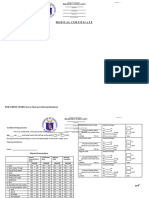
Medical Certificate: Department of Education
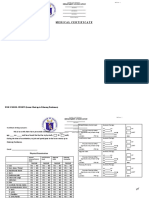
Medical Certificate: Department of Education
Download as doc, pdf, or txt
You might also like
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationJo EvangelistaNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateEeve Yhoung100% (2)
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationCamille Organis100% (2)
- Med Cert DepedDocument1 pageMed Cert DepedMark Cañete PunongbayanNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateJessie Montes JrNo ratings yet
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationnoreliNo ratings yet
- 2017 Medical CertificateDocument1 page2017 Medical CertificateBaliad JeanneNo ratings yet
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationMax DomonNo ratings yet
- Medical Certificate: For Palarong Pambansa OnlyDocument1 pageMedical Certificate: For Palarong Pambansa OnlyMarkusNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateCherry-Anne LetiNo ratings yet
- MedicalCertificate (Regular)Document1 pageMedicalCertificate (Regular)Gilbert Guzman TurarayNo ratings yet
- Regional Schools Press Conference Medical Certificate: Department of EducationDocument1 pageRegional Schools Press Conference Medical Certificate: Department of EducationKris Avein MalaayNo ratings yet
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationJeffreynald Arante FranciscoNo ratings yet
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationJosefina CagocoNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 PalaroJeoffrey Lance UsabalNo ratings yet
- Medical Certificate Form PalaroDocument1 pageMedical Certificate Form PalaroLeslie CastilloNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 PalaroJeoffrey Lance UsabalNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 PalaroJeoffrey Lance Usabal0% (1)
- 2017 Medical CertificateDocument1 page2017 Medical Certificateeking sarmientoNo ratings yet
- Palaro 2009 Medical CertificateDocument1 pagePalaro 2009 Medical CertificateHari Ng Sablay100% (1)
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationTyco MacNo ratings yet
- 2017 Medical CertificateDocument1 page2017 Medical Certificatejuanito buenaventuraNo ratings yet
- 2017 Parental ConsentDocument1 page2017 Parental ConsentAngelou GalonNo ratings yet
- Athlete Medical CertificateDocument1 pageAthlete Medical CertificateAmae GalagarNo ratings yet
- MedicalCertificate-form_-Sports-FINALDocument1 pageMedicalCertificate-form_-Sports-FINALkathleenNo ratings yet
- 2020 MedicalCertificate-ATHLETEDocument2 pages2020 MedicalCertificate-ATHLETEJoise Albertine J. Romblon100% (1)
- 4 - MedicalCertificateDocument1 page4 - MedicalCertificateamoremboneNo ratings yet
- Athlete Medical Certificate InvitationalDocument1 pageAthlete Medical Certificate InvitationalRo Fai DaNo ratings yet
- medical-for-officiating-officialsDocument1 pagemedical-for-officiating-officialsMa Alma RosalNo ratings yet
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 Palarogtunida100% (1)
- Medical Certificate 2010 PalaroDocument1 pageMedical Certificate 2010 PalaroAllen EndayaNo ratings yet
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of Educationshiela manalaysayNo ratings yet
- Medical Certificate 2010 Palaro 1Document1 pageMedical Certificate 2010 Palaro 1elijahgomez268No ratings yet
- Sample Medical CertificateDocument1 pageSample Medical CertificateAce Anthony Figueroa CaroNo ratings yet
- Medical Certificate 2010 Palaro 1Document1 pageMedical Certificate 2010 Palaro 1Anbu Clint Jarantilla MonsantoNo ratings yet
- Medical Certificate: To Whom It May ConcernDocument1 pageMedical Certificate: To Whom It May ConcernJheddai DuelasNo ratings yet
- Chaperon Commitment CertificateDocument1 pageChaperon Commitment CertificateGilbert Guzman TurarayNo ratings yet
- Parent Consent 2023Document2 pagesParent Consent 2023Reximie D. Dollete Jr.No ratings yet
- Medical For Athletes 1 Medical CertificateDocument2 pagesMedical For Athletes 1 Medical CertificateHanna BananaNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Rey Mark Gipulao100% (1)
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Annbelle Bognot BermudoNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Peachy FreezyNo ratings yet
- Rfot Medical CertificateDocument1 pageRfot Medical CertificateRyahNeil Bohol MoralesNo ratings yet
