Quantitative Evaluation of Lip Symmetry in Functional Asymmetry
Quantitative Evaluation of Lip Symmetry in Functional Asymmetry
Download as pdf or txt
You might also like
- Functional Occlusion After Fixed Appliance Orthodontic Treatment: A UK Three-Centre StudyDocument8 pagesFunctional Occlusion After Fixed Appliance Orthodontic Treatment: A UK Three-Centre StudyRebin AliNo ratings yet
- Robert M. Mason, DMD, PHD: Clinical Assessment of The Freeway SpaceDocument2 pagesRobert M. Mason, DMD, PHD: Clinical Assessment of The Freeway SpaceplsssssNo ratings yet
- Relationship Between Molar Occlusion and Masticatory Movement in Lateral Deviation of The MandibleDocument9 pagesRelationship Between Molar Occlusion and Masticatory Movement in Lateral Deviation of The MandibleLina Pérez SánchezNo ratings yet
- CirugiaDocument27 pagesCirugiaalexmtzgNo ratings yet
- Functional OcclusionDocument8 pagesFunctional OcclusionNoor SolikhahNo ratings yet
- 1-S2.0-S0278239119305518-MainDocument15 pages1-S2.0-S0278239119305518-MainALEJANDRA INÉS NIETO ARIASNo ratings yet
- Asymmetries EtiologyDocument15 pagesAsymmetries EtiologyJhovanny OrozcoNo ratings yet
- 2014 AJODO SilveiraDocument11 pages2014 AJODO SilveiraJavier Farias VeraNo ratings yet
- Asymmetry of The Face in Orthodontic PatientsDocument6 pagesAsymmetry of The Face in Orthodontic PatientsplsssssNo ratings yet
- 191 FullDocument9 pages191 Fulljavi222222No ratings yet
- Maryam Alsadat Hashemipour 1 Most Impacted 3 M MBDocument6 pagesMaryam Alsadat Hashemipour 1 Most Impacted 3 M MBAlexandra CicaNo ratings yet
- Jced 5 E231Document8 pagesJced 5 E231ruben dario meza bertelNo ratings yet
- Mal OcclusionDocument8 pagesMal OcclusionLuke XuNo ratings yet
- 1 s2.0 S0889540618300611 MainDocument9 pages1 s2.0 S0889540618300611 MainAly OsmanNo ratings yet
- Short-Term and Long-Term Treatment Outcomes With The FR-3 Appliance of FränkelDocument12 pagesShort-Term and Long-Term Treatment Outcomes With The FR-3 Appliance of FränkelricardoNo ratings yet
- DiPietro 1976 Significance of FMA To ProsDocument12 pagesDiPietro 1976 Significance of FMA To ProsomidNo ratings yet
- Editor in Chief,+ej Clinicmed+24Document8 pagesEditor in Chief,+ej Clinicmed+24Muhmmad Zaman SheraniNo ratings yet
- FDSFCFDSFDocument10 pagesFDSFCFDSFBhumika ChawlaNo ratings yet
- Autoligado 4Document6 pagesAutoligado 4marcela0426No ratings yet
- NIH Public AccessDocument22 pagesNIH Public AccessMariana SantosNo ratings yet
- Face MaskDocument7 pagesFace MaskWaraphon JanewakornwongNo ratings yet
- Glenoid Fossa Position in Class II Malocclusion Associated With Mandibular RetrusionDocument5 pagesGlenoid Fossa Position in Class II Malocclusion Associated With Mandibular RetrusioncaroNo ratings yet
- Association Between 3-Dimensional Mandibular Morphology and Condylar Movement in Subjects With Mandibular Asymmetry 1Document11 pagesAssociation Between 3-Dimensional Mandibular Morphology and Condylar Movement in Subjects With Mandibular Asymmetry 1Valentina Ríos BorrásNo ratings yet
- Hard - and Soft-Tissue Symmetry Comparison in Patients With Class III MalocclusionDocument14 pagesHard - and Soft-Tissue Symmetry Comparison in Patients With Class III MalocclusionSoe San KyawNo ratings yet
