Pressure Habits, Etiological Factors in Maloccclusion
Pressure Habits, Etiological Factors in Maloccclusion
Download as pdf or txt
You might also like
- Arco Bimetrico de WilsonDocument171 pagesArco Bimetrico de WilsonStefan Pru100% (3)
- 1 s2.0 S0901502713000374 MainDocument8 pages1 s2.0 S0901502713000374 MainVeerawit LukkanasomboonNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Andrews 1972 The Six Keys To Normal OcclusionDocument15 pagesAndrews 1972 The Six Keys To Normal OcclusionMiguelNo ratings yet
- Catalogo Masel OrtodonciaDocument171 pagesCatalogo Masel OrtodonciaJuan OntiverosNo ratings yet
- C V Dr. Cesar Guerrero 2014Document38 pagesC V Dr. Cesar Guerrero 2014ucbrotherNo ratings yet
- Mcqs in Orthodontics, With Explanatory Answers and ReferencesDocument1 pageMcqs in Orthodontics, With Explanatory Answers and ReferencesS ANo ratings yet
- Oral HabitsDocument198 pagesOral HabitsDRPRIYA007No ratings yet
- Oral HabitDocument24 pagesOral Habitdr parveen bathlaNo ratings yet
- Some Physiologic Consideration of Centric and Other Jaw RelationsDocument12 pagesSome Physiologic Consideration of Centric and Other Jaw RelationsMartha Lia Castaño EcheverryNo ratings yet
- Minimally Invasive Orthognathic SurgeryDocument3 pagesMinimally Invasive Orthognathic SurgeryIJAR JOURNALNo ratings yet
- The Stressed Pulp Condition An Endodontic RestorativeDocument2 pagesThe Stressed Pulp Condition An Endodontic RestorativeChris TayNo ratings yet
- Correcting The Class II Subdivision MalocclusionDocument2 pagesCorrecting The Class II Subdivision MalocclusionplsssssNo ratings yet
- Ortodoncia Bishara 644 Pag-41Document604 pagesOrtodoncia Bishara 644 Pag-41pedro picapiedra100% (1)
- Corticotomy For Orthodontic Tooth MovementDocument8 pagesCorticotomy For Orthodontic Tooth MovementGissellePantojaNo ratings yet
- Wallace, Maxillary Sinus AugmentationDocument16 pagesWallace, Maxillary Sinus AugmentationChin-lungHsieh0% (1)
- Capitulo 8 Crecimiento Craneo FacialDocument32 pagesCapitulo 8 Crecimiento Craneo FacialLady SolarteNo ratings yet
- Kesling AlineadoresDocument8 pagesKesling AlineadoresJazmin ArciniegaNo ratings yet
- ALTERNATE RAPID MAXILLARY EXPANSION AND CONSTRICTION (ALT-RAMEC) MAY BE MORE EFFECTIVE THAN RAPID MAXILLARY EXPANSION ALONE FOR PROTRACTION FACIAL MASK TREATMENTzhao2020Document3 pagesALTERNATE RAPID MAXILLARY EXPANSION AND CONSTRICTION (ALT-RAMEC) MAY BE MORE EFFECTIVE THAN RAPID MAXILLARY EXPANSION ALONE FOR PROTRACTION FACIAL MASK TREATMENTzhao2020محمد نبيل الدعيس100% (1)
- Asymmetric Deep Bite With A Canted Occlusal Plane - A Case ReportDocument9 pagesAsymmetric Deep Bite With A Canted Occlusal Plane - A Case ReportIacominiGustavoNo ratings yet
- Extract Manauta Layers2Document33 pagesExtract Manauta Layers2Sociedad Dentotal Araucanía0% (1)
- IZC OrthoDocument10 pagesIZC OrthoBashar A. HusseiniNo ratings yet
- Cefalometria de TollaroDocument7 pagesCefalometria de TollaroMargareth Brito100% (1)
- The Examination and Recording of The Occlusion: Why and HowDocument10 pagesThe Examination and Recording of The Occlusion: Why and HowlvisageNo ratings yet
- Orthodontic Intrusion: A Contemporary ReviewDocument7 pagesOrthodontic Intrusion: A Contemporary ReviewRockey ShrivastavaNo ratings yet
