12. Ophthalmology 1991;
98:Suppl:823-33.
24. Klein R, Klein BE, Magli YL, et al.
An alternative method of grading diabet
ic retinopathy. Ophthalmology 1986;93:
1183-7.
25. Klein R, Klein BE, Moss SE. How many
steps of progression of diabetic retinopathy are meaningful? The Wisconsin Epidemiologic Study of Diabetic Retinopathy.
Arch Ophthalmol 2001;119:547-53.
26. Steffes MW, Barbosa J, Basgen JM,
Sutherland DE, Najarian JS, Mauer SM.
Quantitative glomerular morphology of the
normal human kidney. Lab Invest 1983;49:
82-6.
27. Bilous R, Chaturvedi N, Sjlie AK, et
al. Effect of candesartan on microalbuminuria and albumin excretion rate in
diabetes: three randomized trials. Ann
Intern Med 2009 May 18 (Epub ahead of
print).
28. Rule AD, Gussak HM, Pond GR, et al.
Measured and estimated GFR in healthy
potential kidney donors. Am J Kidney Dis
2004;43:112-9. [Errata, Am J Kidney Dis
2004;44:1126, 2005;46:170.]
29. Caramori ML, Fioretto P, Mauer M.
Low glomerular filtration rate in normo
albuminuric type 1 diabetic patients: an
indicator of more advanced glomerular
lesions. Diabetes 2003;52:1036-40.
30. Perkins BA, Ficociello LH, Ostrander
BE, et al. Microalbuminuria and the risk
for early progressive renal function decline
in type 1 diabetes. J Am Soc Nephrol
2007;18:1353-61.
31. Cordonnier DJ, Pinel N, Barro C, et al.
Expansion of cortical interstitium is limited by converting enzyme inhibition in
type 2 diabetic patients with glomerulosclerosis. J Am Soc Nephrol 1999;10:125363.
32. Fioretto P, Stehouwer CD, Mauer M, et
al. Heterogeneous nature of microalbuminuria in NIDDM: studies of endothelial
function and renal structure. Diabetologia 1998;41:233-6.
33. Mathiesen ER, Hommel E, Hansen HP,
Smidt UM, Parving HH. Randomised controlled trial of long term efficacy of captopril on preservation of kidney function in
normotensive patients with insulin dependent diabetes and microalbuminuria. BMJ
1999;319:24-5.
34. Perrin NE, Jaremko GA, Berg UB. The
effects of candesartan on diabetes glomerulopathy: a double-blind, placebo-controlled trial. Pediatr Nephrol 2008;23:94754.
35. Matthews DR, Stratton IM, Aldington
SJ, Holman RR, Kohner EM. Risks of progression of retinopathy and vision loss
related to tight blood pressure control in
type 2 diabetes mellitus: UKPDS 69. Arch
Ophthalmol 2004;122:1631-40.
36. Schrier RW, Estacio RO, Esler A,
Mehler P. Effects of aggressive blood pres-
sure control in normotensive type 2 diabetic patients on albuminuria, retinopathy
and strokes. Kidney Int 2002;61:1086-97.
37. Klein R, Moss SE, Sinaiko AR, et al.
The relation of ambulatory blood pressure
and pulse rate to retinopathy in type 1
diabetes mellitus: the Renin-Angiotensin
System Study. Ophthalmology 2006;113:
2231-6.
38. Nagai N, Izumi-Nagai K, Oike Y, et al.
Suppression of diabetes-induced retinal inflammation by blocking the angiotensin
II type 1 receptor or its downstream nuclear factor-kappaB pathway. Invest Ophthalmol Vis Sci 2007;48:4342-50.
39. Wagner J, Jan Danser AH, Derkx FH,
et al. Demonstration of renin mRNA, angiotensinogen mRNA, and angiotensin
converting enzyme mRNA expression in
the human eye: evidence for an intraocular renin-angiotensin system. Br J Ophthal
mol 1996;80:159-63.
40. Aiello LP, Avery RL, Arrigg PG, et al.
Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl
J Med 1994;331:1480-7.
41. Ishizaki E, Takai S, Ueki M, et al. Correlation between angiotensin-converting
enzyme, vascular endothelial growth factor, and matrix metalloproteinase-9 in the
vitreous of eyes with diabetic retinopathy.
Am J Ophthalmol 2006;141:129-34.
Copyright 2009 Massachusetts Medical Society.
powerpoint slides of journal figures and tables
At the Journals Web site, subscribers can automatically create PowerPoint slides.
In a figure or table in the full-text version of any article at NEJM.org, click
on Get PowerPoint Slide. A PowerPoint slide containing the image, with its title
and reference citation, can then be downloaded and saved.
n engl j med 361;1 nejm.org july 2, 2009
Downloaded from www.nejm.org on July 17, 2009 . Copyright 2009 Massachusetts Medical Society. All rights reserved.
