T.KR Assignment
T.KR Assignment
Download as docx, pdf, or txt
You might also like
- Bridge Shapes 1400-1900 Wim RaymaekersDocument26 pagesBridge Shapes 1400-1900 Wim Raymaekerswilton100% (1)
- QMBU 301 Quiz 3B SolutionDocument4 pagesQMBU 301 Quiz 3B Solutionekocabas19No ratings yet
- ISC Class XII Computer Science Project JAVA ProgramsDocument77 pagesISC Class XII Computer Science Project JAVA ProgramsTed68% (141)
- HANA Security TechleapDocument23 pagesHANA Security TechleapMahesh BabuNo ratings yet
- Total Hip Arthroplasty 243Document40 pagesTotal Hip Arthroplasty 243jefferyNo ratings yet
- Dynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionFrom EverandDynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionRating: 5 out of 5 stars5/5 (2)
- BUI 2019 Catalog Container HardwareDocument339 pagesBUI 2019 Catalog Container Hardwarejuan.vargas.calle6904No ratings yet
- Applied Biomechanics Arthroplasty: DR Abda ShaikhDocument42 pagesApplied Biomechanics Arthroplasty: DR Abda ShaikhAbida ShaikhNo ratings yet
- PT OrthoDocument129 pagesPT OrthoHarish Kumar NNo ratings yet
- Group Members Habiba Jameel Raffia Tariq Amina Zahoor ZunairaDocument27 pagesGroup Members Habiba Jameel Raffia Tariq Amina Zahoor ZunairaMuiz SaddozaiNo ratings yet
- Total Knee ReplacementDocument23 pagesTotal Knee ReplacementLeoNo ratings yet
- PT Ortho ProblemsDocument129 pagesPT Ortho ProblemsvinaymanNo ratings yet
- Total Knee Replacement Prosthesis AssignmentDocument33 pagesTotal Knee Replacement Prosthesis Assignmentdr neha gaggarNo ratings yet
- امراض سريرية 2 (محاضرة 5)Document3 pagesامراض سريرية 2 (محاضرة 5)studypoolyf2023No ratings yet
- ACL Reconstruction SurgeryDocument8 pagesACL Reconstruction Surgeryjohn hagisNo ratings yet
- Soft Tissue Surgeries: Tendon TransferDocument24 pagesSoft Tissue Surgeries: Tendon TransferManish MauryaNo ratings yet
- ACL ReconstructionDocument24 pagesACL Reconstructionsamabdelaal2000No ratings yet
- ACL Reconstruction 2020Document39 pagesACL Reconstruction 2020محمد عقلNo ratings yet
- Acl Rehab ProtocolDocument18 pagesAcl Rehab Protocolapi-256259376No ratings yet
- TKR Physical TherapyDocument29 pagesTKR Physical TherapyHUZAIFA YAMAANNo ratings yet
- Functions of The Knee JointDocument40 pagesFunctions of The Knee JointAlfred JacksonNo ratings yet
- ACL Reconstruction ProtocolDocument23 pagesACL Reconstruction ProtocolRoberto Tommasini100% (2)
- Completari Artroplastie SoldDocument22 pagesCompletari Artroplastie Soldanasimona284No ratings yet
- Department: Sarhad Institute of Allied Health Sciences Program:DPT - BDocument5 pagesDepartment: Sarhad Institute of Allied Health Sciences Program:DPT - BIjaz KhanNo ratings yet
- Knee Replacement / Arthroplasty: Current PositionDocument20 pagesKnee Replacement / Arthroplasty: Current PositionFerdiriva HamzahNo ratings yet
- Total Knee Replacement Brochure PDFDocument2 pagesTotal Knee Replacement Brochure PDFapi-260874114No ratings yet
- Knee Arthroplasty 2Document26 pagesKnee Arthroplasty 2EktaraNo ratings yet
- 2. Upper Extremity OrthosisDocument125 pages2. Upper Extremity Orthosisimanishfaq200No ratings yet
- Q&A About Total Knee ReplacementDocument4 pagesQ&A About Total Knee ReplacementDrManoj JagarlamudiNo ratings yet
- نسخة light blue creative modern medical clinic presentationDocument33 pagesنسخة light blue creative modern medical clinic presentationFaresNo ratings yet
- Ankle InkDocument4 pagesAnkle InkNysm NydNo ratings yet
- Knee Replacement Surgery: Everything You May Like To Know AboutDocument16 pagesKnee Replacement Surgery: Everything You May Like To Know AboutansfaridNo ratings yet
