Nursing Leadership and Management PDF
Nursing Leadership and Management PDF
Uploaded by
hahahahaaaaaaaCopyright:
Available Formats
Nursing Leadership and Management PDF
Nursing Leadership and Management PDF
Uploaded by
hahahahaaaaaaaOriginal Title
Copyright
Available Formats
Share this document
Read this document in other languages
Did you find this document useful?
Is this content inappropriate?
Copyright:
Available Formats
Nursing Leadership and Management PDF
Nursing Leadership and Management PDF
Uploaded by
hahahahaaaaaaaCopyright:
Available Formats
Nursing Leadership and Management
Leadership Effectiveness
the use of one’s skill to influence others able to accomplish your objectives within the resource
parameters
Kinds of Influence: “doing the right things”
1. Assertiveness related to leadership
standing up for oneself and other’s without violating Efficiency
the rights of others able to accomplish you objectives/ production of results
Ex. You have chosen me as your leader... with minimum waste of time and effort
2. Rationality “doing the things right”
trying to convince someone by using reason, logic, or related to management
supporting information Management
Ex. We should do this because we need to give to the - Is the process of planning, organizing, directing and
patient total quality care controlling human and physical resources and technology
3. Ingratiation to achieve organizational goals / objectives?
making an individual feel important or good before
making a request 7 Basic resources of management
4. Exchange 1. Manpower
offering an exchange of favor 2. Money
5. Sanction 3. Machine
coercive authority o bigger equipment; capital expenses; to start a
give punishment for noncompliance or reward for business; costs more
compliance 4. Materials
6. Blocking o lesser/minor equipment; operation of
backing up a request with a threat to damage an organization or unit
individual’s opportunity for advancement 5. Methods – process
not really the best 6. Moment/Minutes – time management
7. Coalition 7. Market
getting co-workers to back-up a request
8. Upward appeal ADMINISTRATION MANAGEMENT
obtaining formal or informal support of a higher-up - Those at the top level of - Directly responsible to the
organization production of services
Levels of Leadership - Focus on establishing - Midline and lower levels of
- Personhood goals and on integrating hierarchy
o Respect work units to achieve the - Directs and guides the
o People follow because of what you are and organization’s mission operations of the
what you represent organization
- People Development Upper level manager:
o Reproduction - Primary responsible for establishing organizational goals
o People follow because of what you have done and strategic plans for the entire division of nursing
for them - Director of Nursing Services, Chairman, Executive Vice-
- Production President
o Results - 24/7 responsibility
o People follow because of what you have done Middle level manager:
for the organization - Usually coordinate nursing activities of several units
- Permission - Supervisor, coordinator, clinical nurse managers, case
o Relationships managers
o People follow because they want to - 24/7 responsibility
- Position First level manager:
o Rights - Directly responsible for the actual production of nursing
o People follow because they have to services; acts as links between higher level managers and
non-managers
Types of Leader - Head nurse (nurse manager), charge nurse (informal),
1. Formal team leader, primary nurse
officially appointed, elected Authority
managers - Legitimate right to give command, to make decisions
2. Informal - Ability to impose his or her with another person or group
chosen by the group Power
those who initiate an action - Ability to get results
- Given with authority
Management
getting things done Powers a manager/leader may possess
it is the process of getting activities completed efficiently - Legitimate power – based on position given
and effectively with and through people; production - Reward power - reward/incentives
is the process of planning, organizing, directing and - Coercive power- give sanctions or punishment
controlling human and physical resources - Expert power
- Referent power
o Charisma – innate personality trait
o Connection
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
- Self (Personal) power – based on individual’s maturity, LEADERSHIP STYLES
credibility, reputation, experience, gender 1. Autocratic
- Information power – based on the individual’s access to Makes decisions alone
valued data Task oriented
Power with coercion
Levels of Nurse Managers Proves useful (even necessary) in crisis situation
1. Upper Level Manager Authoritarian or exploitative style of leadership
primary responsible for establishing Satisfaction is low
organizational goals and strategic plans for the Effective when needed for immediate action
entire division of nursing High productivity, less satisfaction of workers
director of nursing service, chairman, executive 2 Types accdg. to Rensis Likert (Systems 4 approach):
vice president i. Exploitative-authoritative
nurse executives Have little trust in employees and exclude
Policy making body of an organization them in decision making
oversee the activities of the lower levels ii. Benevolent-authoritative
2. Middle Level Manager Are kind to employees but still do not
usually coordinates nursing activities of several involve them in decision making
units They ask the members
supervisor, coordinator, clinical nurse managers,
case managers 2. Democratic
oversee the activities of the lower levels Involve their followers in decision making
3. First Level Managers People oriented
directly responsible for the actual production of Leads to increase productivity and job satisfaction
nursing services There is compliance
acts as links between higher level managers and Participative/Consultative
non-managers 2 Types accdg. Rensis Likert (Systems 4 approach):
head nurse (nurse manager), charge nurse, team i. Consultative-democratic
leader, primary nurse Seek employees advice about decisions
ii. Participative-democratic
Authority Value employee involvement, teamwork
legitimate right to give commands, to make decisions and seek advice in decision making
Power
ability to get results 3. Laissez-faire
ability to impose his or her will on another person or group Loose and permissive
Ultraliberal
MANAGERS LEADERS Foster freedom for everyone and wants everyone to
Appointment Are appointed May or may not be happy
officially to positionhave official Results in low productivity and employee frustration
appointment to Most beneficial to a staff of highly motivated
position professionals
Power and Have power and As long as followers
Authority authority to enforce are willing 4. Bureaucratic
Goals Carry out Influnce others, Lacks a sense of security and depends on established
predetermined either formally or rules and policies
policies, rules and informally Tends to relate impersonality to staff
regulations Avoids decision making without standards or norms for
Risk-taking Maintain an orderly, Interested in risk- guidance
controlled, rational taking and Needed when discipline should be imposed
and equitable exploring new ideas
structure Types of Behaviour
Relationship According to their In an intuitive and 1. Passive or Non-assertive
with people own roles emphatic manner 2. Assertive – stand for oneself but doesn’t violate rights of
Self-reward When fulfilling From personal others
organizational achievements 3. Aggressive – violates rights of others
missions orgoals
THEORIES OF MANAGEMENT
Success as If they are May or may not be
1. Frederick Taylor
manager reappointed; successful manager
manager as long as “Theory of Scientific Management”
appointment holds Observed people in an electric plant
Time and motion studies
One best way to do the job
7 Basic Skills Required of a Leader/Manager
2. Max Weber
1. Conceptual skills
The ideal form of organization is “Bureaucracy”
2. Technical skills
With hierarchies—with rules and regulations
3. Human relations
3. Luther Gulick
4. Administrative skills
Introduced the 7 activities of management as
5. Communication skills
“POSDCORB” - planning, organizaing, staffing,
6. Analytical skills
directing, coordinating, reporting.