51
You might also like
- Https:/zero Sci-Hub Se/5089//boulet2016No ratings yetHttps:/zero Sci-Hub Se/5089//boulet201610 pages
- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesNo ratings yetCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 Diabetes12 pages
- Aliskiren Combined With Losartan in Type 2 DiabetesNo ratings yetAliskiren Combined With Losartan in Type 2 Diabetes14 pages
- High Prevalence of Nonalcoholic Fatty Liver Disease in Patients With Type 2 Diabetes Mellitus and Normal Plasma Aminotransferase Levels - PMCNo ratings yetHigh Prevalence of Nonalcoholic Fatty Liver Disease in Patients With Type 2 Diabetes Mellitus and Normal Plasma Aminotransferase Levels - PMC18 pages
- Type 2 diabetes mellitus and non-alcoholic fatty liver disease: a systematic review and meta-analysisNo ratings yetType 2 diabetes mellitus and non-alcoholic fatty liver disease: a systematic review and meta-analysis7 pages
- Effect of Dietary Protein Restriction On Prognosis in Patients With Diabetic NephropathyNo ratings yetEffect of Dietary Protein Restriction On Prognosis in Patients With Diabetic Nephropathy9 pages
- Review Article: Pharmacogenomics of Drug Response in Type 2 Diabetes: Toward The Definition of Tailored Therapies?No ratings yetReview Article: Pharmacogenomics of Drug Response in Type 2 Diabetes: Toward The Definition of Tailored Therapies?11 pages
- Relation Between Kidney Function, Proteinuria, and Adverse OutcomesNo ratings yetRelation Between Kidney Function, Proteinuria, and Adverse Outcomes7 pages
- 2015 Updates On The Management of Diabetes in Dialysis PatientsNo ratings yet2015 Updates On The Management of Diabetes in Dialysis Patients22 pages
- Prevalence, Risk Factors, Adherence and Non Adherence in Patient With Chronic Kidney Disease: A Prospective StudyNo ratings yetPrevalence, Risk Factors, Adherence and Non Adherence in Patient With Chronic Kidney Disease: A Prospective Study7 pages
- AN UPDATE= INCIDENCE OF NEW ONSET DIABETES AFTER KIDNEY TRANSPLANTATION AT NATIONAL KIDNEY AND TRANSPLANT INSTITUTE (NKTI) ~ A FIVE~YEAR RETROSPECTIVE STUDY (2022)No ratings yetAN UPDATE= INCIDENCE OF NEW ONSET DIABETES AFTER KIDNEY TRANSPLANTATION AT NATIONAL KIDNEY AND TRANSPLANT INSTITUTE (NKTI) ~ A FIVE~YEAR RETROSPECTIVE STUDY (2022)8 pages
- Ten Common Mistakes in The Management of Lupus Nephritis. 2014No ratings yetTen Common Mistakes in The Management of Lupus Nephritis. 201410 pages
- Gout Treatment Dosage Affects Risk For Hypersensitivity SyndromeNo ratings yetGout Treatment Dosage Affects Risk For Hypersensitivity Syndrome5 pages
- Association of High Blood Pressure With RenalNo ratings yetAssociation of High Blood Pressure With Renal6 pages
- Evaluation of Antidiabetic Drug Use in Type 2 Diabetes Mellitus Patients With Chronic Kidney Disease at Dr. M. Djamil Hospital PadangNo ratings yetEvaluation of Antidiabetic Drug Use in Type 2 Diabetes Mellitus Patients With Chronic Kidney Disease at Dr. M. Djamil Hospital Padang5 pages
- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesNo ratings yetCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 Diabetes12 pages
- FREQUENCY - OF - NEPHROPATHY - AND - ITS - RELATION - TO - METAB (Diskusi)No ratings yetFREQUENCY - OF - NEPHROPATHY - AND - ITS - RELATION - TO - METAB (Diskusi)5 pages
- Hanefeld Et Al-2017-Diabetes, Obesity and MetabolismNo ratings yetHanefeld Et Al-2017-Diabetes, Obesity and Metabolism8 pages
- Diabetes Secondary To Treatment With Statins (Laakso 2017)No ratings yetDiabetes Secondary To Treatment With Statins (Laakso 2017)9 pages
- A Trial of Darbepoetin A: Volume 361:2019-2032 November 19, 2009 Number 21No ratings yetA Trial of Darbepoetin A: Volume 361:2019-2032 November 19, 2009 Number 2113 pages
- Delima Et Al. - 2017 - Faktor Risiko Penyakit Ginjal Kronik Studi Kasus Kontrol Di Empat Rumah Sakit Di Jakarta Tahun 2014-AnnotatedNo ratings yetDelima Et Al. - 2017 - Faktor Risiko Penyakit Ginjal Kronik Studi Kasus Kontrol Di Empat Rumah Sakit Di Jakarta Tahun 2014-Annotated10 pages