- Knee Arthroscopy (Meniscectomy) : Anatomy and BiomechanicsDocument9 pagesKnee Arthroscopy (Meniscectomy) : Anatomy and Biomechanicsbayan salahNo ratings yet
- 2.Hip arthroplastyDocument45 pages2.Hip arthroplastyzeyad ismailNo ratings yet
- Prosthesis: Presented by Dr. Chiranjeevi.JDocument63 pagesProsthesis: Presented by Dr. Chiranjeevi.JchirusdunnaNo ratings yet
- Case Study TKRDocument22 pagesCase Study TKRInspirasi KhadijahNo ratings yet
- Askep Klien Total Hip ReplacementDocument55 pagesAskep Klien Total Hip ReplacementAmalia RosaNo ratings yet
- Rehab AclDocument71 pagesRehab AclQuang TranNo ratings yet
- Rehabilitation Case Study Shang Shian Hsieh 80785Document4 pagesRehabilitation Case Study Shang Shian Hsieh 80785Max HsiehNo ratings yet
- Askep Klien Total Hip Replacement: Ns. Mulia Hakam, SP - Kep MBDocument55 pagesAskep Klien Total Hip Replacement: Ns. Mulia Hakam, SP - Kep MBfebriaNo ratings yet
- After Surgery Rehabilitation Program MPFL ReconstructionDocument12 pagesAfter Surgery Rehabilitation Program MPFL ReconstructionNedelcu NicolaeNo ratings yet
- PLC InjuryDocument5 pagesPLC InjuryTeng HanNo ratings yet
- ARTHROPLASTYDocument39 pagesARTHROPLASTYArathyNo ratings yet
- Hip ArthroplastyDocument24 pagesHip ArthroplastyshamoonNo ratings yet
- Anterior Cruciate Ligament Surgery: Trauma & Orthopaedic DirectorateDocument38 pagesAnterior Cruciate Ligament Surgery: Trauma & Orthopaedic DirectorateSzilvia MartonosNo ratings yet
- ArthroplastyDocument64 pagesArthroplastyAmit Kochhar80% (5)
- Lecture 1 Knee OrthosesDocument50 pagesLecture 1 Knee OrthosesAlfred JacksonNo ratings yet
- Knee Injuries ManagementDocument30 pagesKnee Injuries ManagementRehab NaeemNo ratings yet
- ORTHOSIS - and ProthesisDocument112 pagesORTHOSIS - and Prothesismanjukumard2007100% (1)
- Osteoarthritis 2Document35 pagesOsteoarthritis 2khushi ranaNo ratings yet
- Treatment: Home TreatmentsDocument3 pagesTreatment: Home TreatmentsDhimas Reyhan Putra SayudhaNo ratings yet
- Surgical Treatment of ClubfootDocument49 pagesSurgical Treatment of Clubfootvishwas dabasNo ratings yet
- Knee Injuries Part 1Document38 pagesKnee Injuries Part 1meenoNo ratings yet
- Arthoplasty THRDocument30 pagesArthoplasty THRnimra rashidNo ratings yet
- Post-Operative Exercise Program: Knee Joint Replacement SurgeryDocument16 pagesPost-Operative Exercise Program: Knee Joint Replacement SurgeryRamses DagoyNo ratings yet
- Total Elbow Arthroplasty and RehabilitationDocument5 pagesTotal Elbow Arthroplasty and RehabilitationMarina ENo ratings yet
- Qindeel Fatima 102 Sports PT AssignmentDocument16 pagesQindeel Fatima 102 Sports PT AssignmentQindeel FatimaNo ratings yet
- How To Tackle Knee Injury Without Causing Further Trouble To Your KneeDocument4 pagesHow To Tackle Knee Injury Without Causing Further Trouble To Your Kneefoozballer1909No ratings yet
- Trauma-fractures and sprainDocument26 pagesTrauma-fractures and sprainShahana SunijaNo ratings yet
- Patellectomy RehabDocument29 pagesPatellectomy RehabKhateeja Tul KubraNo ratings yet
- ACL InjuryDocument42 pagesACL InjuryRishabh VermaNo ratings yet
- Knee Replacement Surgery, A Simple Guide To The Procedure And Related ConditionsFrom EverandKnee Replacement Surgery, A Simple Guide To The Procedure And Related ConditionsNo ratings yet
- Knee Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentsFrom EverandKnee Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Improvised TreatmentsNo ratings yet
