Hurst 11 - Renal
Hurst 11 - Renal
Download as docx, pdf, or txt
You might also like
- Ati Leadership Proctored Focus ReviewDocument4 pagesAti Leadership Proctored Focus ReviewVin Lorenzo Campbell100% (3)
- Mark KlimekDocument1 pageMark KlimekPascal St Peter NwaorguNo ratings yet
- NCLEX Test Taking StrategiesDocument9 pagesNCLEX Test Taking StrategiesLauren100% (4)
- RACGP Bridging Course AMC PDFDocument97 pagesRACGP Bridging Course AMC PDFAnkita Sinha67% (3)
- Testing Strategies: Hurst Review Services 240Document3 pagesTesting Strategies: Hurst Review Services 240reynold100% (1)
- Hurst BurnsDocument4 pagesHurst BurnsKristin Jones100% (5)
- Nursing Exam Cram Sheet For The NCLEX-RN: 1. Test Information 5. ABG ValuesDocument9 pagesNursing Exam Cram Sheet For The NCLEX-RN: 1. Test Information 5. ABG ValuesGee Angela ZozobradoNo ratings yet
- Complete NotesDocument238 pagesComplete Notesprakash_shr97% (32)
- ATI OB Study GuideDocument26 pagesATI OB Study GuideThelma Jerome100% (1)
- The Chicago Review Press NCLEX-RN Practice Test and ReviewFrom EverandThe Chicago Review Press NCLEX-RN Practice Test and ReviewRating: 4 out of 5 stars4/5 (20)
- OBG Theses TopicsDocument22 pagesOBG Theses TopicsNavya Sanjeeva Reddy100% (4)
- NCLEX-RN For Dummies with Online Practice TestsFrom EverandNCLEX-RN For Dummies with Online Practice TestsRating: 5 out of 5 stars5/5 (1)
- Mind Web Academy - Booster 3Document8 pagesMind Web Academy - Booster 3Charis Gutierrez RodriguezNo ratings yet
- NCLEX (Valerie) PDFDocument18 pagesNCLEX (Valerie) PDFValerie Orengo100% (2)
- Infection Control - NclexDocument4 pagesInfection Control - NclexTashaNo ratings yet
- Prado Random FactsDocument377 pagesPrado Random Factsjkrix100% (2)
- This Study Resource Was Shared Via: Sinus BradycardiaDocument3 pagesThis Study Resource Was Shared Via: Sinus BradycardiaPascal St Peter NwaorguNo ratings yet
- Long Acting Contraceptive Contents of Progesterone HormoneDocument34 pagesLong Acting Contraceptive Contents of Progesterone HormoneJefri SandikaNo ratings yet
- RN Intense Remedial Packet QuestionsDocument85 pagesRN Intense Remedial Packet QuestionsAli Resendiz33% (6)
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Hurst - Content Review - Cardio (Edit)Document8 pagesHurst - Content Review - Cardio (Edit)Elaine NorbergNo ratings yet
- ONCOLOGYDocument6 pagesONCOLOGYRizMarie100% (2)
- ATI Capstone Content Review Tips of The Week 3Document16 pagesATI Capstone Content Review Tips of The Week 3nicki schefflerNo ratings yet
- EndocrineDocument18 pagesEndocrineKristaMaeC.Lazo100% (1)
- Nclex Study GuideDocument4 pagesNclex Study GuideSara Pirman50% (2)
- Capstone ATI EXIT EXAMDocument10 pagesCapstone ATI EXIT EXAMcarol50% (2)
- NCSBN - Pharmacology and ParenteralDocument36 pagesNCSBN - Pharmacology and ParenteralKarissa May Cortez92% (12)
- Medsurg and Pharm HESI ReviewDocument8 pagesMedsurg and Pharm HESI ReviewSarah Vance100% (4)
- Mark K Lecture #2Document16 pagesMark K Lecture #2Melissa Sapp100% (2)
- Nursing Nclex ExamDocument11 pagesNursing Nclex ExamDenisa Viviana Maro100% (1)
