Squamous Cell Carcinoma
Squamous Cell Carcinoma
Download as pdf or txt
You might also like
- ECG .DR Ayalew EthiopiaDocument60 pagesECG .DR Ayalew EthiopiaAyalew Zewdie100% (2)
- 18 Colorectal Polyps and CarcinomaDocument89 pages18 Colorectal Polyps and Carcinomasuhaib ananzehNo ratings yet
- Squamous Cell CarcinomaDocument53 pagesSquamous Cell CarcinomaWacky BlankNo ratings yet
- Oral Squamous Cell Carcinoma (OSCC)Document37 pagesOral Squamous Cell Carcinoma (OSCC)Yusra Shaukat100% (1)
- Oral Cancer: Nader A. Al-AizariDocument51 pagesOral Cancer: Nader A. Al-AizariNader AlaizariNo ratings yet
- Head & Neck TumoursDocument15 pagesHead & Neck TumoursMalueth AnguiNo ratings yet
- Malignant MelanomaDocument29 pagesMalignant MelanomaHealth Education Library for People100% (2)
- Medicine2 - Complications of Cancer Treatment 2007Document76 pagesMedicine2 - Complications of Cancer Treatment 2007api-3762917No ratings yet
- Phyllodes Tumors of The Breast FINALDocument25 pagesPhyllodes Tumors of The Breast FINALchinnnababuNo ratings yet
- 1-Malignant Melanoma of The Oral Cavity A ReviewDocument3 pages1-Malignant Melanoma of The Oral Cavity A ReviewPaomo Zhixia EarlyNo ratings yet
- Principles of OncologyDocument26 pagesPrinciples of OncologyDr Shahzad Alam ShahNo ratings yet
- Cancer of The LarynxDocument16 pagesCancer of The Larynxhelaley_1983No ratings yet
- Oral CancerDocument6 pagesOral CancerGhege GuntaranNo ratings yet
- CancerDocument24 pagesCancerarshadmuhammedNo ratings yet
- Squamous Cell CarcinomaDocument12 pagesSquamous Cell CarcinomaA. Pathak0% (1)
- Oral Squamous Cell CarcinomaDocument10 pagesOral Squamous Cell CarcinomadeenmNo ratings yet
- Breast SurgeryDocument6 pagesBreast SurgeryDeedee Rocha100% (1)
- Oral Tumours: DR B M KalyanyamaDocument216 pagesOral Tumours: DR B M Kalyanyamafredrick damianNo ratings yet
- Principles of Surgical OncologyDocument34 pagesPrinciples of Surgical Oncologykaukab azim100% (1)
- Premalignant LesionsDocument76 pagesPremalignant LesionsPrima D Andri100% (1)
- MyxomaDocument36 pagesMyxomasgoeldoc_550661200No ratings yet
- Cancer of Oral CavityDocument27 pagesCancer of Oral CavityMihai AlexandruNo ratings yet
- Soft Tissue SarcomasDocument37 pagesSoft Tissue SarcomasHealth Education Library for People100% (1)
- Thyroid CancerDocument39 pagesThyroid CancerFaheem SarwarNo ratings yet
- MelanomaDocument14 pagesMelanomaMarco Antonio Koff100% (1)
- Salivary Gland TumorsDocument29 pagesSalivary Gland Tumorssajidali143No ratings yet
- Giant Cell Lesions of The Jaws: DR Syeda Noureen IqbalDocument61 pagesGiant Cell Lesions of The Jaws: DR Syeda Noureen IqbalMuhammad maaz khanNo ratings yet
- Papillary CarcinomaDocument7 pagesPapillary Carcinomarazik89No ratings yet
- TUMOR MARKER - ModulpptDocument30 pagesTUMOR MARKER - Modulpptnouval_iqbal100% (1)
- Salivary Gland TumorsDocument25 pagesSalivary Gland TumorsdrpnnreddyNo ratings yet
- Merged IncisionsDocument76 pagesMerged IncisionsJoshua MendozaNo ratings yet
- Rectal CarcinomaDocument16 pagesRectal Carcinomabuddy557No ratings yet
- Nursing Process OsteosarcomaDocument34 pagesNursing Process OsteosarcomaDonJohnNo ratings yet