7. Decision making skills
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
4. Henry Fayol Rules of Delegation to Unlicensed Staff
Developed the principles management and o Do not delegate the functions of
functions of management assessment, teaching, evaluation and
nursing judgement
Fayol’s 14 Principles of Management: o Delegate activities that involve
i. Division of labor-you should know your job standard, unchanging procedures
ii. Authority, responsibility (pure obligation to o Delegate care of stable patients with
do the task to the best of your ability), and predictable outcomes; assessment as
accountability long as stable
iii. Unity of command Task that may not be delegated
iv. Unity of direction – one path, goal, objective o Assessment
v. Scalar chain of authority and o Interpretation of data
communication-highest to lowest level; o Care of invasive lines
channels of communication o Performing triads during emergencies
vi. Interest of the whole organization over o Making a nursing diagnosis
interest of the individual o IV insertion
vii. Equity and justice
viii. Order (hierarchy, everything in order, in their Span of Control
place) o Number of persons that the leader can
ix. Stability or tenure of personnel – rapid effectively manage
turnover would not benefit the organization o If noob-small span of control muna
x. Initiative-right to make their own projects, PODC
decisions
xi. Centralization- upper level of hierarchy 5. Mary Follet
makes decision Exercise power WITH people rather than power
xii. Discipline- follows rules over people
xiii. Remuneration - compensation Participatory management
xiv. Teamwork and esprit de corps 6. Elton May
“Hawthorne Effect”
Command responsibility Tendency of people to perform as expected
o Leader responsible for acts of because of special attention
subordinate Should show concern to subordinates to increase
o Respondeat superior level of performance
7. Kurt Lewin
Principle of Definition 3 phases of behaviour change
o Every employee must have a job o Unfreezing-identify what needs to be
description changed
o Changing – practicing, doing
Principle of delegation o Refreezing- integrating into your daily
o Entrusting responsibility to others and to activities
create accountability for results 8. Peter Drucker
Delegation Management by objectives (MBO)
o Provides learning opportunities for Be able to achieve your goals by having
subordinates objectives
o Increases power 9. Herbert Simon
o Cannot delegate total responsibility 2 approaches to decision making
o Do not delegate responsibility without o Optimizing-choosing the best possible
authorityg alternative; longer time to achieve
o Don’t just delegate boring jobs o Satisfying- first workable acceptable
For nurses, delegation is not an option but a solution
necessity 10. Henry Mintzberg
Proposed the managerial roles
5 Rights of Delegation Interpersonal roles
o Right Person o Figurehead role
o Right Task o Leader role
o Right Circumstance o Liaison role
o Right Direction/Communication Informational Roles
o Right Supervision o Monitor
o Dissemination
Causes of Underdelegating o Spokesman
o Waste of time to explain Decision Roles
o Believes that no one else can do the o Entrepreneur
job o Disturbance handler
o Fear- fear of criticism, fear of failing to o Negotiator
get others to follow him o Resource allocator role
o The need to control or be perfect
o Enjoys the personal satisfaction
o Gained from doing the work herself
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
MOTIVATIONAL THEORIES Fiedler’s Contingency theory
1. Maslow’s Hierarchy of Needs o Matches leadership style to situational
2. Douglas McGregor’s Theory X and Y factors
Theory X o Good relationship with subordinates
o Man is lazy, dislike work, unmotivated o Knowledge is needed to accomplish a
Theory Y task, use of relationship, power
o Man is self-motivated, enjoy their work Situational Theory by Hersey and Blanchard
3. William Ouchi (Theory Z) o Depends on the situation-may be
Involved workers are key to inc. productivity follower or leader
4. Ferdinand Herzberg o Considers the person’s readiness and
Hygienic factors- working environment willingness
Motivation factors-work itself 4. Path Goal Theory
o Give them work they really know People act as they do because they expect their
behaviour to produce satisfactory results
Hygenic factors Motivation factors Leader rewards followers for completing their task
(working environment) (work itself) 5. Contemporary Leadership Theory
- Adequate salary - Achievement Collaboration and teamwork
- Appropriate supervision - Recognition Transactional Leadership
- Good interpersonal - Appropriate Interaction between leaders and followers are
relations responsibility essentially economic- use rewards trade offs
- Safe and tolerable working - Opportunity for Transformational Leadership
condition advancement and Focusing on change through its commitment to
- Job security achievement its vision
- Agency policies and Empowering the subordinates
procedures Servant Leadership Theory (Greenleaf, 1977)
Leaders put serving others as number one priority
THEORIES OF LEADERSHIP Shared Leadership/Governance
1. Trait Theories – who the leader is Several individuals and subordinate share the
Great Man Theory (Aristotelian) responsibility in achieving the organization’s
o Leaders are born, not made goals
Charismatic Theory Quantum Leadership
Trait Studies Should be updated, innovative and creative
o integrity, intelligence, initiative, industry Initiate to update himself
o popularity, sociability, dependability Multiple Intelligence
2. Behavioral Theories – what leader can do Recognizes the different abilities affect
Lewin, Lippit and White leadership
o Leadership Styles Emotional Intelligence
Rensis Liker Understand feelings of others
o Systems 4 approach Cultural Bridges
Blake and Mouton Leaders/managers must become culturally
o Managerial Grid sensitive
o Country Club-high concern for people,
low on results FUNCTIONS/PROCESSES OF MANAGEMENT
o Impoverished-low concern for people
and results PLANNING