- ATI Pharm TIPSDocument17 pagesATI Pharm TIPSmike Gee100% (3)
- Breaking Down The NCLEX QuestionsDocument2 pagesBreaking Down The NCLEX QuestionsKaloy KamaoNo ratings yet
- ATI NotesDocument16 pagesATI NotesMei Sarte100% (1)
- Mother and Baby Labour and Delivery NotesDocument1 pageMother and Baby Labour and Delivery NotesSavanna ChambersNo ratings yet
- 2016module5 PDFDocument24 pages2016module5 PDFAicir Tap100% (1)
- Uworld & Kaplan Nclex RN CardsDocument19 pagesUworld & Kaplan Nclex RN CardsOlgaK100% (1)
- Focus Review For ATIDocument16 pagesFocus Review For ATIphandrew0892% (50)
- Nclex 3500Document4 pagesNclex 3500chitor100% (1)
- Ati #3Document8 pagesAti #3Leah Elizabeth100% (8)
- NCLEX Study GuideDocument7 pagesNCLEX Study Guidemmgoodall22100% (3)
- Sata ListDocument11 pagesSata ListNaidin Catherine De Guzman-AlcalaNo ratings yet
- N53 ATI PHARM 207637583-Ati-PharmacologyDocument26 pagesN53 ATI PHARM 207637583-Ati-PharmacologyWMWrian100% (3)
- Maternity Nclex RN ReviewDocument11 pagesMaternity Nclex RN ReviewKwai Browne100% (7)
- Nclex RNDocument36 pagesNclex RNHR100% (14)
- HURST NCLEX Review FactsDocument6 pagesHURST NCLEX Review FactsNicole Alexis100% (9)
- The Pearls For NCLEX Review PDFDocument32 pagesThe Pearls For NCLEX Review PDFSandhu Sdhu100% (8)
- NCLEX Seminar ManuscriptDocument53 pagesNCLEX Seminar ManuscriptKim Medairos100% (1)
- NCLEX Review ExamplefinalDocument52 pagesNCLEX Review Examplefinalisapatrick8126100% (1)
- NCLEX Test Taking TipsDocument3 pagesNCLEX Test Taking TipsjrilleraNo ratings yet
- ATIDocument9 pagesATIKitesaMedeksa100% (9)
- Scary NCLEX Topics Student Workbook 2020Document23 pagesScary NCLEX Topics Student Workbook 2020Kristen Nate100% (2)
- Day 7 SlidesDocument53 pagesDay 7 SlidesHudson OnsareNo ratings yet
- Ignatavicius Renal QuestionsDocument9 pagesIgnatavicius Renal Questionsboogie02100% (5)
- Nclex ReviewDocument12 pagesNclex ReviewNathalee Walker50% (2)
- Pediatric RemediationDocument5 pagesPediatric RemediationAlvin L. Rozier67% (3)
- Nclex Sata 1 5Document14 pagesNclex Sata 1 5Elizabella Henrietta TanaquilNo ratings yet
- Tips For NCLEX From All NursesDocument2 pagesTips For NCLEX From All NursesPeej Reyes75% (4)
- NCLEX Select All That Apply Practice Exam 4Document8 pagesNCLEX Select All That Apply Practice Exam 4Heather ClemonsNo ratings yet
- ENDOCRINEDocument5 pagesENDOCRINERizMarie100% (3)
- How To PassDocument9 pagesHow To PassPatrick Tera ReyesNo ratings yet
- Chicago Review Press NCLEX-PN Practice Test and ReviewFrom EverandChicago Review Press NCLEX-PN Practice Test and ReviewRating: 4 out of 5 stars4/5 (4)
- Endocrine 10-Day Post Live ModulesDocument15 pagesEndocrine 10-Day Post Live ModulesPascal St Peter Nwaorgu100% (2)
- Metabolic and Endocrine Disorders PDFDocument14 pagesMetabolic and Endocrine Disorders PDFPascal St Peter Nwaorgu100% (2)
- PrioritizationDocument20 pagesPrioritizationPascal St Peter Nwaorgu100% (1)
- Nclex Exam PrepDocument26 pagesNclex Exam PrepPascal St Peter Nwaorgu100% (1)
- Daftar Obat BaksosDocument4 pagesDaftar Obat Baksosandi linaNo ratings yet
- Preeklampsia Eklampsia: April 2018Document16 pagesPreeklampsia Eklampsia: April 2018mariana ulfaNo ratings yet