- Surgery Papillary Thyroid CADocument15 pagesSurgery Papillary Thyroid CAMelissa LabadorNo ratings yet
- Module 6 Dr. AlbertoDocument10 pagesModule 6 Dr. AlbertoJASTHER LLOYD TOMANENGNo ratings yet
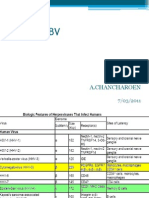
- CMV & Ebv: A.ChancharoenDocument59 pagesCMV & Ebv: A.ChancharoenRapid MedicineNo ratings yet
- 050 PPT - RetinoblastomaDocument61 pages050 PPT - RetinoblastomaAnastasia TjanNo ratings yet
- Orofacial Complications of Non Surgical Cancer TherapyDocument59 pagesOrofacial Complications of Non Surgical Cancer TherapyKassim OboghenaNo ratings yet
- Colorectal CancerDocument29 pagesColorectal CancerLeeyanBhadzzVagayNo ratings yet
- Treatment Algorithm For Ameloblastoma RRDocument30 pagesTreatment Algorithm For Ameloblastoma RRpanjidrgNo ratings yet
- Malignant Breast DiseasesDocument49 pagesMalignant Breast DiseasesEsha Bhatia100% (1)
- Colon PolypsDocument65 pagesColon PolypsorianattNo ratings yet
- Contemporary Treatment of AmeloblastomaDocument7 pagesContemporary Treatment of AmeloblastomaomeerulrafieNo ratings yet
- Crush Syndrome & Compartment Syndrome 2020Document45 pagesCrush Syndrome & Compartment Syndrome 2020Icha Marissa SofyanNo ratings yet
- Management of Thyroid CancerDocument57 pagesManagement of Thyroid CancerAshis SahaNo ratings yet
- Prostatic CancerDocument4 pagesProstatic CancerParixit DasNo ratings yet
- Oral Cancer: "The Forgotten Disease"Document16 pagesOral Cancer: "The Forgotten Disease"Amit KumarNo ratings yet
- Ewing SarcomaDocument4 pagesEwing SarcomaNurulAqilahZulkifliNo ratings yet
- 1) BiopsyDocument30 pages1) BiopsySosa GeorgeNo ratings yet
- Patho of Invasive Duct CarcinomaDocument3 pagesPatho of Invasive Duct CarcinomaBESA JERIC FLORESNo ratings yet
- Nasopharyngeal Cancer CompleteDocument54 pagesNasopharyngeal Cancer CompleteAmemonsajaah AmemonNo ratings yet
- Salivary Gland TumorDocument62 pagesSalivary Gland Tumordeepak kumarNo ratings yet
- Local and Regional Flaps-1Document89 pagesLocal and Regional Flaps-1Bilal Basit100% (1)
- Penile Cancer 2010Document28 pagesPenile Cancer 2010raghavagummadiNo ratings yet
- GenioplastyDocument11 pagesGenioplastyMohamed El-shorbagyNo ratings yet
- Cancer Prevention, Screening, & Early DetectionDocument13 pagesCancer Prevention, Screening, & Early Detectionchfalguera100% (1)
- Breast Cancer UpdatedDocument20 pagesBreast Cancer UpdatedHAZEL LEELA A P RICHARDNo ratings yet
- Necrotizing FasciitisDocument6 pagesNecrotizing FasciitisVirtues GracesNo ratings yet
- Thyroid CarcinomaDocument27 pagesThyroid CarcinomaGanesh MarutinathNo ratings yet
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Drug InventoryDocument1 pageDrug InventoryWacky BlankNo ratings yet
- MseDocument22 pagesMseWacky BlankNo ratings yet
- Neuro ReportingDocument32 pagesNeuro ReportingWacky BlankNo ratings yet
- Derma PaperDocument5 pagesDerma PaperWacky BlankNo ratings yet
- Chemotherapy PDFDocument16 pagesChemotherapy PDFbbdddNo ratings yet
- Research PapercapstoneDocument7 pagesResearch Papercapstoneapi-251518438No ratings yet
- Asma 2018Document3 pagesAsma 2018gheaNo ratings yet
