Neural Mobilization
Neural Mobilization
Download as pdf or txt
You might also like
- 04 - 20210720 SopgDocument270 pages04 - 20210720 SopgNick Reithmaier100% (2)
- Mpeh Grade8 Pre-TestDocument3 pagesMpeh Grade8 Pre-TestElmie Valencia-Cuachon77% (53)
- Cyriax IntroDocument14 pagesCyriax IntrodrrajmptnNo ratings yet
- 1 Peripheral Manipulation Lecture OneDocument13 pages1 Peripheral Manipulation Lecture Onebuhlembatha304No ratings yet
- Kalternborn Joint Mobilization-3Document36 pagesKalternborn Joint Mobilization-3jayadevanNo ratings yet
- Joint Mobilization To The Elbow, Wrist and Hand2Document43 pagesJoint Mobilization To The Elbow, Wrist and Hand2Tripty Khanna Karwal100% (1)
- Bobath ApprochDocument2 pagesBobath ApprochRùpám KanungoNo ratings yet
- 14 Biomechanics of Normal Human Gait PDFDocument26 pages14 Biomechanics of Normal Human Gait PDFDiego A. MezaNo ratings yet
- Muhammed Kocabiyik Physical Medicine & Rehabilitation Iv. Class V. GroupDocument14 pagesMuhammed Kocabiyik Physical Medicine & Rehabilitation Iv. Class V. GroupsanalcrazyNo ratings yet
- BY Dr. Amrit Kaur (PT) Lecturer, N.D.M.V.P College of Physiotherapy NashikDocument70 pagesBY Dr. Amrit Kaur (PT) Lecturer, N.D.M.V.P College of Physiotherapy Nashikmd jawedNo ratings yet
- ACL Reconstruction Rehabilitation ProtocolDocument11 pagesACL Reconstruction Rehabilitation ProtocolNijin XmxNo ratings yet
- Physiotherapy in Disaster MenegementDocument82 pagesPhysiotherapy in Disaster MenegementAtiKa YuLiantiNo ratings yet
- Do Sliders' Slide and Tensioners' Tension An Analysis of Neurodynamic Techniques and Considerations Regarding Their Application PDFDocument9 pagesDo Sliders' Slide and Tensioners' Tension An Analysis of Neurodynamic Techniques and Considerations Regarding Their Application PDFryanbroad82No ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- Pathomechanics of Knee JointDocument55 pagesPathomechanics of Knee JointAkhila SudheerbabuNo ratings yet
- PNFDocument12 pagesPNFKanika KakkarNo ratings yet
- Dysphagia ManagementDocument21 pagesDysphagia ManagementSooraj A. O.100% (1)
- Mulligan MobilizationDocument70 pagesMulligan MobilizationjayadevanNo ratings yet
- Brunnstrom ApproachDocument32 pagesBrunnstrom ApproachTalha ParkarNo ratings yet
- Biomechanics of PostureDocument12 pagesBiomechanics of PostureMariana PachecoNo ratings yet
- Brunnstrom ApproachDocument33 pagesBrunnstrom ApproachAISHWARYA SWAMINATHANNo ratings yet
- MUHS - BPT - 2017 - 4 - Winter - B.P.TH - 51411 Musculoskeletal PhysiotherapyDocument2 pagesMUHS - BPT - 2017 - 4 - Winter - B.P.TH - 51411 Musculoskeletal PhysiotherapyYuvraj AtholeNo ratings yet
- A Proposed Evidence-Based Shoulder Special Testing Examination Algorithm - Clinical Utility Based On A Systematic Review of The LiteratureDocument14 pagesA Proposed Evidence-Based Shoulder Special Testing Examination Algorithm - Clinical Utility Based On A Systematic Review of The LiteratureAfonso MacedoNo ratings yet
- Physiotherapy Technician - CTS - NSQF-4Document41 pagesPhysiotherapy Technician - CTS - NSQF-4gaurav kumar100% (1)