- Tips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointFrom EverandTips for Everyday Life and Sports With an Artificial Joint: Expert guidebook for dealing with a prosthesis for patients with a new hip or knee jointNo ratings yet
- Trigonometry (M102) Course Specification: A2. Enumerate The Application of TrigonometryDocument5 pagesTrigonometry (M102) Course Specification: A2. Enumerate The Application of TrigonometryjimjimNo ratings yet
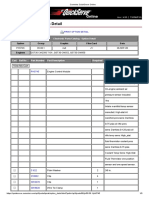
- Parts Catalog - Option DetailDocument3 pagesParts Catalog - Option DetailmunhNo ratings yet
- Risk Assessmnet RecrystallizationDocument3 pagesRisk Assessmnet Recrystallizationh9g886qdnpNo ratings yet
- Tezpur University: Result Sheet Autumn 2009Document37 pagesTezpur University: Result Sheet Autumn 2009Deepjoy DasNo ratings yet
- Talking About Food Taste and TextureDocument13 pagesTalking About Food Taste and TextureSepfi SepfianiNo ratings yet
- Life Sciences Gr.11 Lesson 2 Basic Structure of BacteriaDocument11 pagesLife Sciences Gr.11 Lesson 2 Basic Structure of Bacteriatmalatji106No ratings yet
- Week 10-12 TQMDocument7 pagesWeek 10-12 TQMKrisha Mabel TabijeNo ratings yet
- Motley: Presented By:-Ankush Gupta Abhinav Upadhyay Ankesh Dave Ankit DubeyDocument46 pagesMotley: Presented By:-Ankush Gupta Abhinav Upadhyay Ankesh Dave Ankit DubeyAnkush GuptaNo ratings yet
- 02 Worksheet 2 BSCPE G402 UMPAD CHRISTIANDocument3 pages02 Worksheet 2 BSCPE G402 UMPAD CHRISTIANumpadchristian29No ratings yet
- Media Ownership EssayDocument3 pagesMedia Ownership EssayAnonymous tMLuEVVniNo ratings yet
- Cambridge IGCSE Mathematics Core and Extended by Ric Pimental Terry WallDocument2 pagesCambridge IGCSE Mathematics Core and Extended by Ric Pimental Terry WallKishani SarmilanNo ratings yet
- New Multidimensional Functional Diversity Indices For A Multifaceted Framework in Functional EcologyDocument12 pagesNew Multidimensional Functional Diversity Indices For A Multifaceted Framework in Functional EcologyDaniel Florez TellezNo ratings yet
- Rohit DSA ManualDocument102 pagesRohit DSA Manualjayswalrohit502No ratings yet
- Navigation - Master DataDocument2 pagesNavigation - Master DatagenfinNo ratings yet
- CHAPTER 3 - Science, Technology and Nation-Building Preliminary ActivityDocument3 pagesCHAPTER 3 - Science, Technology and Nation-Building Preliminary ActivityNikki Marie A. CabahugNo ratings yet
- ES Exercise 23-24副本 2Document47 pagesES Exercise 23-24副本 2singyuetchan05No ratings yet
- 60Hz Standard Frequency of Calibration Using MM5369 - ElecCircuitDocument1 page60Hz Standard Frequency of Calibration Using MM5369 - ElecCircuitChanna PrasadNo ratings yet
- Bisleri ProjectDocument78 pagesBisleri ProjectSangit MararNo ratings yet
- +1-657-529-2372 Buy TestDaF Certificate Without Exam in JordanDocument10 pages+1-657-529-2372 Buy TestDaF Certificate Without Exam in JordanLouis KimengzNo ratings yet
- Research DesignDocument3 pagesResearch Designjonjon.manlapasNo ratings yet
- This Study Resource WasDocument4 pagesThis Study Resource WasKoshi SugawaraNo ratings yet
- Deep Security AMEA Partner Handbook1.5Document40 pagesDeep Security AMEA Partner Handbook1.5Rooney NascimentoNo ratings yet
- SKN - PCC - Class 11 Physics - Unit 1 Nature of Physical World and MeasurementDocument3 pagesSKN - PCC - Class 11 Physics - Unit 1 Nature of Physical World and Measurementlohitgenius08No ratings yet
- Criteria For The Evaluation of Damage and Remaining Life in Reformer FurnaceDocument9 pagesCriteria For The Evaluation of Damage and Remaining Life in Reformer FurnaceAndrea CalderaNo ratings yet
- Economics Question Bank 2024Document26 pagesEconomics Question Bank 2024Aru PalNo ratings yet