Policy Phlebotomy Blood Collection
Policy Phlebotomy Blood Collection
Download as pdf or txt
You might also like
- GEHC Revolution Maxima BrochureDocument16 pagesGEHC Revolution Maxima Brochureardyanto florensius100% (1)
- Laboratory General Sep07Document130 pagesLaboratory General Sep07Marta TozziNo ratings yet
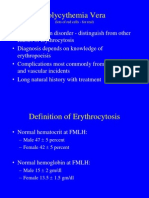
- PolycythemiaDocument22 pagesPolycythemiaIrman DinejadNo ratings yet
- Health Privacy Issues For ResearchersDocument20 pagesHealth Privacy Issues For ResearchersVanessa ZuletaNo ratings yet
- Chapter OneDocument53 pagesChapter OnemustangsarahNo ratings yet
- 25 Phlebotomy ProcedureDocument10 pages25 Phlebotomy ProcedureMichael TaylorNo ratings yet
- Statement of Deficiencies and Plan of Correction For Andbe Home (Via DHHS)Document12 pagesStatement of Deficiencies and Plan of Correction For Andbe Home (Via DHHS)NTV NewsNo ratings yet
- 3 - Poster Phlebotomy Workshop-1Document1 page3 - Poster Phlebotomy Workshop-1muhammadhanifmohdfahmiNo ratings yet
- Interview QuestionsDocument10 pagesInterview Questionskumarvicky228No ratings yet
- Feb 2022 Compliance ReportDocument62 pagesFeb 2022 Compliance ReportThe TexanNo ratings yet
- PHB Lec 1 Phlebotomy and The Health Care Setting Part 1Document42 pagesPHB Lec 1 Phlebotomy and The Health Care Setting Part 1Jean KenNo ratings yet
- Phlebotomy 1. Requisition FormDocument7 pagesPhlebotomy 1. Requisition FormRicci Anne B. MelgarNo ratings yet
- Critical Care/ICU NurseDocument2 pagesCritical Care/ICU Nurseapi-78203561No ratings yet
- 12-13 Handbook School of Medical TechnologyDocument41 pages12-13 Handbook School of Medical TechnologyPeter SewehaNo ratings yet
- Medical Terminology Information SheetDocument3 pagesMedical Terminology Information SheetNanami MomozonoNo ratings yet
- Medical Laboratory NotesDocument5 pagesMedical Laboratory NotesDinesh KumarNo ratings yet
- Medical Terminology Part 1Document35 pagesMedical Terminology Part 1B-094. Dwi PurwatiNo ratings yet
- Phlebotomy Worktext and Procedures Manual 4th Edition PDFDocument26 pagesPhlebotomy Worktext and Procedures Manual 4th Edition PDFxakeh24420No ratings yet
- Diploma in Medical Lab Technician Course SyllabusDocument29 pagesDiploma in Medical Lab Technician Course SyllabusMohanbabu DivotsNo ratings yet
- Models of CounsellingDocument48 pagesModels of Counsellingrumi royNo ratings yet
- Post Operative Bedside Thoracic Surgery 2018Document7 pagesPost Operative Bedside Thoracic Surgery 2018Devi SiswaniNo ratings yet
- Syllabus Syllabus Syllabus: Last Revised: 8/1/2020 7:04 A8/p8Document22 pagesSyllabus Syllabus Syllabus: Last Revised: 8/1/2020 7:04 A8/p8KweenPin AsiaNo ratings yet
- Postal Exam TipsDocument23 pagesPostal Exam TipsShay EllisNo ratings yet
- Paper Cuts: Reducing Health Care Administrative CostsDocument48 pagesPaper Cuts: Reducing Health Care Administrative CostsCenter for American ProgressNo ratings yet
- Long Term Care Monitoring Tools: Resident Meal Time and Dining Experience Kitchen and Food ServiceFrom EverandLong Term Care Monitoring Tools: Resident Meal Time and Dining Experience Kitchen and Food ServiceNo ratings yet
- Certification in PhlebotomyDocument2 pagesCertification in PhlebotomyBrian KingNo ratings yet
- CCMA EXAM OutlineDocument3 pagesCCMA EXAM OutlineReanna50% (2)
- Phlebotomy Handbook REVISEDDocument41 pagesPhlebotomy Handbook REVISEDAna mariaNo ratings yet
- Medical AssistantDocument1 pageMedical AssistantMLastTryNo ratings yet
- Introduction To Clinical HematologyDocument42 pagesIntroduction To Clinical HematologyBishoy GalalNo ratings yet
- Medical Technology: (1) History of The Medical Laboratory ScienceDocument63 pagesMedical Technology: (1) History of The Medical Laboratory ScienceJAKE DANGPASONNo ratings yet
- The Different Types of Sample Tubes Used in PhlebotomyDocument2 pagesThe Different Types of Sample Tubes Used in PhlebotomyAminu HassanNo ratings yet
- %igv Tipo Precio X Kilo %arancel: TotalDocument14 pages%igv Tipo Precio X Kilo %arancel: TotalPaul Ccana0% (1)