- Introduction To The Mulligan ConceptDocument6 pagesIntroduction To The Mulligan ConceptPrima Krishna DharmawanNo ratings yet
- PNF For Lower LimbDocument22 pagesPNF For Lower LimbsanalcrazyNo ratings yet
- Proprioceptive Neuromuscular Facilitation (PNF)Document76 pagesProprioceptive Neuromuscular Facilitation (PNF)Hasan KhawaldehNo ratings yet
- Concepts of Management in MSK DisordersDocument25 pagesConcepts of Management in MSK DisordersIzzaAyub100% (1)
- Anatomy and Pathoanatomic of Lumbosacral PlexusDocument33 pagesAnatomy and Pathoanatomic of Lumbosacral PlexusRachmad FaisalNo ratings yet
- Physiotherapy For PoliomyelitisDocument16 pagesPhysiotherapy For Poliomyelitisabdalsucs100% (1)
- Hip Biomechanics SRSDocument119 pagesHip Biomechanics SRSSreeraj S RNo ratings yet
- Muscle Re-Education: BY DR - Eswar Kolli, MPTDocument42 pagesMuscle Re-Education: BY DR - Eswar Kolli, MPTShubha Diwakar100% (1)
- Kaltenborn 1993Document5 pagesKaltenborn 1993hari vijayNo ratings yet
- Pathomechanics of Acromioclavicular JointDocument28 pagesPathomechanics of Acromioclavicular JointMuhib ArfinNo ratings yet
- M7 Neurodynamic Mobility and Neural Tension TestDocument36 pagesM7 Neurodynamic Mobility and Neural Tension TestSylvia LoongNo ratings yet
- Peripheral Joint MobilizationDocument20 pagesPeripheral Joint MobilizationLove_dove612100% (1)
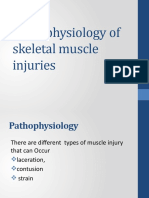
- Pathophysiology of Skeletal Muscle InjuriesDocument32 pagesPathophysiology of Skeletal Muscle InjuriesZaroon Abdullah Khan100% (1)
- Positional Release Technique: Dr. Nistara S. Chawla Miap, CSTMT MPT NeurologyDocument25 pagesPositional Release Technique: Dr. Nistara S. Chawla Miap, CSTMT MPT NeurologyNistara Singh ChawlaNo ratings yet
- Suspension TherapyDocument52 pagesSuspension TherapyROJA MACHERLA0% (1)
- Physiotherapy Pain CareDocument3 pagesPhysiotherapy Pain CareMuhammad Aurangzeb FahimNo ratings yet
- 7 FUP 2020 EditedDocument15 pages7 FUP 2020 EditedZayn100% (1)
- CRICKET SKILLS INJURY (PPT For Assignment) LnipeDocument59 pagesCRICKET SKILLS INJURY (PPT For Assignment) LnipeVinod Baitha (Vinod Sir)No ratings yet
- TapingDocument9 pagesTapingim. EliasNo ratings yet
- Chris Littlewood - Stephen May - Understanding Physiotherapy Research-Cambridge Scholars Publishing (2013)Document136 pagesChris Littlewood - Stephen May - Understanding Physiotherapy Research-Cambridge Scholars Publishing (2013)Aya KhalilNo ratings yet
- Faradic CurrentDocument4 pagesFaradic CurrentNamrathaThalatoti ywSSAmHsULNo ratings yet
- The Convex Concave Rule and The Lever LawDocument4 pagesThe Convex Concave Rule and The Lever LawOwais KhanNo ratings yet
- GONIOMETRYDocument28 pagesGONIOMETRYnn2dgdypkcNo ratings yet
- Roods ApprochDocument59 pagesRoods Approchsridhar_physioNo ratings yet
- PhysiotherapydfsfDocument21 pagesPhysiotherapydfsfsaadbinsadaqat123456No ratings yet
- High Ankle SprainDocument6 pagesHigh Ankle SprainJesusNavarrete97No ratings yet