o Middle of the road - Deciding in advance what, where, how, when and who is
o Authority Compliance-high concern for to do future actions
results, low for people - Is a continuous process of assessing, establishing goals and
o Team- high concern for people and objectives, implementing and evaluating them which is
results subject to change as new facts are known
1,9 9,9 4 Planning modes:
Managemen Managemen 1. Reactive Planning – occurs after a problem exists;
t t done in response to a crisis
Country Club Team 2. Inactivism – a type of conventional planning
5,5 where the person considers the STATUS QUO as
Managemen stable environment
t 3. Preactivism – utilizes technology to accelerate
Middle of the change and is future-oriented; do not value
Road experience and the past; future is always
1,1 9,1 preferable
Managemen Managemen 4. Interactivism or Proactive – considers the past,
t t present and future; done in anticipation of
Impoverished Authority changing needs
compliance
3. Contingency-Situational Theories
Adapts leadership style depending on situation
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
Levels of Planning in Nursing: Budgeting Methods
1. Strategic Planning o Incremental
3-5 years years or more Flat percentage increase method
In charge of whole organization Consider the inflation rate (around
CEO, division heads, chief nurse 20%)
Exists farther in the future Multiply the current year expenses
by the inflation rate
2. Intermediate Planning
6 months-2 years o Zero-based
Supervisors, clinical specialist Requires managers to justify in
detail the cost of all programs both
3. Operational Planning and and new
1 week-1 year o Sunset Budget
Managers of nursing units, head nurse, charge Is designed to self-destruct within
nurse, primary care nurse, team leader the prescribed period to ensure
cessation of the funder program by
Scope of Planning a predetermined date
1. Forecast Are fixed expenses that cannot be
Estimate the future recovered even if a program is
Short or long range projections cancelled
Vision
o Mental image of something not actually *Participation by nursing personnel in planning and
visible, dreams, aspirations controlling budget leads to cost consciousness
Mission
o Purpose or brief statement identifying Time Management
reasons why organization exists o Making optimal use of available time
Philosophy o More work with less time
o Articulates a vision and provides statement o Work smarter not harder
beliefs and values that guide one’s practice 3 Steps in Time management
External and Internal Assessment o Establish priorities
o SWOT Analysis o Finish one task before beginning another
Know the strength to overcome the o Reprioritize
weaknesses; Know the External Time Wasters
opportunities to overcome the o Telephone interruptions
threats o Socializing
2. Set Goals/Objectives o Meetings
Goals-broad o Incomplete coworkers
o Achieve goals through OBJECTIVES o Paperworks and readings
Objectives- specific Internal Time Wasters
o SMART o Procrastination
o Behavioral o Poor planning
3. Develop and Schedule Strategies, Programs, Activities. Set time o Inability to say NO
frame. o Failure to set objectives
Strategy o Inability to delegate
o Overall plans of the higher management
system 5. Establish polices, control standards and evaluation procedures
Programs First step in evaluation
o Series of activities that function together to Standards
facilitate attainment of some desired goals o Indicate the minimal level of achievement
4. Prepare Budget accepted to meet the objectives
Allocation of resources or systematic plan of meeting o Pre-determined level of excellence that
expenses serves as a guide for practice
Purpose is TO SET operating cost limits Types of Standards
Approaches/Systems of Budgeting o Structure
o Centralized-upper level makes the budget Those that focus on the structure or
o Decentralized- middle and lower level management system used to
managers sets the budget then gives to deliver care including number and
upper level management categories of personnel
o Process
Types of Institutional Budget Refers to actual procedure, those
o Capital Budget activities engage in to administer
Lands, buildings, major equipments care
greater than 50,00 o Outcome
o Operating Budgets Result of the procedures and
Includes cost of supplies, minor nursing care
equipment repairs and overhead What results (if any) occurred as a
expenses result of specific intervention
o Manpower Budgets
Salaries and wages
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
Policies o Flat, decentralizaed
o Are guides of basic rules that define the Systematic delegation of power
general course and scope of activities and responsibility to middle and
Procedures lower levels of the organization
o Step by step guide to action o Matrix
Rules A second structure overlies the first
o Describe the situation that allow only one creating two directions for lines of
choice of action authority, accountability and
communication
ORGANIZING
Involves establishing a formal structure to provide for the FLAT PYRAMIDAL
coordination of resources to accomplish objectives Authority Decentralized Centralized
# of levels Fewer More
Scope of Organizing Span of Control Broad Narrow
1. Organizational Structure Delegation Greater Lesser
Refers to the way a group is formed including its: Control over Lesser More
CHANNELS OF AUTHORITY, SPAN OF CONTROL AND subordinates
LINES OF COMMUNICATION Type Modern Traditional
Is a mechanism through which work is arranged and
distributed among members of the organization to 2. Staffing
achieve goals and objectives
Assigning people to fill roles designed for the
Organizational Relationship organizational structure
o Formal or Reporting-straight line Process of determining and providing the accepting
o Informal or coordinating- broken line personnel to produce a desired level of care to meet
the patient’s demand
Organization Steps:
signifies an institution or a functional group with a formal o Recruitment
intentional structure of roles or positions o Selection/interview
o Hiring
Organizational Culture o Induction and orientation