- Tietz Fundamentals of Clinical Chemistry and Molecular Diagnostics 7th Edition Carl A. Burtis All Chapter Instant DownloadDocument52 pagesTietz Fundamentals of Clinical Chemistry and Molecular Diagnostics 7th Edition Carl A. Burtis All Chapter Instant Downloadmakhaobram100% (3)
- NMC Code of Conduct PDFDocument5 pagesNMC Code of Conduct PDFico_isNo ratings yet
- 2 PhlebotomyDocument102 pages2 PhlebotomyCatherine Merilleno100% (1)
- Evidence-Based HematologyFrom EverandEvidence-Based HematologyMark A. CrowtherNo ratings yet
- Phlebotomy in A NutshellDocument131 pagesPhlebotomy in A Nutshellgreen_archerNo ratings yet
- Textbook of Urgent Care Management: Chapter 33, EMTALA in Urgent Care MedicineFrom EverandTextbook of Urgent Care Management: Chapter 33, EMTALA in Urgent Care MedicineNo ratings yet
- Management of Chronic WoundsDocument20 pagesManagement of Chronic WoundsRia SukmaNo ratings yet
- Blood Transfusion GuidelineDocument402 pagesBlood Transfusion GuidelineAdam Razi0% (1)
- Textbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationFrom EverandTextbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationNo ratings yet
- How To Understand Medical TerminologyDocument37 pagesHow To Understand Medical TerminologyKai MeNo ratings yet
- AMCA Study Guide For EKGDocument24 pagesAMCA Study Guide For EKGFernando AlmaguerNo ratings yet
- Casac TDocument1 pageCasac Tapi-121403262No ratings yet
- Radiology Code ListDocument2 pagesRadiology Code Listtimvrghs123No ratings yet
- Safe Blood: Purifying the Nations Blood Supply in the Age of AFrom EverandSafe Blood: Purifying the Nations Blood Supply in the Age of ANo ratings yet
- MayoTestCatalog Rochester SortedByTestName Duplex InterpretiveDocument2,763 pagesMayoTestCatalog Rochester SortedByTestName Duplex InterpretiveLaboratorium RS BELLANo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Metabolism of Proteins: Dr. Lotfi S. Bin Dahman M.D. Ph.D. Clinical Biochemistry HucomDocument27 pagesMetabolism of Proteins: Dr. Lotfi S. Bin Dahman M.D. Ph.D. Clinical Biochemistry HucomHUAWEI HUAWEINo ratings yet
- Clinical Procedures For Medical AssistantDocument40 pagesClinical Procedures For Medical AssistantStudent1010No ratings yet
- The Clinical LaboratoryDocument24 pagesThe Clinical LaboratoryRomar Durian100% (2)
- COLLECTION OF BLOOD SPECIMENS MANUAL 2018-2020 - For Lab Guide PDFDocument27 pagesCOLLECTION OF BLOOD SPECIMENS MANUAL 2018-2020 - For Lab Guide PDFGonzalez ArturoNo ratings yet
- A Comprehensive Text Book on Self-emulsifying Drug Delivery SystemsFrom EverandA Comprehensive Text Book on Self-emulsifying Drug Delivery SystemsNo ratings yet
- PATHOPHYSIOLOGY LAB - Hanbook of Pathophysiology SevastreDocument192 pagesPATHOPHYSIOLOGY LAB - Hanbook of Pathophysiology Sevastredorina0101No ratings yet
- Chapter 2: Assessments For The Resident Assessment Instrument (Rai)Document69 pagesChapter 2: Assessments For The Resident Assessment Instrument (Rai)Eva100% (1)
- Textbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordFrom EverandTextbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordNo ratings yet
- Utilization Review RNDocument2 pagesUtilization Review RNapi-121451258No ratings yet
- Nursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationDocument4 pagesNursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationCharlene Jacobe Cornista100% (1)
- Leukemias: Principles and Practice of TherapyFrom EverandLeukemias: Principles and Practice of TherapyStefan FaderlNo ratings yet
- Topic 1 PDFDocument18 pagesTopic 1 PDFmuhammadhanifmohdfahmiNo ratings yet
- Prepositions of Time (At - in - On) - Print - QuizizzDocument4 pagesPrepositions of Time (At - in - On) - Print - QuizizzmuhammadhanifmohdfahmiNo ratings yet
- Trizol InfographicsDocument1 pageTrizol InfographicsmuhammadhanifmohdfahmiNo ratings yet
- Laisal GhareebDocument4 pagesLaisal GhareebmuhammadhanifmohdfahmiNo ratings yet
- 10 Tips For Reviewing Scientific Manuscripts - and 5 Red FlagsDocument2 pages10 Tips For Reviewing Scientific Manuscripts - and 5 Red FlagsmuhammadhanifmohdfahmiNo ratings yet