- Self-Mobilizations of Hip Belting TechniquesDocument16 pagesSelf-Mobilizations of Hip Belting TechniquesIrsan MonroNo ratings yet
- 3 Advantage of Free Ex 3Document13 pages3 Advantage of Free Ex 3Farrukh ShahzadNo ratings yet
- McKenzie CONCEPT AnilDocument12 pagesMcKenzie CONCEPT AnilSOUMYADEEP BHUINYANo ratings yet
- Manual Muscle Test (MMT) : Prepared By: DR - Rahul Chhatlani MPT (Neuro)Document80 pagesManual Muscle Test (MMT) : Prepared By: DR - Rahul Chhatlani MPT (Neuro)Rahul ChhatlaniNo ratings yet
- Manual Muscle Test For Upper Limb MusclesDocument17 pagesManual Muscle Test For Upper Limb MusclesDr Ahmed NabilNo ratings yet
- How Manipulation WorksDocument5 pagesHow Manipulation WorksRajeev TiwariNo ratings yet
- Advances in Spinal Stabilization PDFDocument333 pagesAdvances in Spinal Stabilization PDFMateo CortesNo ratings yet
- Prescription Principle of KAFODocument54 pagesPrescription Principle of KAFOFERYANDA UTAMI100% (1)
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Unlocking Pathways of Pain: Stories of Innovative Treatments and How They WorkFrom EverandUnlocking Pathways of Pain: Stories of Innovative Treatments and How They WorkNo ratings yet
- Review of Trial Therapies and Treatment For COVID-19: Lessons For IndonesiaDocument6 pagesReview of Trial Therapies and Treatment For COVID-19: Lessons For IndonesiaAri SudarsonoNo ratings yet
- Jospt 1984 5 6 348 PDFDocument25 pagesJospt 1984 5 6 348 PDFAri SudarsonoNo ratings yet
- SOAP Injury Evaluation Form PDFDocument2 pagesSOAP Injury Evaluation Form PDFAri SudarsonoNo ratings yet
- Algoritma Neck PainDocument12 pagesAlgoritma Neck PainAri SudarsonoNo ratings yet
- Pelatihan Dry NeedleDocument101 pagesPelatihan Dry NeedleAri SudarsonoNo ratings yet
- Professor of Anatomy Dept. of Biomedical Sciences Heritage College of Osteopathic Medicine, Ohio University Athens, Ohio 45701 Witmerl@Ohio - EduDocument20 pagesProfessor of Anatomy Dept. of Biomedical Sciences Heritage College of Osteopathic Medicine, Ohio University Athens, Ohio 45701 Witmerl@Ohio - EduAri SudarsonoNo ratings yet
- Cervical RadiculopathyDocument36 pagesCervical RadiculopathyAri SudarsonoNo ratings yet
- TMJDocument33 pagesTMJMohamed Magdy El Meligie100% (2)
- Bandaging in LymphodemaDocument19 pagesBandaging in LymphodemaAri SudarsonoNo ratings yet
- Introduction To PhysiotherapyDocument34 pagesIntroduction To PhysiotherapyAri Sudarsono100% (1)
- The Fundamentals of PNFDocument5 pagesThe Fundamentals of PNFAri SudarsonoNo ratings yet
- Leopold's Maneuver SCRPTDocument1 pageLeopold's Maneuver SCRPTDarwin QuirimitNo ratings yet
- Questionnaire On Stress Management - Google FormsDocument9 pagesQuestionnaire On Stress Management - Google FormsHimanshu JoshiNo ratings yet
- Cholesterol ARC CHEMDocument8 pagesCholesterol ARC CHEMSalah AnamNo ratings yet
- (ACV-S08) Week 08 - Pre-Task - Quiz - Weekly Quiz (PA) - INGLES IV (10354)Document5 pages(ACV-S08) Week 08 - Pre-Task - Quiz - Weekly Quiz (PA) - INGLES IV (10354)Rosendo Salas YanquiNo ratings yet
- Health Care Cover LetterDocument7 pagesHealth Care Cover Letterguv0k1jemen3100% (2)