- Role of Cephalometery in Evaluation of Vertical DimensionDocument4 pagesRole of Cephalometery in Evaluation of Vertical DimensionAhmad ShoeibNo ratings yet
- Medoralv17 I3 Pe435Document7 pagesMedoralv17 I3 Pe435ortodoncia 2022No ratings yet
- Comparison of The Effects of Twin Block and Activator Treatment On The Soft Tissue ProfileDocument7 pagesComparison of The Effects of Twin Block and Activator Treatment On The Soft Tissue ProfilemishaladnankpNo ratings yet
- TMJ MorphologyDocument6 pagesTMJ MorphologyHossam BarghashNo ratings yet
- Tweed's Philosophy-A Review: June 2018Document10 pagesTweed's Philosophy-A Review: June 2018rohitNo ratings yet
- Correction of Class III Malocclusions Through Morphological Changes of The Maxilla Using The Protraction Face Mask by Three Different Therapeutic ApproachesDocument11 pagesCorrection of Class III Malocclusions Through Morphological Changes of The Maxilla Using The Protraction Face Mask by Three Different Therapeutic ApproachesMariana SantosNo ratings yet
- Evaluation of Different Treatments For Oroantral Oronasal Communications - Abuabara Et Al PDFDocument4 pagesEvaluation of Different Treatments For Oroantral Oronasal Communications - Abuabara Et Al PDFVictor HernandezNo ratings yet
- Dimension TransversalDocument10 pagesDimension TransversalEstaf EmkeyzNo ratings yet
- Evaluation of Soft-Tissue Changes in Young Adults Treated With The Forsus Fatigue-Resistant DeviceDocument11 pagesEvaluation of Soft-Tissue Changes in Young Adults Treated With The Forsus Fatigue-Resistant DeviceDominikaSkórkaNo ratings yet
- Nivelacion Curva de SpeeDocument9 pagesNivelacion Curva de SpeenicovejarNo ratings yet
- Correlation Between Cranial Base Morphology and The Position of The Glenoid Fossa in Patients With Facial AsymmetryDocument5 pagesCorrelation Between Cranial Base Morphology and The Position of The Glenoid Fossa in Patients With Facial AsymmetryValentina Ríos BorrásNo ratings yet
- Original Research Article: Burhan Showkat, Jayesh S. Rahalkar, Sandeep Jethe, Ravindra ManerikarDocument5 pagesOriginal Research Article: Burhan Showkat, Jayesh S. Rahalkar, Sandeep Jethe, Ravindra ManerikarjaslinshalinNo ratings yet
- 1 s2.0 S0889540621005631 MainDocument8 pages1 s2.0 S0889540621005631 MainDANTE DELEGUERYNo ratings yet
- Nasolabial Symmetry Following Tennison-Randall Lip RepairDocument10 pagesNasolabial Symmetry Following Tennison-Randall Lip RepairShaly MaduroNo ratings yet
- Xác Định Nguyên Nhân Cắn Hở- Cắn SâuDocument8 pagesXác Định Nguyên Nhân Cắn Hở- Cắn Sâutâm nguyễnNo ratings yet
- Comparison Between Skeletal, and Facial Measurements of Vertical Dimension in Edentulous PatientsDocument4 pagesComparison Between Skeletal, and Facial Measurements of Vertical Dimension in Edentulous Patientspaula catanaNo ratings yet
- Evaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyDocument10 pagesEvaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyPututu PatataNo ratings yet
- Craniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingDocument10 pagesCraniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingMonojit DuttaNo ratings yet
- Seehra2012 AJODO Retrospectivo MáscaraDocument6 pagesSeehra2012 AJODO Retrospectivo MáscaraYeimi ArdilaNo ratings yet
