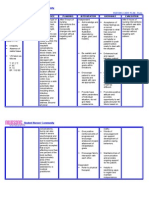
Brain Tumor
Brain Tumor
Download as docx, pdf, or txt
You might also like
- Ebook Facilitation Techniques in Therapeutic Recreation 3Rd Edition John Dattilo Alexis Mckenney Online PDF All ChapterDocument69 pagesEbook Facilitation Techniques in Therapeutic Recreation 3Rd Edition John Dattilo Alexis Mckenney Online PDF All Chapterannetta.velez139100% (10)
- Care Plan 5Document13 pagesCare Plan 5مالك مناصرة100% (2)
- Francisco VarelaDocument5 pagesFrancisco Varelahatdog adadaNo ratings yet
- Spinal Injury Nursing Care PlanDocument2 pagesSpinal Injury Nursing Care PlanPatricia OrtegaNo ratings yet
- Nursing Care Plan-AscitesDocument10 pagesNursing Care Plan-AscitesKayki Louise75% (4)
- Nursing Care Plan For The Patient With Burn Injury - Acute Pain Related To Tissue and Nerve InjuryDocument2 pagesNursing Care Plan For The Patient With Burn Injury - Acute Pain Related To Tissue and Nerve InjuryAngel Garcia67% (3)
- Nursing Care Plan - BurnDocument2 pagesNursing Care Plan - Burnderic90% (10)
- Nursing Care Plan Hemorrhagic StrokeDocument8 pagesNursing Care Plan Hemorrhagic StrokeJeffrey Dela Cruz50% (4)
- NCPDocument1 pageNCPhaniehaehae100% (1)
- Myocarditis NCP 2Document8 pagesMyocarditis NCP 2astro_aaron117375% (4)
- CVA NCP Ineffective Airway ClearanceDocument2 pagesCVA NCP Ineffective Airway ClearanceJoanne Kaye Taylor100% (1)
- Craniotomy Nursing Care PlanDocument5 pagesCraniotomy Nursing Care PlanJordz Placi100% (2)
- Nursing Care PlanDocument3 pagesNursing Care PlanKwini Jeyn50% (2)
- NCP - Patient With Chest TubeDocument2 pagesNCP - Patient With Chest TubeSelwynVillamorPatente0% (1)
- Anxiety Related To Hospitalization and Disease Condition As Manifested by Fiscal Expression and VerbalizationDocument2 pagesAnxiety Related To Hospitalization and Disease Condition As Manifested by Fiscal Expression and VerbalizationmonaNo ratings yet
- Aneurysm NCPDocument4 pagesAneurysm NCPAnneUXD100% (1)
- NCP GbsDocument2 pagesNCP GbsJaylord VerazonNo ratings yet
- NCP FVDDocument2 pagesNCP FVDMarlon AnryNo ratings yet
- Nursing Care Plan SeizureDocument2 pagesNursing Care Plan Seizuretimie_reyes100% (1)
- Nursing Care Plan 1Document4 pagesNursing Care Plan 1Johndelle Banlasan Hernan100% (1)
- NCPDocument2 pagesNCPJhel NabosNo ratings yet
- NCP Heart BlockDocument3 pagesNCP Heart BlockEköw Santiago Javier60% (5)
- Nursing Diagnosis Care Plan HyponitremiaDocument2 pagesNursing Diagnosis Care Plan HyponitremiaAbdallah AlasalNo ratings yet
- NCP Epidural HemDocument32 pagesNCP Epidural HemKatrina PonceNo ratings yet
- Risk For InfectionDocument3 pagesRisk For Infectioncamziii100% (1)
- NCP - Ineffective Cerebral Tissue Perfusion R/T Space Occupying Lesion (Neuroblastoma On Frontal Lobe)Document4 pagesNCP - Ineffective Cerebral Tissue Perfusion R/T Space Occupying Lesion (Neuroblastoma On Frontal Lobe)Carl Elexer Cuyugan Ano100% (4)
- NCP Cataract SurgeryDocument5 pagesNCP Cataract SurgeryKristaJaneCelmarBagcatNo ratings yet
- Nanda NCP BasedDocument14 pagesNanda NCP Baseddeliejoyce100% (1)
- Breast Ca NCPDocument3 pagesBreast Ca NCPThirdy AquinoNo ratings yet
- Nursing Care Plan HyperthyroidismDocument2 pagesNursing Care Plan HyperthyroidismAbdallah Alasal0% (1)
- NCP AneurysmDocument4 pagesNCP AneurysmJanielle Christine Monsalud100% (1)