consist of norms and traditions maintained Complete requirements you
deep rooted assumptions, beliefs and values that are
haven’t made
handed down from one generation to another
Organizing Patient Care
3 types of culture 5 Primary Means of Organizing Care For Patient
o Positive culture
Delivery :
Proactive and interactive to meet their
1. Total Patient Care or Case Method
satisfaction needs – based on
Oldest mode of organizing patient care
humanism, achievement, self- Nurses assume total responsibility for
actualization meeting the needs of all the patients
o Passive-agressive
assigned
Based on approval, dependent, and
avoidance norms 2. Functional
o Aggressive-defensive
Evolved as a result of WW2
Based on power, oppositional,
Task-oriented
competitive, and perfectionistic norms
3. Team
Organizational Climate Term by RN
is the own perception of characteristics of an organization
Ancillary personnel collaborate in
behaviour, attitudes and feelings of personnel providing care to a group of patients
Types of Organization by nature of Authority Requires extensive team
o Line organization communication and regular team
Each position has general authority
planning
over the lower position in the
hierarchy 4. Modular
Backbone of the organization
Like team nursing, but uses a smaller
o Staff/Matrix
team (buddy system)
Purely advisory, with no authority to Pairs professional nurse with ancillary
place recommendations to action nurse
o Functional
A specialist aid line positions within
5. Primary Care
a limited and clearly defined From admission to discharge
scope of authority As originally designed, requires an all-RN
staff
Forms/Patterns of Organizational Structure 24 hours responsibility for planning the
o Tall, pyramidal, or Centralized care of one or more patients
Systematic retention of power and During work hours, the primary nurse
responsibility at higher levels of
provides direct care to those patients
organization
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
Job Title
Managed care – an agency or corporation contracts Job relationship
with a group of providers to deliver specific services Performance description
for a limited cost per enrollee
Case Management DIRECTING
Refers to a service carried out by professionally Explaining what is to be done, to whom, at what time, how
trained individual who provides and or and why
coordinates health or social services Is the issuance of assignments, orders and instructions that
Coordinates care throughout an episode of permit the worker to understand what is expected of him
illness
Critical pathways-tools or guidelines that direct Scope of Directing
care by identifying expected outcomes
Even before and after discharge 1. Delegation
2. Supervision
Population-based health Care/ Disease Management Guiding and directing the work to be done, helping
Focus is on the covered lives or populations the individual do his work better
of patients with chronic illness rather than on Assess the capability of the individual if he needs
individual illness supervision
Differentiated Nursing Practice 3. Coordination
Delineates nursing roles based on their skills, Develop linkages/network
knowledge, educational level and Interdepartmental coordination
motivation o Medical team
o Radiology Dept.
Patient-focused Care Preparation for a procedure
Is a delivery model that brings all services Time schedules for special exams
and care at the bedside Proper notification of the nursing
service upon complication of
Patient Classification System procedures
o A method of grouping patients according to
the amount and complexity of their nursing o Lab Services
care o Administrative Services
o Self-Care- 1.5 hours; patients are capable of Chief Nurse
carrying out ADLs Recruitment
o Intermediate- 3 hours; requires some help Promotion
from the nursing staff with special Procurement of supplies and
treatments, or certain aspects of personal equipment
care; IVs, colostomy Budget preparation
o Total Care-4.5 hours; a bedridden patient
who lacks strength and mobility to do ADLs o Medical Records
o Intensive care- 4.5-6.5; a critically ill patient Safeguarding
who is in constant danger of death or serious Maintaining
injury Processing medical records
Scheduling o Dietary Service
o A timetable showing planned work days and Notification of new admission
shifts of a nursing personnel Patient transfers
Discharges
40 hour per week load (RA 5901) – less than 1,000,000 Specialty items for VIP admissions
but more than 5,000 they can be required for 48 hours and employees
o 8 hours X 5 days
o 10 hours X 4 days o Medical Social Services
o 12 hours X 3 days Patient’s record
Health education for patient,
Types of Scheduling: relatives and watchers
o Centralized – upper level schedule Referrals for patients in need of
o Decentralized-senior nurses schedule blood, medicine, financial and
o Cyclical/Block- 2 week period same material assistance
schedule. With off for a weekend
o Permanent Shifts- o Pharmacy
o Variable-floaters The pharmacy should provide the
nursing service with the established
More nurses in the morning. 45%, 37% and 18% hospital Drug Formulary including
effective and administration of
3. Job Descriptions medicines through the Unit drug
Are specifications of duties, conditions and Dose System (UDDS)
requirements of a particular job, also called
performance description
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
Principles: Categories of Conflict
o Responsbilities of each dept./ service should o Interpersonal
be clearly defined and understood by all Also known as horizontal violence
o Policies, guidelines, SOPs on or bullying
interdepartmental relationships should be o Intrapersonal
made available to all o Intergroup
o Schedules of different dept. should be Conflict Resolution Outcomes
synchronized and adhered to o Win-win
4. Communication o Win-lose
Process by which a message is sent, received and o Lose-lose
understood as intended
Ensuring common understanding Ways of Resolving Conflict
Flow of Communication o Avoiding
o Downward-highest to lowest Parties are aware of a conflict but