- ALTRAMECARTICULODocument12 pagesALTRAMECARTICULOAlejandra NietoNo ratings yet
- GnatologieDocument8 pagesGnatologieAlexandra FocaNo ratings yet
- Glenoid Fossa RemodellingDocument59 pagesGlenoid Fossa RemodellingArnabNo ratings yet
- J Ajoms 2014 09 006Document7 pagesJ Ajoms 2014 09 006mudepaNo ratings yet
- A Comparison Between Arbitrary and KinematicDocument4 pagesA Comparison Between Arbitrary and KinematicsmritinarayanNo ratings yet
- Intjmi v8n2p84 FaDocument7 pagesIntjmi v8n2p84 FaRein KarnasiNo ratings yet
- Articulo de InglesDocument7 pagesArticulo de InglesJose Manuel Caldelas GuizarNo ratings yet
- 052008-276 1 PDFDocument6 pages052008-276 1 PDFCynthia AlfaroNo ratings yet
- Linear Mandibular Measurements ComparisoDocument7 pagesLinear Mandibular Measurements ComparisoDeyan SyambasNo ratings yet
- Perinetti.2010 - Dental Malocclusion and Body Posture in Young Subjects - A Multiple Regression StudyDocument8 pagesPerinetti.2010 - Dental Malocclusion and Body Posture in Young Subjects - A Multiple Regression Studysalvatoreaurelio.cannataNo ratings yet
- 10 1093@ejo@cjv053Document11 pages10 1093@ejo@cjv053Drazza TagaldinNo ratings yet
- Comparision of Orofacial Airway Dimensions in Subject With Different Breathing PatternDocument8 pagesComparision of Orofacial Airway Dimensions in Subject With Different Breathing PatternLudy Jiménez ValdiviaNo ratings yet
- The Effect of Posterior Bite Plane On Dentoskeletal Changes in Skeletal Open Bite Malocclusion (2018)Document3 pagesThe Effect of Posterior Bite Plane On Dentoskeletal Changes in Skeletal Open Bite Malocclusion (2018)Novita BerlianaNo ratings yet
- Changes in Facial Form Relative To Progressive Atrophy of The Edentulous JawsDocument7 pagesChanges in Facial Form Relative To Progressive Atrophy of The Edentulous JawsshraddhaNo ratings yet
- Reverse-Sequencing Chewing Patterns Evaluation in Anterior Versus Posterior Unilateral Crossbite Patients.Document7 pagesReverse-Sequencing Chewing Patterns Evaluation in Anterior Versus Posterior Unilateral Crossbite Patients.Ale RamírezNo ratings yet
- Facial AsymmetryDocument41 pagesFacial AsymmetryRahul GoteNo ratings yet
- Fellowship Centers 2024 2025Document4 pagesFellowship Centers 2024 2025Neel GuptaNo ratings yet
- Face WizardDocument22 pagesFace Wizardscribdthrowaway3No ratings yet
- Structure and Functions of The EyeDocument16 pagesStructure and Functions of The EyeabdirizakNo ratings yet
- Share Face Recognition TechnologyDocument15 pagesShare Face Recognition TechnologyBikram RockNo ratings yet
- Review Article 2Document5 pagesReview Article 2Kartik R. MorjariaNo ratings yet
- Prosthetic Aspects of Dental Implants - IIDocument73 pagesProsthetic Aspects of Dental Implants - IIKomal Talreja100% (1)
- IGCSE 0610 - EYES Sense Organs NOTES (2023-2025)Document4 pagesIGCSE 0610 - EYES Sense Organs NOTES (2023-2025)ckqx1234No ratings yet
- MalocclusionDocument29 pagesMalocclusionsidney changiNo ratings yet
- Aesthetic Management of Immediate Anterior Tooth Replacement With Ovate Pontic: A Case Report PDFDocument5 pagesAesthetic Management of Immediate Anterior Tooth Replacement With Ovate Pontic: A Case Report PDFAnita PrastiwiNo ratings yet