- Stroke Nursing Care PlanDocument1 pageStroke Nursing Care PlanTracy Pearl100% (1)
- Nursing Care Plan Ineffective Breathing Pattern Hepatic MassDocument2 pagesNursing Care Plan Ineffective Breathing Pattern Hepatic MassRheegell Ellar-Fuertes100% (3)
- Iii. Nursing Care PlansDocument13 pagesIii. Nursing Care PlansLharra Cagulada-Postrano100% (1)
- Drug NameDocument4 pagesDrug Namecheanne003No ratings yet
- BibliographyDocument2 pagesBibliographyMahesh T Madhavan100% (1)
- Nursing Care Plan For Patiients With MeningitisDocument35 pagesNursing Care Plan For Patiients With Meningitisixa_morales67% (6)
- FHP & NCP - FractureDocument14 pagesFHP & NCP - FractureFrancis AdrianNo ratings yet
- Impaired Oral Mucous Membranes - NCPDocument2 pagesImpaired Oral Mucous Membranes - NCPXtianna Jade Doquila100% (1)
- Patient With Neutropenia Risk For Infection Related To Inadequate Secondary Defenses (Leukopenia, Neutropenia), Altered Response To MicrobialDocument2 pagesPatient With Neutropenia Risk For Infection Related To Inadequate Secondary Defenses (Leukopenia, Neutropenia), Altered Response To MicrobialICa MarlinaNo ratings yet
- Nursing Care Plan: Subjective DataDocument4 pagesNursing Care Plan: Subjective DataAbdallah AlasalNo ratings yet
- Diabetes Mellitus (DM)Document1 pageDiabetes Mellitus (DM)Bheru LalNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationJamie Haravata0% (1)
- NCPDocument2 pagesNCPJamaica SaranquinNo ratings yet
- Nursing Care Plans For Burned PatientDocument5 pagesNursing Care Plans For Burned PatientJunah Marie Rubinos Palarca85% (26)
- NCP Cardiogenic ShockDocument3 pagesNCP Cardiogenic ShockTrixia Camporedondo100% (1)
- Nursing Care Plan Risk For InjuryDocument1 pageNursing Care Plan Risk For InjuryAce Dioso TubascoNo ratings yet
- Acute Pain OsteosarcomaDocument8 pagesAcute Pain OsteosarcomaMaryjoy Gabriellee De La Cruz100% (1)
- Nursing Care Plan For Hip Fracture Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationDocument1 pageNursing Care Plan For Hip Fracture Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationJaylord Verazon100% (1)
- NCP For RS-HF (Cor PulmonaleDocument5 pagesNCP For RS-HF (Cor PulmonaleMika Saldaña100% (1)
- Nursing Care Plan Rheumatoid ArthritisDocument3 pagesNursing Care Plan Rheumatoid ArthritisJashAnia MarIe EvArdo FloresNo ratings yet
- NCP (Deficient Fluid VolumeDocument3 pagesNCP (Deficient Fluid VolumeNica RespondoNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanSophia Loraine Dorone Jesura100% (1)
- Nursing Care PlanDocument2 pagesNursing Care PlanAldrein GonzalesNo ratings yet
- Post-Operative Nursing Care Plan # 1Document14 pagesPost-Operative Nursing Care Plan # 1Vince John SevillaNo ratings yet
- Actual NCP Pt.Document2 pagesActual NCP Pt.Kate WeyganNo ratings yet
- NCP FractureDocument7 pagesNCP FractureMacris BondocNo ratings yet
- "I Don't Have An Infection in My Gallbladder Which Is Good, But I Do Feel The Pain," As Verbalized by TheDocument2 pages"I Don't Have An Infection in My Gallbladder Which Is Good, But I Do Feel The Pain," As Verbalized by Theunnamed person100% (1)
- Escoton, Kate Angel P (NCP)Document4 pagesEscoton, Kate Angel P (NCP)Kate EscotonNo ratings yet