Memos choose not to acknowledge it or
Directives attempt to resolve it
o Upward-lowest to highest Lose-lose
Incident reports o Compromise
o Horizontal- peer groups Each party gives up something it
Endorsement wants
Types of Communication Lose-lose
o Formal o Competing
passes through the hierarchy One party pursue what it wants
o Informal regardless of the cost to others
no agenda needed Win-lose
o Verbal o Accommodating
Conferences One party sacrifices his beliefs and
Endorsement wants to allow the other party to
staff meetings win
change of shift reports Lose-win
o Written o Smoothing
patient’s chart An individual attempts to reduce
memos the emotional component of the
directives conflict
manuals of operation Win-lose
o Grapevine (Informal) o Majority Rule
effective nurse manager uses the Trying to resolve conflict by majority
grapevine advantageously by rule
maintaining an open and trusting Win-lose
relationship through the use of o Dominance and Suppression
formal communication channels One side is forced to give way to
and by giving pertinent information the other side
to liaison, influential or key people Loser is left feeling angry and
Tell one then it the one told will tell frustrated
another Win-lose
Risk for distortion of message; o Collaborating
correct immediately An assertive and cooperative
means of conflict resolution
Barriers to Effective Communication whereby all parties set aside their
o Physical Barriers- environmental factors original goals and work together a
Distance supraordinate or common priority
Noise goal.
Ventilation Win-win
o Social-psychologic- from judgements,
emotions and social values of people such Organizational Stresses
as lack of trust and respect o Task demands
Transference of patients Are associated with the specific
Emotionally unstable task
o Interpretation of meanings and semantics A nurse called during cardiac
Oral arrest
Written- POS o Role demands
Repeat order to doctor in Stress may result when there is role
telephone orders ambiguity
o Physical demands
5. Management of Conflict Back strains, feet problems, allergy
Conflict to some solution
o The internal or external struggle as a result of o Interpersonal demands
differences in ideas, values, or beliefs of two Associated with relationships within
or more people organizations
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
Benchmarking
6. Staff Development o Is a technique whereby an organization
In-service training programs seeks out the BEST PRACTICE in its
o Orientation industry to improve its performance
o Skills training
o Leadership training 2. Monitor and evaluate nursing care services utilizing various
o FREE methods
Continuing education programs Quality Assurance
o Seminars o Monitoring compliance with established
o Workshops standards
o Symposiums Total Quality Management
o Specialty nursing trainings o Also referred to as continuous quality
o Given by other accredited agencies improvement
PNA, Heart Centre o Doctor Edward Deming
o With payment from nurse o Focus is on doing the doing the right
things, the right way, the first time, all
7. Decision Making the time and problem prevention,
Decision-making tools planning, not inspective and reactive
o Gantt chart problem solving
tool used to visualize multiple tasks Nursing Audit
that need to be done o Method for assuring documentation of
o Decision tree quality of nursing care in keeping with
graphic tool to visualize established standards
alternatives available, chance o Types:
events and probable Open chart review or concurrent
consequences process- patient is still in the
o CPM (Critical Path Method) hospital; check charting;
calculate time estimate for observation of patient care
activities Closed chart review or
o PERT (Program Evaluation and Review retrospective process- patient is
Technique)- identifying key activities in a discharged
project, sequencing activities in a flow
diagram Performance Appraisal
Review previous activities before o Evaluated by supervisors
moving forward o Method of evaluating accomplishments
to help employees improve his work
CONTROLLING methods
Assessing/regulating performance o When done correctly, it is one of the
Process of seeing that actual expenditures and activities greatest tools an organization has to
conform to plan develop and motivate staff
Quality Control o When done poorly, it has the potential
o Activities that evaluate, monitor, or regulate to discourage and demotivate
services rendered to consumers
Types of evaluation responses
Total Quality Management o Free Response Report
Management Comment in writing on the
Quality Improvement quality of the nurse’s
Improvement performance
Quality Assurance o Performance Checklist
Prevention Indicate in a checklist the
Quality Control behaviour desired in the
Inspection performance
o Simple Ranking
Scope of Controlling Employee is ranked in relation
to his co-workers
1. Establish standards for measuring performance o Graphic Rating
No one set of standards fits all organization Use graph or a numerical
Standards must be SMART scale
Criteria/Indicators of Standards o Forced-choice Comparison
o Characteristics used to measure Choose from a group of
performance weighted descriptive
Audits Frequently used in Quality Control statements those that best
o Structure Audit describe the nurse
o Process Audit
o Outcome Audit Common Errors of Evaluation
o Halo error
Good things done
overshadow errors
University of Santo Tomas – College of Nursing / JSV
Nursing Leadership and Management
o Horn’s
Poor performance Four Common Steps in Progressive Discipline
overshadowed good 1. Informal reprimand or verbal
performance admonishment
underrated 2. Formal reprimand or written
o Logical error admonishment
First impression 3. Suspension from work without
o Central tendency error pay
All treated as average 4. Termination
o Leniency error
Given mercy rating 4. Meeting change confidently
Planned Change
Quality Program Evaluation o Overt-one that people are aware of
o FOCUS-PDCA model o Covert- hidden or occurs without the
o Provides a systematic method to study individual’s awareness.