- Hemolysis in Serum Samples Drawn by Emergency Department Personnel Versus Laboratory PhlebotomistsDocument3 pagesHemolysis in Serum Samples Drawn by Emergency Department Personnel Versus Laboratory PhlebotomistsmuhammadhanifmohdfahmiNo ratings yet
- Participant: Parking Lot Beside Fsk6 BuildingDocument1 pageParticipant: Parking Lot Beside Fsk6 BuildingmuhammadhanifmohdfahmiNo ratings yet
- Purdue Owl - Apa StyleDocument53 pagesPurdue Owl - Apa StylemuhammadhanifmohdfahmiNo ratings yet
- Hub ColourDocument1 pageHub ColourmuhammadhanifmohdfahmiNo ratings yet
- Final Ichase17 Tentative ProgrammeDocument1 pageFinal Ichase17 Tentative ProgrammemuhammadhanifmohdfahmiNo ratings yet
- Bad Breath - What To Do About It - Health Powered KidsDocument4 pagesBad Breath - What To Do About It - Health Powered KidsRena PollardNo ratings yet
- Atividade Inglês InstrumentalDocument5 pagesAtividade Inglês InstrumentalMaria SampaioNo ratings yet
- Steroid Tapering and Supportive Treatment Guidance V1.0Document1 pageSteroid Tapering and Supportive Treatment Guidance V1.0Dr. Prasanna DahalNo ratings yet
- FOUR Score Coma ScaleDocument32 pagesFOUR Score Coma ScaleAndriawan BramNo ratings yet
- Cap 1 EndoDocument33 pagesCap 1 EndoDaniela SosaNo ratings yet
- New Drug Approval From Cdsco Till DateDocument5 pagesNew Drug Approval From Cdsco Till DateAshish1pharmaNo ratings yet
- Yuvraj Kumar Male18 Years 90294Document1 pageYuvraj Kumar Male18 Years 90294Anjali KumariNo ratings yet
- Ludwig's Angina MCQSDocument3 pagesLudwig's Angina MCQSdr arshadNo ratings yet
- Reyes Vs Sisters of Mercy HospitalDocument11 pagesReyes Vs Sisters of Mercy HospitalJenNo ratings yet
- L3 Patho Cell Response To Injury 2 (Basic of Disease)Document27 pagesL3 Patho Cell Response To Injury 2 (Basic of Disease)mohamedelkomy4400No ratings yet
- Sphingomonas KoreensisDocument11 pagesSphingomonas KoreensisSMIBA MedicinaNo ratings yet
- 1 in 10 Infants Worldwide Did Not Receive Any Vaccinations in 2016Document2 pages1 in 10 Infants Worldwide Did Not Receive Any Vaccinations in 2016YennyIrdayaniNasutionNo ratings yet
- Tranexamic Acid in Gynaecology & ObstetricDocument26 pagesTranexamic Acid in Gynaecology & ObstetricsivaNo ratings yet
- Psychiatry Questions - Combined All Previous Year QuestionsDocument33 pagesPsychiatry Questions - Combined All Previous Year QuestionsDivyashree Venkatesh100% (2)
- Aorn 12784Document10 pagesAorn 12784Yahia HassaanNo ratings yet
- Exchange Transfusion Guidelines 2019Document8 pagesExchange Transfusion Guidelines 2019Dr AhmedNo ratings yet
- Chronische Mudigkeit 2020 Klinghardt MüdigkeitDocument99 pagesChronische Mudigkeit 2020 Klinghardt Müdigkeitzim1dsgvo.ruNo ratings yet
- Educating Preeclampsia Management Using Case Studies of Disease PDocument30 pagesEducating Preeclampsia Management Using Case Studies of Disease PANUM NOORINo ratings yet
- Screening Checklist For Contraindications AdultsDocument1 pageScreening Checklist For Contraindications AdultsEduardo VelásquezNo ratings yet
- Biosafety ReduxDocument625 pagesBiosafety ReduxHasna MazidahNo ratings yet
- Canine Distemper Virus - FinalDocument17 pagesCanine Distemper Virus - FinalikliptikawatiNo ratings yet
- Chalazion and Hordeolum (Stye) - Eye Disorders - Merck Manuals Professional EditionDocument3 pagesChalazion and Hordeolum (Stye) - Eye Disorders - Merck Manuals Professional EditionAlfina MeidinaNo ratings yet
- Ballengers Manual of Otorhinolaryngology PDFDocument858 pagesBallengers Manual of Otorhinolaryngology PDFIrma Sari Muliadi100% (1)
- Lucknow Apollohospitals Com Mayank Somani HTMLDocument2 pagesLucknow Apollohospitals Com Mayank Somani HTMLEndocrinologist in lucknowNo ratings yet
- Traditional Treatment: Nur Jannatul Naimah Binti ZainalabidinDocument12 pagesTraditional Treatment: Nur Jannatul Naimah Binti ZainalabidinSnexon Jajan MariaNo ratings yet
- Health Assessment: Nursing ProcessDocument7 pagesHealth Assessment: Nursing ProcessAngelrica TumbadoNo ratings yet
- Practice: Pituitary AdenomasDocument7 pagesPractice: Pituitary AdenomasujiNo ratings yet
- Cadcam0213 PDFDocument52 pagesCadcam0213 PDFclaudia360100% (1)
- Surgical Drains Catheters and Tubes (M)Document120 pagesSurgical Drains Catheters and Tubes (M)nikprov100% (7)