- Medical TerminologyDocument305 pagesMedical TerminologyDITSARA Child and Elderly Care School100% (2)
- Cold&CoughDocument24 pagesCold&CoughMaria KhawajaNo ratings yet
- Algorithm - Managing A COPD Exacerbation in Primary CareDocument1 pageAlgorithm - Managing A COPD Exacerbation in Primary Caremufidah mawaddahNo ratings yet
- Daftar Obat High AlertDocument3 pagesDaftar Obat High AlertLupus BoyssNo ratings yet
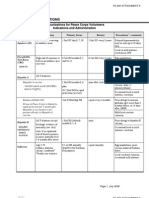
- Peace Corps Vaccine Administration Schedule - TG 300 Medical Technical Guideline 300 - July 2008Document4 pagesPeace Corps Vaccine Administration Schedule - TG 300 Medical Technical Guideline 300 - July 2008Accessible Journal Media: Peace Corps Documents100% (1)
- Educational Topic 15: Ectopic Pregnancy: U 2: O S B: A ODocument4 pagesEducational Topic 15: Ectopic Pregnancy: U 2: O S B: A OStetho LoveNo ratings yet
- NCLEX Updates June 2010Document21 pagesNCLEX Updates June 2010erika_datu100% (1)
- Sexually Transmitted Disease or STI Complete SymtomsDocument11 pagesSexually Transmitted Disease or STI Complete SymtomsPowerzNo ratings yet
- ChickenpoxDocument16 pagesChickenpoxJeet ThuraiNo ratings yet
- Hubungan Preeklamsi Berat Dengan Kelahiran Preterm Di Rumah Sakit Umum Provinsi Nusa Tenggara Barat 2013Document10 pagesHubungan Preeklamsi Berat Dengan Kelahiran Preterm Di Rumah Sakit Umum Provinsi Nusa Tenggara Barat 2013Vera Andri YaniNo ratings yet
- Sensus Pasien Bangsal Periode 29 Januari 2021Document3 pagesSensus Pasien Bangsal Periode 29 Januari 2021Alya MaulidaNo ratings yet
- The Other Diabetes - LADA, or Type 1Document3 pagesThe Other Diabetes - LADA, or Type 1rey_fremyNo ratings yet
- XXXXXDocument14 pagesXXXXXJonas Marvin AnaqueNo ratings yet
- Typhoid FeverDocument13 pagesTyphoid FeverSuhas Ingale0% (1)
- Update Stok TGL 02 Januari 2019Document31 pagesUpdate Stok TGL 02 Januari 2019Hamka AchmadNo ratings yet
- Obat IFARSDocument5 pagesObat IFARSOky Spinola IdroosNo ratings yet
- Upper Respiratory Tract Infection (Urti)Document2 pagesUpper Respiratory Tract Infection (Urti)wen_pilNo ratings yet
- Atopic DermatitisDocument22 pagesAtopic DermatitisBonitavanyNo ratings yet
- Pedia Care Study - Appendix B - Drug StudyDocument8 pagesPedia Care Study - Appendix B - Drug Studyryan100% (1)
- Diuretics:: Acetazolamide Carbonic Anhydrase InhibitorsDocument3 pagesDiuretics:: Acetazolamide Carbonic Anhydrase InhibitorsFatimah FaqihiNo ratings yet
- HepatitisDocument24 pagesHepatitisEric PeprahNo ratings yet
- National Immunization ScheduleDocument3 pagesNational Immunization SchedulescribdscribdtestNo ratings yet
- Daftar PPK CP Per KSM 2019Document10 pagesDaftar PPK CP Per KSM 2019ayuNo ratings yet
- Causes of Blindness and Visual ImpairmentDocument3 pagesCauses of Blindness and Visual ImpairmentMuhammad Amri KautsarNo ratings yet
- Journal Reading: R.Gantira W.Danasasmita Narasumber: Prof. Dr. Dr. Harry Isbagyo, SPPD-KR, KgerDocument22 pagesJournal Reading: R.Gantira W.Danasasmita Narasumber: Prof. Dr. Dr. Harry Isbagyo, SPPD-KR, Kgerira danasasmitaNo ratings yet