- Periodontal Prosthesis in Contemporary Dentistry: SciencedirectDocument8 pagesPeriodontal Prosthesis in Contemporary Dentistry: SciencedirectJuan Carlos Montañez BenavidesNo ratings yet
- Anatomy and Function of The Eye: Henry J. KaplanDocument7 pagesAnatomy and Function of The Eye: Henry J. KaplanCucută Alexandru-DanielNo ratings yet
- Departemen Ilmu Kesehatan Mata Fakultas Kedokteran Universitas Padjadjaran Pusat Mata Nasional Rumah Sakit Mata Cicendo BandungDocument11 pagesDepartemen Ilmu Kesehatan Mata Fakultas Kedokteran Universitas Padjadjaran Pusat Mata Nasional Rumah Sakit Mata Cicendo BandungBambang RinandiNo ratings yet
- Klasifikasi Impaksi Caninus Rahang Atas Pada Pemeriksaan Radiograf Panoramik Dan CBCT Sebagai Penunjang OdontomyDocument8 pagesKlasifikasi Impaksi Caninus Rahang Atas Pada Pemeriksaan Radiograf Panoramik Dan CBCT Sebagai Penunjang OdontomyAlsya Yulia RosidiNo ratings yet
- Contemporary Management Pediatric Craniofacial InjuriesDocument8 pagesContemporary Management Pediatric Craniofacial InjuriesTabishur RahmanNo ratings yet
- The Clinical Application A Tooth-Size Analysis: IntroductiokDocument26 pagesThe Clinical Application A Tooth-Size Analysis: Introductiokapi-26468957No ratings yet
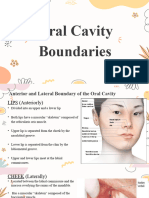
- Oral Cavity BoundariesDocument8 pagesOral Cavity BoundariesLean Edrielle BillonesNo ratings yet
- Dental Record ChartDocument4 pagesDental Record ChartJacqueline Acera Balingit67% (3)
- Components of Frankels Function Regulator and Twin BlockDocument73 pagesComponents of Frankels Function Regulator and Twin BlockSrishti Syal100% (1)
- Submental Intubation.20150306120342Document5 pagesSubmental Intubation.20150306120342dini anitaNo ratings yet
- 'Dissertation - SynopsisDocument11 pages'Dissertation - SynopsisAjith SmileloverNo ratings yet
- Draft Week 2 AssignmentDocument6 pagesDraft Week 2 Assignmentrosalynashley1826No ratings yet
- 0a. Megatron S4 HPS Complete Solution - Functional Anatomy of The Eye PDFDocument31 pages0a. Megatron S4 HPS Complete Solution - Functional Anatomy of The Eye PDFkirubel hailuNo ratings yet
- Dr. Moni BhargavaDocument1 pageDr. Moni BhargavaAnirudh MittalNo ratings yet
- Review of Face Detection System Using Neural NetworkDocument5 pagesReview of Face Detection System Using Neural NetworkVIVA-TECH IJRINo ratings yet
- Nasal Cavity and Paranasal Sinuses: Anatomy and FunctionDocument17 pagesNasal Cavity and Paranasal Sinuses: Anatomy and FunctionVictor EnachiNo ratings yet
- Materi Science Our SelvesDocument2 pagesMateri Science Our SelvesCIP DriveNo ratings yet
- Regional Anesthesia of The Face: Jeffrey S. Eaton, MD and Roy C. Grekin, MDDocument4 pagesRegional Anesthesia of The Face: Jeffrey S. Eaton, MD and Roy C. Grekin, MDPrajna PNo ratings yet
- Determination of Occlusal Vertical Dimension For Complete Dentures Patients: An Updated ReviewDocument12 pagesDetermination of Occlusal Vertical Dimension For Complete Dentures Patients: An Updated ReviewJohnNo ratings yet
- Spitz, R. A. (1955) - The Primal CavityDocument27 pagesSpitz, R. A. (1955) - The Primal CavitycabaretdadaNo ratings yet
- Inspired 3D Short Film Production - Character Development and DesignDocument41 pagesInspired 3D Short Film Production - Character Development and DesignKadriankNo ratings yet