a work process for improvement. It May be gradual or sudden
includes:
Find a process to improve Unplanned Change
Organize a team that knows o Is an alteration imposed by external
the process events or persons and occurs when
Clarify current knowledge of unexpected event, force or reaction
the process All major change brings feelings of achievement,
Understanding causes of loss and stress
process variation
Select the process Change Agent Strategies
improvement o Empirical-rational
Plan the improvement People are willing to adapt or
Do data collection, data change if it is justified and if
analysis and improvement they are shown how they can
Check data process benefit from the change
improvement and costumer o Normative-reeducative
outcome Are based on the assumption
Act to maintain and continue that people act according to
improvement their commitment to socio-
cultural norms
3. Employee discipline Staff development through
Is the process of generating employee training groups
compliance with the institutional rules and o Power-coercive
regulations When you comply to the
Problem employees: rule breakers, marginal plans, direction of the more
employees (working but do not exert effort to powerful
improve), and chemically or mentally impaired Strikes, sit-ins, negotiations
Principles of disciplinary action
o Have a positive attitude 5. Legal and ethical control
If they are treated as suspects
they are more likely to provide
the trouble that the manager
anticipates
o Investigate carefully
o Be prompt
o Protect privacy
o Focus on the act
o Enforce rules carefully. Use extreme
caution in instituting disciplinary
measures
o Be flexible
o Take corrective, constructive actions
o Should be progressive in nature
preceded with counselling
Counselling
Verbal reprimand
Written reprimand
Short suspension
Long suspension
Dismissal/Discharge
University of Santo Tomas – College of Nursing / JSV
You might also like
- Nursing Leadership and Management For Patient Safety and Quality Care PDFDocument409 pagesNursing Leadership and Management For Patient Safety and Quality Care PDFAnonymous FGqnrDuM94% (16)
- LMR Answer KeyDocument18 pagesLMR Answer KeyDon Marcus88% (8)
- Directing in Nursing ManagementDocument27 pagesDirecting in Nursing Managementwersken100% (5)
- Organizational Development and Change ExamNotesDocument36 pagesOrganizational Development and Change ExamNotesAbbas T P90% (10)
- Nursing Management & LeadershipDocument8 pagesNursing Management & LeadershipDjhoanna Kriska88% (42)
- Nursing Leadership & ManagementDocument36 pagesNursing Leadership & ManagementPrince Paraiso100% (7)
- Nursing Leadership and Management ExamsDocument4 pagesNursing Leadership and Management ExamsMarisol Jane Jomaya67% (9)
- Leadership and Managementfinal Nursing ReviewerDocument23 pagesLeadership and Managementfinal Nursing ReviewerPhilip Simangan100% (6)
- Nursing Management Process and FunctionsDocument151 pagesNursing Management Process and FunctionsJaq Kyatchon90% (30)
- Test Bank Leadership and Management in Nursing 4th EditionDocument5 pagesTest Bank Leadership and Management in Nursing 4th EditionRichard1Lauritsen86% (7)
- NCM 119 Midterm ExamDocument23 pagesNCM 119 Midterm Examlainey10190% (10)
- Intensive Palmr 1 Nothing CompressDocument4 pagesIntensive Palmr 1 Nothing CompressjsNo ratings yet
- Palmer Nursing ReviewerDocument9 pagesPalmer Nursing ReviewerVon R Semilla50% (2)
- NCM 119 Notes EndtermDocument11 pagesNCM 119 Notes EndtermDJ Evan Jules100% (1)
- Nursing Leadership and Management Prelims Lesson 1-5Document4 pagesNursing Leadership and Management Prelims Lesson 1-5Paul Christian P. Santos, RN100% (14)
- Nursing Leadership and ManagementDocument305 pagesNursing Leadership and Managementpaul andrew laranjo asuncion97% (30)
- CBQ - Leadership and Management in Nursing 2009Document14 pagesCBQ - Leadership and Management in Nursing 2009Lizette Leah Ching95% (20)
- Nursing Leadership and ManagementDocument43 pagesNursing Leadership and Managementbajaoc95% (22)
- Midterm Leadership and Management (MCN 107) EXAMDocument26 pagesMidterm Leadership and Management (MCN 107) EXAMsophi30100% (1)
- Palmr FCDocument21 pagesPalmr FCMei Joy100% (1)
- Controlling in Nursing ManagementDocument45 pagesControlling in Nursing Managementverna92% (38)
- Leadership and Management in NursingDocument5 pagesLeadership and Management in NursingSolsona Natl HS Maananteng50% (2)
- LEC 1 PRELIM Nursing Leadership and ManagementDocument307 pagesLEC 1 PRELIM Nursing Leadership and ManagementMae Montesena BreganzaNo ratings yet