- Caregivers Application FormDocument8 pagesCaregivers Application FormKumah WisdomNo ratings yet
- Travel Characteristics of Older and Disaled People in The Colombo DistrictDocument4 pagesTravel Characteristics of Older and Disaled People in The Colombo DistrictShan BasnayakeNo ratings yet
- Case 8 ОкDocument4 pagesCase 8 ОкАбдул Насер МохаммадізмаелNo ratings yet
- Rehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbaruDocument27 pagesRehabilitasi Post Op Spine Surgery: Kobal Sangaji Dokter Spesialis Rehabilitasi Medik RS Awalbros PekanbarukurniaNo ratings yet
- International Islamic University Islamabad: 1.1.1.1 Final Year Project ProposalDocument9 pagesInternational Islamic University Islamabad: 1.1.1.1 Final Year Project ProposalAtif SadiqNo ratings yet
- Essential Components of Palliative CareDocument20 pagesEssential Components of Palliative CareJonah R. Merano60% (5)
- Module 12 of Child and Adolescence DevelopmentDocument3 pagesModule 12 of Child and Adolescence DevelopmentMakki Andre Antonio75% (4)
- Play Therapy With TeenagersDocument21 pagesPlay Therapy With TeenagersRochelle HenekeNo ratings yet
- Growth PredictionDocument101 pagesGrowth PredictionKristty Magallanes100% (1)
- JesafinalDocument50 pagesJesafinalMay BatilaranNo ratings yet
- Fire and Earthquake SymposiumDocument2 pagesFire and Earthquake Symposiumirinakayla27No ratings yet
- Annex F - SOP For Warehouse and Inventory Management in UNHCRDocument38 pagesAnnex F - SOP For Warehouse and Inventory Management in UNHCRWilliam LeungNo ratings yet
- Bohol Water and Sanitation Project - PPP CenterDocument8 pagesBohol Water and Sanitation Project - PPP CenterFaux LexieNo ratings yet
- Cervicothoracic ExamDocument1 pageCervicothoracic ExamGustavo AcauanNo ratings yet
- Assessment On The Home Based Care and Support Programme For Infected and Affected People With Hiv Aids in NigeriaDocument46 pagesAssessment On The Home Based Care and Support Programme For Infected and Affected People With Hiv Aids in Nigeriajamessabraham2No ratings yet
- MG04-Rev 0Document28 pagesMG04-Rev 0saifNo ratings yet
- HOW To ZENDOODLE - Imagination, Creativity and Meditation Through Tangle Patterns and Designs! Ling, Zentangle, Creativity, Art of Zendoodle, Intervention, Meditation) - Abby Olivia CollinsDocument29 pagesHOW To ZENDOODLE - Imagination, Creativity and Meditation Through Tangle Patterns and Designs! Ling, Zentangle, Creativity, Art of Zendoodle, Intervention, Meditation) - Abby Olivia CollinsIsaBel43% (14)
- DBA0AE07-4F0D-47BF-9BF3-C06E311F21E3Document3 pagesDBA0AE07-4F0D-47BF-9BF3-C06E311F21E3Setiawan Dwi HandoyoNo ratings yet
- History of PainDocument25 pagesHistory of Paingabitor100% (1)
- Workout App Research PaperDocument5 pagesWorkout App Research PaperVA ClashersNo ratings yet
- Counseling TheoryDocument9 pagesCounseling Theoryapi-273583647No ratings yet
- Candida Grande KegelDocument5 pagesCandida Grande KegelCandy KegelNo ratings yet
- Three Days To See (Excerpts)Document2 pagesThree Days To See (Excerpts)Yan ShengNo ratings yet