- Assessmen T Nursing Diagnosi S Nursing Goal Nursing Intervention Rationale Subjective Cues: Independent IndependentDocument3 pagesAssessmen T Nursing Diagnosi S Nursing Goal Nursing Intervention Rationale Subjective Cues: Independent IndependentKim Glaidyl BontuyanNo ratings yet
- NCP For ChronicPain PDFDocument2 pagesNCP For ChronicPain PDFjay kusainNo ratings yet
- NCP Pain 1Document6 pagesNCP Pain 1goodemonz15No ratings yet
- Parabola: Property of Cid - Deped Lipa City Under Learning From Home Scheme 2020Document20 pagesParabola: Property of Cid - Deped Lipa City Under Learning From Home Scheme 2020Charles Acielo100% (1)
- Book Review - The Offr Factory-1Document19 pagesBook Review - The Offr Factory-1Naveen Sharma100% (1)
- The Bowdoin Orient - Vol. 144, No. 23 - May 1, 2015Document24 pagesThe Bowdoin Orient - Vol. 144, No. 23 - May 1, 2015bowdoinorientNo ratings yet
- Sports Club ProfileDocument4 pagesSports Club Profilemanuel ramosNo ratings yet
- Effective Mobile Learning: 50+ Tips & Resources EbookDocument21 pagesEffective Mobile Learning: 50+ Tips & Resources EbookShelly Terrell100% (2)
- Final Ver Group 2 Assignment 3 MG632Document7 pagesFinal Ver Group 2 Assignment 3 MG632Arthur beatzNo ratings yet
- Writing Pt3Document7 pagesWriting Pt3Nur Amanina Binti Abd AzizNo ratings yet
- MORAL SELF-WPS OfficeDocument34 pagesMORAL SELF-WPS Officekicken chickenNo ratings yet
- Image Processing PDFDocument7 pagesImage Processing PDFRavindar Negi0% (1)
- Branches of Philosophy PDFDocument5 pagesBranches of Philosophy PDFBernard BasilioNo ratings yet
- Raman Research InstituteDocument2 pagesRaman Research InstituteGuru P MNo ratings yet
- MN006473A01 005 LACR Learning CatalogDocument68 pagesMN006473A01 005 LACR Learning CatalogAlvaro ApNo ratings yet
- Tantra Basics GlossaryDocument8 pagesTantra Basics Glossaryjeremiezulaski100% (1)
- Additional Resources Chapter One Study Pack 1Document3 pagesAdditional Resources Chapter One Study Pack 1hlumbane789No ratings yet
- Critical Literature ReviewDocument55 pagesCritical Literature Reviewcth_yao100% (1)
- Lesson-Plan-10 11 2021Document6 pagesLesson-Plan-10 11 2021AnnaMaria.2987No ratings yet
- Adverbs of Manner: Adjective Adverb Adjective AdverbDocument2 pagesAdverbs of Manner: Adjective Adverb Adjective AdverbDiana CoaylaNo ratings yet
- Practical ResearchDocument2 pagesPractical ResearchAAAAANo ratings yet
- Progress Test 4 PDFDocument1 pageProgress Test 4 PDFCsaba És Katalin KaracsonyiNo ratings yet
- GATE 2022 - Computer Science - Information TechnologyDocument2 pagesGATE 2022 - Computer Science - Information TechnologySumanNo ratings yet
- History and Nursing Knowledge: Guest Editor'S NoteDocument5 pagesHistory and Nursing Knowledge: Guest Editor'S NoteBernadeth Meily100% (1)
- Physicalscience q1 Mod13 Useoftheotheringredientsincleaningagents v2Document21 pagesPhysicalscience q1 Mod13 Useoftheotheringredientsincleaningagents v2Arthur LaurelNo ratings yet
- RiMINING TLS RIEGLDocument23 pagesRiMINING TLS RIEGLyadiomNo ratings yet
- 12 EsDocument4 pages12 Esrobinknit2009No ratings yet
- Lesson Plan Writing TSL 3112Document3 pagesLesson Plan Writing TSL 3112Judin MalekNo ratings yet
- JDVP SurveyDocument3 pagesJDVP SurveyAnnabel Marianas0% (1)
- Nawankot MonumentDocument6 pagesNawankot MonumentZishan AhmadNo ratings yet
- ESSENZA CatalogueDocument32 pagesESSENZA CataloguefisherNo ratings yet