- Annex 3: General Intake SheetDocument2 pagesAnnex 3: General Intake SheetSouth SepakaNo ratings yet
- Cerificate of EnrollmentDocument1 pageCerificate of EnrollmentJulius MejiaNo ratings yet
- Medical For Coaches Asst Coaches Chaperones - v2024Document2 pagesMedical For Coaches Asst Coaches Chaperones - v2024Ellaisha AnselmoNo ratings yet
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationJone del PinoNo ratings yet
- Medical Certificate: Department of EducationDocument2 pagesMedical Certificate: Department of EducationSerLem WellNo ratings yet
- Medical Certificate 2016 PalaroDocument6 pagesMedical Certificate 2016 PalaroJosefina LlamadoNo ratings yet
- Medical For Athletes 1 1Document2 pagesMedical For Athletes 1 1Alvin TorbelesNo ratings yet
- Medical Certificate: To Whom It May ConcernDocument1 pageMedical Certificate: To Whom It May ConcernJaypee AgbayaniNo ratings yet
- Medical Certificate DSPC and DFOTDocument1 pageMedical Certificate DSPC and DFOTbenjie painaganNo ratings yet
- Sample Application Form of UPCMDocument5 pagesSample Application Form of UPCMHenrietta QuillaNo ratings yet
- Medical Certificate: Department of EducationDocument1 pageMedical Certificate: Department of EducationXavier Reyes HermanoNo ratings yet
- 2020 Commitment of ChaperonDocument1 page2020 Commitment of ChaperonEarvin Joseph Barace50% (2)
- 2017 Cerificate of EnrollmentDocument1 page2017 Cerificate of EnrollmentJimraida KalidNo ratings yet
- Medical Certificate For AthletesDocument2 pagesMedical Certificate For Athletesalshedjiboy22198No ratings yet
- Completion SeniorDocument1 pageCompletion SeniorJhean Laurence Orbon Siman - PaitNo ratings yet
- 2020 - Commiment of ChaperonDocument1 page2020 - Commiment of ChaperonRodel PajatinNo ratings yet
- Kagawaran NG Edukasyon - Sangay Na PalawanDocument12 pagesKagawaran NG Edukasyon - Sangay Na PalawanLance Aldrin AdionNo ratings yet
- Historical DataDocument1 pageHistorical DataLance Aldrin AdionNo ratings yet
- Kagawaran NG Edukasyon - Sangay Na PalawanDocument12 pagesKagawaran NG Edukasyon - Sangay Na PalawanLance Aldrin AdionNo ratings yet
- Filipino ChecklistDocument1 pageFilipino ChecklistLance Aldrin AdionNo ratings yet
- Republic of The Philippines: Organizational Chart School Disaster Risk Reduction and Management Team (SDRRMT)Document1 pageRepublic of The Philippines: Organizational Chart School Disaster Risk Reduction and Management Team (SDRRMT)Lance Aldrin AdionNo ratings yet
- Consolidated Project Kumustahan EspDocument3 pagesConsolidated Project Kumustahan EspLance Aldrin Adion71% (7)
- LDM1 Module 4 Readiness Checklist For Learners Teachers and ParentsDocument2 pagesLDM1 Module 4 Readiness Checklist For Learners Teachers and ParentsLance Aldrin AdionNo ratings yet
- DRRM CornerDocument13 pagesDRRM CornerLance Aldrin Adion100% (1)
- Heart and Neck VesselsDocument1 pageHeart and Neck VesselsLance Aldrin AdionNo ratings yet
- I. Introduction/Background: Land Area and Political SubdivisonDocument7 pagesI. Introduction/Background: Land Area and Political SubdivisonLance Aldrin AdionNo ratings yet
- Total: Sedurante, Michael Justin, ODocument18 pagesTotal: Sedurante, Michael Justin, OLance Aldrin AdionNo ratings yet
- Gad Plan & BudgetDocument25 pagesGad Plan & BudgetLance Aldrin Adion100% (2)
- Reading Profile 2020Document6 pagesReading Profile 2020Lance Aldrin Adion100% (1)
- Acknowledgement ReceiptDocument2 pagesAcknowledgement ReceiptLance Aldrin AdionNo ratings yet
- Gender EqualityDocument51 pagesGender EqualityLance Aldrin AdionNo ratings yet
- CSC Form 6 2017Document1 pageCSC Form 6 2017Lance Aldrin AdionNo ratings yet
- Extent of Implementation of Gender Equality Policy at Brady Philippines CorporationDocument7 pagesExtent of Implementation of Gender Equality Policy at Brady Philippines CorporationLance Aldrin AdionNo ratings yet
- Masterlist2018 ElemDocument18 pagesMasterlist2018 ElemLance Aldrin AdionNo ratings yet
- Human BehaviorDocument12 pagesHuman BehaviorLance Aldrin AdionNo ratings yet
- What Is Meant by GenderDocument4 pagesWhat Is Meant by GenderLance Aldrin AdionNo ratings yet
- Class Record: IV Learners' Names Written Works Performance TasksDocument27 pagesClass Record: IV Learners' Names Written Works Performance TasksLance Aldrin AdionNo ratings yet
- Class Record: IV Learners' Names Written Works Performance TasksDocument29 pagesClass Record: IV Learners' Names Written Works Performance TasksLance Aldrin AdionNo ratings yet