- Unit 1 Chapter 2 Nursing Leadership and ManagementDocument9 pagesUnit 1 Chapter 2 Nursing Leadership and Managementfree_books_jym100% (2)
- Concept 1 - Leadership & Management in NursingDocument652 pagesConcept 1 - Leadership & Management in Nursingezenz0205100% (3)
- Nursing Leadership and Management Practice TestDocument6 pagesNursing Leadership and Management Practice TestHaifi Hun0% (1)
- Zamboanga Del Sur General Hospital: Staff Nurse Performance Evaluation SheetDocument5 pagesZamboanga Del Sur General Hospital: Staff Nurse Performance Evaluation Sheethahahahaaaaaaa100% (1)
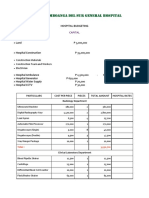
- Hospital Budgeting: - Construction Materials - Construction Team and Workers - ElectricianDocument11 pagesHospital Budgeting: - Construction Materials - Construction Team and Workers - ElectricianhahahahaaaaaaaNo ratings yet
- CHN Lecture SY2015-2016 1 SemesterDocument141 pagesCHN Lecture SY2015-2016 1 SemesterhahahahaaaaaaaNo ratings yet
- Reading Skills. Ibt TOEFL 2Document11 pagesReading Skills. Ibt TOEFL 2litamelperuNo ratings yet
- Rational Choice TheoryDocument5 pagesRational Choice Theorycharlene saguinhonNo ratings yet
- Probability and Statistics For EngineersDocument42 pagesProbability and Statistics For EngineersJennifer ThomasNo ratings yet
- Jay Walljasper, Project For Public Spaces - The Great Neighborhood Book - A Do-it-Yourself Guide To Placemaking (2007)Document193 pagesJay Walljasper, Project For Public Spaces - The Great Neighborhood Book - A Do-it-Yourself Guide To Placemaking (2007)Sandra SamirNo ratings yet
- Business and Administrative Communication by Kitty Locker and Donna Kienzler - 10e, TEST BANK 0073403180Document35 pagesBusiness and Administrative Communication by Kitty Locker and Donna Kienzler - 10e, TEST BANK 0073403180jksmtnNo ratings yet
- Guay Motivation ScaleDocument5 pagesGuay Motivation Scaleadanon9375% (4)
- Task-Oriented Relationship-Oriented Participative Leadership Task-OrientedDocument17 pagesTask-Oriented Relationship-Oriented Participative Leadership Task-OrientedDENNIS N. MUÑOZNo ratings yet
- Nursing Leadership and ManagementDocument8 pagesNursing Leadership and Managementaurezea50% (2)
- NLM QuestionsDocument15 pagesNLM Questionsleoboi_leoboi81% (16)
- Nursing Professional Adjustment, Leadership and ManagementDocument8 pagesNursing Professional Adjustment, Leadership and ManagementRolther Villaflor CapioNo ratings yet
- NSG 129: Nursing Leadership and ManagementDocument13 pagesNSG 129: Nursing Leadership and ManagementJOHN PEARL FERNANDEZ100% (1)
- Nursing Leadership and ManagementDocument13 pagesNursing Leadership and ManagementChrisgr8100% (6)
- Nursing Leadership - Reviewquestion 1Document6 pagesNursing Leadership - Reviewquestion 1Darren Jay Nikazy80% (5)
- Nursing Management and LeadershipDocument143 pagesNursing Management and LeadershipVivi rikkaNo ratings yet
- Professional AdjustmentDocument16 pagesProfessional Adjustmentnoelitoluzon100% (5)
- Nursing LeadershipDocument14 pagesNursing LeadershipJohn Paul Casiraya AgacerNo ratings yet
- NCM 119 PrelimDocument12 pagesNCM 119 Prelimczeremar chan100% (1)
- Nursing Leadership and ManagementDocument7 pagesNursing Leadership and ManagementCecilio AlvarezNo ratings yet
- Nursing Leadership and ManagementDocument182 pagesNursing Leadership and ManagementAlain Dave90% (10)
- Nursing Leadership and ManagementDocument20 pagesNursing Leadership and ManagementDenzelle Zchallet100% (1)
- QUESTIONS For NRSG MNGT and LeadershipDocument13 pagesQUESTIONS For NRSG MNGT and Leadershipd1choosen100% (1)
- NCM 119 CompilationDocument57 pagesNCM 119 Compilationticker100% (1)
- Nursing Management 2Document118 pagesNursing Management 2Jasmin Jacob100% (36)
- Nursing Research, Leadership and MGMT (1) .Document14 pagesNursing Research, Leadership and MGMT (1) .shariternolaNo ratings yet
- Sample Exam 40 Items LMRDocument8 pagesSample Exam 40 Items LMRChiskie Faldas GenodiaNo ratings yet
- Leadership & Management 2013 HandoutsDocument138 pagesLeadership & Management 2013 HandoutsHampson Malekano88% (8)
- Palmer Nursing ReviewerDocument9 pagesPalmer Nursing ReviewerVon R SemillaNo ratings yet
- Palmer Nursing ReviewerDocument11 pagesPalmer Nursing ReviewerRielle MatasNo ratings yet
- Human Behavior NotesDocument9 pagesHuman Behavior NotesDiola QuilingNo ratings yet
- Chapter 3 - HboDocument4 pagesChapter 3 - HboJosephine LeonNo ratings yet
- Cepm T1 T2Document13 pagesCepm T1 T2Gwyneth Lynn C. InchanNo ratings yet
- Leadership MNGT .PPT Online PresentationDocument58 pagesLeadership MNGT .PPT Online PresentationDivynne Bless Madelo100% (2)
- PALMRDocument10 pagesPALMRggukNo ratings yet