- Chronic Kidney Disease in Primary Care: Duaine D. Murphree, MD, and Sarah M. Thelen, MDNo ratings yetChronic Kidney Disease in Primary Care: Duaine D. Murphree, MD, and Sarah M. Thelen, MD9 pages
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Cupping: Guasha. Still, A Certain Amount of Bruising Is Expected Both From Fixed Position Cupping100% (1)Cupping: Guasha. Still, A Certain Amount of Bruising Is Expected Both From Fixed Position Cupping7 pages
- Effects of Antihypertensive Drugs On Thyroid Function in Type 2 Diabetes Patients With EuthyroidismNo ratings yetEffects of Antihypertensive Drugs On Thyroid Function in Type 2 Diabetes Patients With Euthyroidism12 pages
- Phil National Drug Formulary Vol1ed7 - 2008100% (5)Phil National Drug Formulary Vol1ed7 - 2008315 pages
- Antihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.No ratings yetAntihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.44 pages
- Treatment of Systemic Hypertension Associated With Kidney DiseaseNo ratings yetTreatment of Systemic Hypertension Associated With Kidney Disease6 pages
- For The Candidates Admitted From The Academic Year 2019-2020 Batch OnwardsNo ratings yetFor The Candidates Admitted From The Academic Year 2019-2020 Batch Onwards12 pages
- Ambulatory Blood Pressure Measurement: Brief ReviewNo ratings yetAmbulatory Blood Pressure Measurement: Brief Review8 pages
- NURS FPX 6614 Assessment 1 Defining A Gap in PracticeNo ratings yetNURS FPX 6614 Assessment 1 Defining A Gap in Practice7 pages
- Targeting Hypertension in Patients With Cardiorenal Metabolic SyndromeNo ratings yetTargeting Hypertension in Patients With Cardiorenal Metabolic Syndrome6 pages
- Evaluation and Treatment of Hypertensive Emergencies in Adults - UpToDateNo ratings yetEvaluation and Treatment of Hypertensive Emergencies in Adults - UpToDate13 pages
- Women's Views and Postpartum Follow-Up in The CHIPS Trial (Control of Hypertension in Pregnancy Study)No ratings yetWomen's Views and Postpartum Follow-Up in The CHIPS Trial (Control of Hypertension in Pregnancy Study)9 pages
- Treatment of Hypertension in Older Adults, Particularly Isolated Systolic Hypertension - UpToDateNo ratings yetTreatment of Hypertension in Older Adults, Particularly Isolated Systolic Hypertension - UpToDate34 pages
- Combination Therapy With Amlodipine and Captopril For Resistant Systemic HypertensionNo ratings yetCombination Therapy With Amlodipine and Captopril For Resistant Systemic Hypertension4 pages
- Effect of Valsartan Addition To Amlodipine On AnklNo ratings yetEffect of Valsartan Addition To Amlodipine On Ankl6 pages





























































































- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 Diabetes
- Aliskiren Combined With Losartan in Type 2 DiabetesAliskiren Combined With Losartan in Type 2 Diabetes
- High Prevalence of Nonalcoholic Fatty Liver Disease in Patients With Type 2 Diabetes Mellitus and Normal Plasma Aminotransferase Levels - PMCHigh Prevalence of Nonalcoholic Fatty Liver Disease in Patients With Type 2 Diabetes Mellitus and Normal Plasma Aminotransferase Levels - PMC
- Type 2 diabetes mellitus and non-alcoholic fatty liver disease: a systematic review and meta-analysisType 2 diabetes mellitus and non-alcoholic fatty liver disease: a systematic review and meta-analysis
- Effect of Dietary Protein Restriction On Prognosis in Patients With Diabetic NephropathyEffect of Dietary Protein Restriction On Prognosis in Patients With Diabetic Nephropathy
- Review Article: Pharmacogenomics of Drug Response in Type 2 Diabetes: Toward The Definition of Tailored Therapies?Review Article: Pharmacogenomics of Drug Response in Type 2 Diabetes: Toward The Definition of Tailored Therapies?