- Currie Et Al 2017 Angle Orthod PDFDocument14 pagesCurrie Et Al 2017 Angle Orthod PDFplayer osama100% (1)
- Vienna 2012 Program AbstractDocument32 pagesVienna 2012 Program AbstractMCK1348100% (1)
- Dental Trauma - An Overview of Its Influence On The Management of Orthodontic Treatment - Part 1.Document11 pagesDental Trauma - An Overview of Its Influence On The Management of Orthodontic Treatment - Part 1.Djoka DjordjevicNo ratings yet
- 18 1994 - John Preston - The Golden Proportion RevistedDocument5 pages18 1994 - John Preston - The Golden Proportion RevistedSilvia KriNo ratings yet
- Facial Height Index: Case ReportDocument7 pagesFacial Height Index: Case ReportEstefania MontoyaNo ratings yet
- Charles Burstone PDFDocument2 pagesCharles Burstone PDFPaola Lolo100% (1)
- 00 RWISO JOURNAL - Roth Williams International Society of PDFDocument61 pages00 RWISO JOURNAL - Roth Williams International Society of PDFanon_768201406No ratings yet
- 5 Años RothDocument8 pages5 Años RothTOMAS DAVID CHICA LLAMAS100% (1)
- Orthodontics in 3 Millennia. Chapter 16: Late 20th-Century Fixed AppliancesDocument4 pagesOrthodontics in 3 Millennia. Chapter 16: Late 20th-Century Fixed AppliancesDiego Andres Hincapie HerreraNo ratings yet
- Oral Surgery - Treatment Planning GuidelinesDocument5 pagesOral Surgery - Treatment Planning GuidelinesFaizal Prabowo KalimanNo ratings yet
- Van BeekDocument4 pagesVan BeekThendral DevanathanNo ratings yet
- Biografía Robert Ricketts OrtodonciaDocument3 pagesBiografía Robert Ricketts OrtodonciaPablo100% (1)
- Crecimiento y Desarrollo de La ATMDocument9 pagesCrecimiento y Desarrollo de La ATMMaría Fernanda Cea QuintanaNo ratings yet
- Success of Infrazygomatic Crest Bone ScrewsDocument8 pagesSuccess of Infrazygomatic Crest Bone ScrewscdentistacesarmNo ratings yet
- 1alikhani M Ed Clinical Guide To Accelerated Orthodontics WitDocument139 pages1alikhani M Ed Clinical Guide To Accelerated Orthodontics WitMiodrag PopovNo ratings yet
- Joseph R. Jarabak-A Living LegendDocument2 pagesJoseph R. Jarabak-A Living Legendjoseph n100% (1)
- Manual de Odontologia PediatricaDocument251 pagesManual de Odontologia PediatricaMonsters CUNo ratings yet
- Marpe V SarpeDocument10 pagesMarpe V SarpeAngieNo ratings yet
- An Outline of Oral SurgeryDocument272 pagesAn Outline of Oral Surgerydoctorsoha.sh100% (1)
- EWS Rends Rthodontics: A J I T ODocument84 pagesEWS Rends Rthodontics: A J I T OMatias AnghileriNo ratings yet
- Interdisciplinary Approach To The MandibDocument7 pagesInterdisciplinary Approach To The MandibZachary DuongNo ratings yet
- 3 Definition and Prevalence of Dentofacial Deformities 2014 Orthognathic SurgeryDocument8 pages3 Definition and Prevalence of Dentofacial Deformities 2014 Orthognathic Surgeryiweourvgiu100% (1)
- Guidelines For Contemporary Air-Rotor StrippingDocument6 pagesGuidelines For Contemporary Air-Rotor StrippingGerman Cabrera DiazNo ratings yet
- Studies in The Mobility of The Human Mandible: Bibliographic InformationDocument4 pagesStudies in The Mobility of The Human Mandible: Bibliographic InformationRhea OngNo ratings yet
- 999 252 Rev 06 14 Carriere Motion Workbook PDFDocument24 pages999 252 Rev 06 14 Carriere Motion Workbook PDFMiguel Angel Gonzalez HuertaNo ratings yet