- Pregnancy and LactationDocument62 pagesPregnancy and LactationFe Mina NisperosNo ratings yet
- World Pharma Market PDFDocument49 pagesWorld Pharma Market PDFCapitaine KrunchNo ratings yet
- Tumors of External and Middle EarDocument42 pagesTumors of External and Middle EarAmiteshwar SinghNo ratings yet
- Neurology Passmedicine & Onexamination Notes 2016Document158 pagesNeurology Passmedicine & Onexamination Notes 2016Muhammad Haneef100% (2)
- FadfdDocument5 pagesFadfdVanessa MeanaNo ratings yet
- Education Bureau Territory-Wide System Assessment 2019 Secondary 3 Mathematics Question BookletDocument20 pagesEducation Bureau Territory-Wide System Assessment 2019 Secondary 3 Mathematics Question BookletJake WongNo ratings yet
- Food Labels ExerciseDocument20 pagesFood Labels ExerciseAnonymous h2EnKyDbNo ratings yet
- Formulation and Evaluation of Time Dependendt Release of Montelukast Tablets by Using Mini Tablet TechnologyDocument13 pagesFormulation and Evaluation of Time Dependendt Release of Montelukast Tablets by Using Mini Tablet TechnologyBaru Chandrasekhar RaoNo ratings yet
- Everyday Practice:: Diabetes MellitusDocument6 pagesEveryday Practice:: Diabetes Mellitusailima2No ratings yet
- Amarin OrderDocument71 pagesAmarin OrderprofcgardenNo ratings yet
- Nursing Compilation of Questions June2019Document154 pagesNursing Compilation of Questions June2019Wani Zahoor50% (2)
- Noncardiogenic Pumonary EdemaDocument15 pagesNoncardiogenic Pumonary EdemaAnonymous OlS0WZwNo ratings yet
- The Pharma Innovation - Journal: Psidium Guajava A Fruit or Medicine - An OverviewDocument5 pagesThe Pharma Innovation - Journal: Psidium Guajava A Fruit or Medicine - An OverviewMuhammad Abdur RokhimNo ratings yet
- 1995 Mayis Kpds SorulariDocument15 pages1995 Mayis Kpds SorulariiskenderbeyNo ratings yet
- BS BuzzDocument8 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- Hematology and Oncology PDFDocument8 pagesHematology and Oncology PDFGuruyogendra MuthyalNo ratings yet
- CA Oral CavityDocument53 pagesCA Oral Cavityaakash11No ratings yet
- LactulozaDocument2 pagesLactulozaRaluca Elena Raluca ElenaNo ratings yet
- Examining The PrecordiumDocument83 pagesExamining The PrecordiumnicolNo ratings yet
- The Clinical Use of Drugs. Lippincott Williams & Wilkins Pennsylvania, United StatesDocument4 pagesThe Clinical Use of Drugs. Lippincott Williams & Wilkins Pennsylvania, United StatesshaniNo ratings yet
- Best Practice & Research Clinical RheumatologyDocument15 pagesBest Practice & Research Clinical RheumatologyTatiana GonzalezNo ratings yet
- BONE SCAN PPT NewDocument19 pagesBONE SCAN PPT Newdrgurpal740% (1)
- Pathophysiology of Variceal Bleeding in CirrhoticsDocument8 pagesPathophysiology of Variceal Bleeding in Cirrhoticsanon_914506742No ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakadevyhandayaniNo ratings yet
- Au Di Minor Case Study Myasthenia GravisDocument17 pagesAu Di Minor Case Study Myasthenia Gravisapi-301816885No ratings yet
- Study Links Accelerated Aging To Cancer Risk in Younger Adults - CNNDocument11 pagesStudy Links Accelerated Aging To Cancer Risk in Younger Adults - CNNspapazian1No ratings yet