- Relation Between Kidney Function, Proteinuria, and Adverse OutcomesRelation Between Kidney Function, Proteinuria, and Adverse Outcomes
- 2015 Updates On The Management of Diabetes in Dialysis Patients2015 Updates On The Management of Diabetes in Dialysis Patients
- Prevalence, Risk Factors, Adherence and Non Adherence in Patient With Chronic Kidney Disease: A Prospective StudyPrevalence, Risk Factors, Adherence and Non Adherence in Patient With Chronic Kidney Disease: A Prospective Study
- AN UPDATE= INCIDENCE OF NEW ONSET DIABETES AFTER KIDNEY TRANSPLANTATION AT NATIONAL KIDNEY AND TRANSPLANT INSTITUTE (NKTI) ~ A FIVE~YEAR RETROSPECTIVE STUDY (2022)AN UPDATE= INCIDENCE OF NEW ONSET DIABETES AFTER KIDNEY TRANSPLANTATION AT NATIONAL KIDNEY AND TRANSPLANT INSTITUTE (NKTI) ~ A FIVE~YEAR RETROSPECTIVE STUDY (2022)
- Ten Common Mistakes in The Management of Lupus Nephritis. 2014Ten Common Mistakes in The Management of Lupus Nephritis. 2014
- Gout Treatment Dosage Affects Risk For Hypersensitivity SyndromeGout Treatment Dosage Affects Risk For Hypersensitivity Syndrome
- Evaluation of Antidiabetic Drug Use in Type 2 Diabetes Mellitus Patients With Chronic Kidney Disease at Dr. M. Djamil Hospital PadangEvaluation of Antidiabetic Drug Use in Type 2 Diabetes Mellitus Patients With Chronic Kidney Disease at Dr. M. Djamil Hospital Padang
- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 Diabetes
- FREQUENCY - OF - NEPHROPATHY - AND - ITS - RELATION - TO - METAB (Diskusi)FREQUENCY - OF - NEPHROPATHY - AND - ITS - RELATION - TO - METAB (Diskusi)
- Hanefeld Et Al-2017-Diabetes, Obesity and MetabolismHanefeld Et Al-2017-Diabetes, Obesity and Metabolism
- Diabetes Secondary To Treatment With Statins (Laakso 2017)Diabetes Secondary To Treatment With Statins (Laakso 2017)
- A Trial of Darbepoetin A: Volume 361:2019-2032 November 19, 2009 Number 21A Trial of Darbepoetin A: Volume 361:2019-2032 November 19, 2009 Number 21
- Delima Et Al. - 2017 - Faktor Risiko Penyakit Ginjal Kronik Studi Kasus Kontrol Di Empat Rumah Sakit Di Jakarta Tahun 2014-AnnotatedDelima Et Al. - 2017 - Faktor Risiko Penyakit Ginjal Kronik Studi Kasus Kontrol Di Empat Rumah Sakit Di Jakarta Tahun 2014-Annotated
- Chronic Kidney Disease in Primary Care: Duaine D. Murphree, MD, and Sarah M. Thelen, MDChronic Kidney Disease in Primary Care: Duaine D. Murphree, MD, and Sarah M. Thelen, MD
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: Urology
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and Gallbladder
- Cupping: Guasha. Still, A Certain Amount of Bruising Is Expected Both From Fixed Position CuppingCupping: Guasha. Still, A Certain Amount of Bruising Is Expected Both From Fixed Position Cupping
- Effects of Antihypertensive Drugs On Thyroid Function in Type 2 Diabetes Patients With EuthyroidismEffects of Antihypertensive Drugs On Thyroid Function in Type 2 Diabetes Patients With Euthyroidism
- Antihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.Antihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.
- Treatment of Systemic Hypertension Associated With Kidney DiseaseTreatment of Systemic Hypertension Associated With Kidney Disease
- For The Candidates Admitted From The Academic Year 2019-2020 Batch OnwardsFor The Candidates Admitted From The Academic Year 2019-2020 Batch Onwards
- Ambulatory Blood Pressure Measurement: Brief ReviewAmbulatory Blood Pressure Measurement: Brief Review
- NURS FPX 6614 Assessment 1 Defining A Gap in PracticeNURS FPX 6614 Assessment 1 Defining A Gap in Practice
- Targeting Hypertension in Patients With Cardiorenal Metabolic SyndromeTargeting Hypertension in Patients With Cardiorenal Metabolic Syndrome
- Evaluation and Treatment of Hypertensive Emergencies in Adults - UpToDateEvaluation and Treatment of Hypertensive Emergencies in Adults - UpToDate
- Women's Views and Postpartum Follow-Up in The CHIPS Trial (Control of Hypertension in Pregnancy Study)Women's Views and Postpartum Follow-Up in The CHIPS Trial (Control of Hypertension in Pregnancy Study)
- Treatment of Hypertension in Older Adults, Particularly Isolated Systolic Hypertension - UpToDateTreatment of Hypertension in Older Adults, Particularly Isolated Systolic Hypertension - UpToDate
- Combination Therapy With Amlodipine and Captopril For Resistant Systemic HypertensionCombination Therapy With Amlodipine and Captopril For Resistant Systemic Hypertension
- Effect of Valsartan Addition To Amlodipine On AnklEffect of Valsartan Addition To Amlodipine On Ankl