- Maxillary Transverse DeficiencyDocument4 pagesMaxillary Transverse DeficiencyCarlos Alberto CastañedaNo ratings yet
- Klammt y KinetorDocument6 pagesKlammt y KinetorMiguel candelaNo ratings yet
- Controlling Factors in Craniofacial GrowthDocument82 pagesControlling Factors in Craniofacial GrowthPrachodh0% (1)
- Historia de La Super Elasticidad Alberto TeramotoDocument12 pagesHistoria de La Super Elasticidad Alberto TeramotoJorge RamírezNo ratings yet
- Ortodoncia Brackets inDocument17 pagesOrtodoncia Brackets injavierNo ratings yet
- The Role of Articulators in Orthodontics and Orthognatic SurgeryDocument5 pagesThe Role of Articulators in Orthodontics and Orthognatic SurgeryDr Shivam VermaNo ratings yet
- Mosby's Orthodontic Review (2nd Edition) Pages 92 - 96Document5 pagesMosby's Orthodontic Review (2nd Edition) Pages 92 - 96sillyazianNo ratings yet
- ATT00183Document7 pagesATT00183Daniel VelezNo ratings yet
- Clinical Periodontology and Implant Dentistry, 2 Volume SetFrom EverandClinical Periodontology and Implant Dentistry, 2 Volume SetNo ratings yet
- Author's Accepted ManuscriptDocument24 pagesAuthor's Accepted ManuscriptMargarita Lopez MartinezNo ratings yet
- Manual Optical de AdhesiónDocument9 pagesManual Optical de AdhesiónMargarita Lopez MartinezNo ratings yet
- TADs - NandaDocument437 pagesTADs - NandaPrabhu Thurai91% (22)
- Diagnosis in Orthodontics - Theory and PracticeDocument13 pagesDiagnosis in Orthodontics - Theory and PracticeMargarita Lopez MartinezNo ratings yet
- ANgle Calvin CaseDocument7 pagesANgle Calvin CaseMargarita Lopez MartinezNo ratings yet
- The Use of Temporary Anchorage Devices For ORTHODONTIC TREATMENT of Class III Uin A Patient With An Impacred Upper CanineDocument7 pagesThe Use of Temporary Anchorage Devices For ORTHODONTIC TREATMENT of Class III Uin A Patient With An Impacred Upper CanineMargarita Lopez MartinezNo ratings yet
- !excellence in Finishing Current Concepts Goals and Mechanics PDFDocument13 pages!excellence in Finishing Current Concepts Goals and Mechanics PDFMargarita Lopez Martinez100% (2)
- Biological Mechanism in The Thoot MovementDocument18 pagesBiological Mechanism in The Thoot MovementMargarita Lopez MartinezNo ratings yet
- Biology Tooth MovementDocument8 pagesBiology Tooth MovementMargarita Lopez MartinezNo ratings yet
- ANgle Calvin CaseDocument7 pagesANgle Calvin CaseMargarita Lopez MartinezNo ratings yet
- ABO Ideal Photos-RadiographsDocument23 pagesABO Ideal Photos-RadiographsMargarita Lopez MartinezNo ratings yet
- Soft Tissues AdaptabilityDocument11 pagesSoft Tissues AdaptabilityMargarita Lopez MartinezNo ratings yet
- La Dieta South Beach PDFDocument416 pagesLa Dieta South Beach PDFMargarita Lopez MartinezNo ratings yet
- Oral Habits in School Going Children of Delhi: A Prevalence StudyDocument5 pagesOral Habits in School Going Children of Delhi: A Prevalence StudyStacia AnastashaNo ratings yet
- 5.etiology of MalocclusionDocument20 pages5.etiology of MalocclusionAhmed Hegazy100% (2)
- Mouth BreathingDocument55 pagesMouth BreathingHansa KunduNo ratings yet
- Throat Pharynx Adenoids ENT LecturesDocument33 pagesThroat Pharynx Adenoids ENT LecturesRaju GangadharanNo ratings yet