- Basic Concept of Leadership and ManagementDocument5 pagesBasic Concept of Leadership and ManagementLenie DegraciaNo ratings yet
- Organization & ManagementDocument3 pagesOrganization & ManagementLara MarceloNo ratings yet
- Humanbe Midterm ReviewerDocument11 pagesHumanbe Midterm ReviewerLove Glenhir MestidioNo ratings yet
- OrgMa Reviewer 1 1Document10 pagesOrgMa Reviewer 1 1potato langNo ratings yet
- Intensive Palmr 1 NothingDocument5 pagesIntensive Palmr 1 Nothingxktct94q4mNo ratings yet
- LM HandoutDocument9 pagesLM HandoutKyrajane EsguerraNo ratings yet
- Freaom 2Document9 pagesFreaom 25sdggfnpq4No ratings yet
- Napili Ka Because of A QualityDocument4 pagesNapili Ka Because of A QualityNicholas TagleNo ratings yet
- CefuroximeDocument1 pageCefuroximehahahahaaaaaaaNo ratings yet
- Balance, Posture and Body AlignmentDocument6 pagesBalance, Posture and Body AlignmenthahahahaaaaaaaNo ratings yet
- PantoprazoleDocument1 pagePantoprazolehahahahaaaaaaaNo ratings yet
- Biodata and AnaphyDocument3 pagesBiodata and AnaphyhahahahaaaaaaaNo ratings yet
- Fluids and Electrolytes: 2. Interstitial SpaceDocument13 pagesFluids and Electrolytes: 2. Interstitial Spacehahahahaaaaaaa100% (1)
- Drug TableDocument1 pageDrug TablehahahahaaaaaaaNo ratings yet
- FilariasisDocument11 pagesFilariasishahahahaaaaaaa100% (1)
- Composition Qualifications and Terms of HRDocument2 pagesComposition Qualifications and Terms of HRhahahahaaaaaaaNo ratings yet
- Escavape Cloud RoomDocument2 pagesEscavape Cloud RoomhahahahaaaaaaaNo ratings yet
- Service Ward FebruaryDocument1 pageService Ward FebruaryhahahahaaaaaaaNo ratings yet
- The Wall of The Heart Consists of Three Layers of TissueDocument4 pagesThe Wall of The Heart Consists of Three Layers of TissuehahahahaaaaaaaNo ratings yet
- Journal Headnusring 4CDocument1 pageJournal Headnusring 4ChahahahaaaaaaaNo ratings yet
- 3C Drug StudyDocument2 pages3C Drug StudyhahahahaaaaaaaNo ratings yet
- Radiologic Technologist Job DescriptionDocument1 pageRadiologic Technologist Job DescriptionhahahahaaaaaaaNo ratings yet
- Ap Psychology Unit 5 OverviewDocument4 pagesAp Psychology Unit 5 Overviewapi-262090199No ratings yet
- Advait VendataDocument10 pagesAdvait VendataReandil CarreosNo ratings yet
- Short Story Guided Notes MDocument5 pagesShort Story Guided Notes Mapi-204719782No ratings yet
- Analysis of Matthew Arnolds Dover BeachDocument2 pagesAnalysis of Matthew Arnolds Dover BeachP DasNo ratings yet
- The Ethical MindDocument2 pagesThe Ethical MindGautamNo ratings yet
- Home Visit Plan2Document2 pagesHome Visit Plan2Bianca BasnilloNo ratings yet
- AI Essay Final PrintDocument5 pagesAI Essay Final PrintShao Shyang Chuang100% (1)
- Introduction To Human Resource ManagementDocument26 pagesIntroduction To Human Resource ManagementPrateek BhargavaNo ratings yet
- Influence of Active Reminders On Oral Hygiene Compliance in Orthodontic PatientsDocument6 pagesInfluence of Active Reminders On Oral Hygiene Compliance in Orthodontic PatientsPutu WidiastriNo ratings yet
- BSCA Luzon Wide Research IIDocument20 pagesBSCA Luzon Wide Research IIEduard CastilloNo ratings yet
- Human Resource Management, A Contemporary PerspectiveDocument43 pagesHuman Resource Management, A Contemporary Perspectivechandmagsi90% (10)
- Rauhauser's Conspiracy Theory Involving Conspiracy TheoristsDocument3 pagesRauhauser's Conspiracy Theory Involving Conspiracy TheoristsAaronWorthingNo ratings yet
- Chapter1 Introduction To Management ProcessDocument4 pagesChapter1 Introduction To Management Processsuhaib1282No ratings yet
- A-Glance-at-Contemporary-Social-Theories 3 PDFDocument4 pagesA-Glance-at-Contemporary-Social-Theories 3 PDFROX RICABLANCANo ratings yet
- Socio-Emotional Processes of DevelopmentDocument17 pagesSocio-Emotional Processes of DevelopmentNathalie DagmangNo ratings yet
- DV Graal - The Dragon's HeartDocument5 pagesDV Graal - The Dragon's HeartVarious TingsNo ratings yet
- The Sociology of Humor PDFDocument38 pagesThe Sociology of Humor PDFCloudiu9100% (1)
- Cognitive TheoryDocument19 pagesCognitive TheoryAriel De La CruzNo ratings yet
- Case Study by BalramDocument11 pagesCase Study by BalramShashank100% (1)
- Influences On Individual Communication & Interpersonal ProcessesDocument32 pagesInfluences On Individual Communication & Interpersonal ProcessesLindsey Marie0% (1)
- Final Power Point Erik EriksonDocument12 pagesFinal Power Point Erik EriksonJake CasipleNo ratings yet
- Inner Beauty Doesn't Really ExistDocument1 pageInner Beauty Doesn't Really ExistMistermickeyNo ratings yet
- SKMU 3812 - Group Project GuidelinesDocument2 pagesSKMU 3812 - Group Project GuidelinesUmmu AfiqahNo ratings yet