- Oral Habits in OrthodonticsDocument111 pagesOral Habits in Orthodonticsdentistpro.org75% (4)
- Habits MDocument94 pagesHabits MVivek Gaurav100% (1)
- 7 Step CBR Program To Better BreathingDocument8 pages7 Step CBR Program To Better BreathingPeter BenNo ratings yet
- Bad HabitsDocument7 pagesBad HabitsAnonymous itwv6oMNo ratings yet
- Sleep With Buteyko - Physician D - McKeown, PatrickDocument137 pagesSleep With Buteyko - Physician D - McKeown, PatrickLuis Oneto RothNo ratings yet
- Nasal Airway and Malocclucion / Orthodontic Courses by Indian Dental AcademyDocument35 pagesNasal Airway and Malocclucion / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
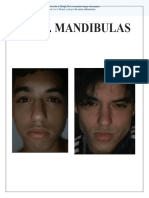
- Mr. Mandibulas: Subscribe To Deepl Pro To Translate Larger Documents. Visit For More InformationDocument87 pagesMr. Mandibulas: Subscribe To Deepl Pro To Translate Larger Documents. Visit For More Informationav495600No ratings yet
- The Hindu Yogi - Science of BreathDocument84 pagesThe Hindu Yogi - Science of Breathm r100% (1)
- Adenoids: What Are They & How Do They Affect My Child's Hearing?Document2 pagesAdenoids: What Are They & How Do They Affect My Child's Hearing?Wahyu JuliandaNo ratings yet
- Adenoid Facies and Its Management An Orthodontic PerspectiveDocument7 pagesAdenoid Facies and Its Management An Orthodontic PerspectiveSatyaki PalNo ratings yet
- Mouth Breathing: Adverse Effects On Facial Growth, Health, Academics, and BehaviorDocument8 pagesMouth Breathing: Adverse Effects On Facial Growth, Health, Academics, and BehaviorlogoioanninaNo ratings yet
- Orofacial Myologist Lip IncompetenceDocument4 pagesOrofacial Myologist Lip IncompetenceLinda DeliaerikaNo ratings yet
- Toxicologie HFDocument7 pagesToxicologie HFArtemisisNo ratings yet
- The Impact of Allergic Rhinitis On Symptom Improvement in Pediatric Patients After AdenotonsillectomyDocument6 pagesThe Impact of Allergic Rhinitis On Symptom Improvement in Pediatric Patients After AdenotonsillectomyBayu PrakosoNo ratings yet
- !chronic Mouth Breathing A Serious Health Concer PDFDocument3 pages!chronic Mouth Breathing A Serious Health Concer PDFBianca IovoaiaNo ratings yet
- Presentation 1Document54 pagesPresentation 1Ishtiaq Hasan100% (1)
- Adenoid Faces ManagementDocument6 pagesAdenoid Faces ManagementVEENA k.aNo ratings yet
- Mouth Breathing I. Etiology and EffectsDocument16 pagesMouth Breathing I. Etiology and EffectsRommy MelgarejoNo ratings yet
- MiofuncionalDocument9 pagesMiofuncionalKaterine TrillosNo ratings yet
- Module 15 - Treatment Planning SlideShow 080306Document45 pagesModule 15 - Treatment Planning SlideShow 080306ishtiiiNo ratings yet
- Mouth Breathing Habit: A ReviewDocument7 pagesMouth Breathing Habit: A ReviewMohamed FaizalNo ratings yet
- Gingival Inflammation in Mouth Breathing PatientsDocument5 pagesGingival Inflammation in Mouth Breathing PatientsCamiLunaNo ratings yet
- Upper Nasal AirwayDocument23 pagesUpper Nasal AirwayKapil ThakerNo ratings yet
- "Camouflage Treatment in Adenoid Facies: Long Face Syndrome"-A Case Report. - Orthodontic Cyber JouDocument11 pages"Camouflage Treatment in Adenoid Facies: Long Face Syndrome"-A Case Report. - Orthodontic Cyber Joudrrajesh27100% (1)