Skin PDF
Skin PDF
Download as pdf or txt
You might also like
- Veterinary Forensic Medicine and Forensic Sciences by Jason H. Byrd (Editor) Patricia Norris (Editor) Nancy Bradley-Siemens (Editor)Document497 pagesVeterinary Forensic Medicine and Forensic Sciences by Jason H. Byrd (Editor) Patricia Norris (Editor) Nancy Bradley-Siemens (Editor)Mae PimentelNo ratings yet
- Primary and Secondary Skin Lesions - IJDocument43 pagesPrimary and Secondary Skin Lesions - IJThanh Thảo Huỳnh ThịNo ratings yet
- Table of Differentiation of ParasitesDocument18 pagesTable of Differentiation of ParasitesManuel RendonNo ratings yet
- Erythema NodosumDocument42 pagesErythema Nodosummedpedshospitalist100% (1)
- Ncvms Approved Constitution and BylawsDocument12 pagesNcvms Approved Constitution and BylawsRoyd Joseph R. MosasoNo ratings yet
- DA Sistemik TerapiDocument11 pagesDA Sistemik TerapiariyatiNo ratings yet
- Ghid Anestezie Locala PDFDocument19 pagesGhid Anestezie Locala PDFanaNo ratings yet
- Skintox Practiceguidelines EGFR SCCDocument17 pagesSkintox Practiceguidelines EGFR SCCFelipe Scholz RamosNo ratings yet
- Dermnet NZ: Special Stains and TestsDocument4 pagesDermnet NZ: Special Stains and TestsRaja Sekaran DuraiNo ratings yet
- Tumors DR Ahmed KamelDocument98 pagesTumors DR Ahmed KamelABDALRAHMAN ABDALLAH KASEMNo ratings yet
- List of Dermatology Differential Diagnosis and Signs in DermatologyDocument54 pagesList of Dermatology Differential Diagnosis and Signs in DermatologyAhmadq76No ratings yet
- Dermatology Lectures JRRMMCDocument10 pagesDermatology Lectures JRRMMCGi Em100% (1)
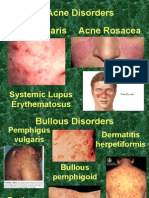
- Acne Vulgaris Acne Rosacea Acne Disorders: Systemic Lupus ErythematosusDocument19 pagesAcne Vulgaris Acne Rosacea Acne Disorders: Systemic Lupus Erythematosusapi-26938624No ratings yet
- Chapter-03 Acneiform EruptionDocument6 pagesChapter-03 Acneiform EruptionSylvia DiamondNo ratings yet
- AAD BF Paisley Tie DiagnosisDocument2 pagesAAD BF Paisley Tie Diagnosiskahkashanahmed065No ratings yet
- Derma Final 2021 (19th, 25th of May)Document91 pagesDerma Final 2021 (19th, 25th of May)Mr.FantasthiccNo ratings yet
- Derma MegatableDocument21 pagesDerma MegatableNicole ChanNo ratings yet
- Paraneoplastic DermatosesDocument57 pagesParaneoplastic DermatosesMohamed Riyaz100% (1)
- LALA Megatable DermaDocument39 pagesLALA Megatable DermaJorelle MarquezNo ratings yet
- The 3rd Year Derma Missing TableDocument6 pagesThe 3rd Year Derma Missing TableEmil GulmaticoNo ratings yet
- Phototherapy For Dermatologic ConditionsDocument18 pagesPhototherapy For Dermatologic ConditionsSeth MosebyNo ratings yet
- Dermatology Imp Images NEET PGDocument5 pagesDermatology Imp Images NEET PGSmrithi ThriloNo ratings yet
- Topical Antibiotics in DermatologyDocument19 pagesTopical Antibiotics in DermatologyJejem Marandra EmkamasNo ratings yet
- DR Pallavi - Dermatology FMGEDocument74 pagesDR Pallavi - Dermatology FMGEVickyNo ratings yet
- Melanocytic TumorsDocument254 pagesMelanocytic TumorsmixandgoNo ratings yet
- General Considerations For Topical PreparationsDocument6 pagesGeneral Considerations For Topical PreparationsOccamsRazorNo ratings yet
- Dermatology Revision 2Document49 pagesDermatology Revision 2Bahaa Shaaban100% (2)
- Eczema, Psoriasis, Cutaneous Infections, Acne, and Other Common Skin DisordersDocument6 pagesEczema, Psoriasis, Cutaneous Infections, Acne, and Other Common Skin DisordersElrey InocianNo ratings yet
- Palmoplantar KeratodermaDocument4 pagesPalmoplantar KeratodermakurutalaNo ratings yet
- HirsutismDocument86 pagesHirsutismBella AgustinNo ratings yet
- Dermatology Mcqs For PGDocument204 pagesDermatology Mcqs For PGjusta7863No ratings yet
- Derm StuffDocument7 pagesDerm StuffSudesna Roy ChowdhuryNo ratings yet
- An Approach To The Patient With ErythrodermaDocument42 pagesAn Approach To The Patient With ErythrodermaShakilNo ratings yet
- Anti Fungal DrugsDocument6 pagesAnti Fungal Drugsbilal ahmadNo ratings yet
- Tumours of Skin: DR F Bhatti Pennine VTS Sept 08Document39 pagesTumours of Skin: DR F Bhatti Pennine VTS Sept 08pfxbkNo ratings yet
- Spongiotic Dermatitis: Aka EczemaDocument8 pagesSpongiotic Dermatitis: Aka EczemafadoNo ratings yet
- Clinical Pearls DermatologíamatologyDocument4 pagesClinical Pearls DermatologíamatologyMaritza24No ratings yet
- Acne Vulgaris: Basic Dermatology CurriculumDocument58 pagesAcne Vulgaris: Basic Dermatology CurriculumJhoel Jhonatan Torres MuñozNo ratings yet
- AAD Atopic Dermatitis - Phototherapy and Systemic Agents 2014Document42 pagesAAD Atopic Dermatitis - Phototherapy and Systemic Agents 2014Yan Zhen YuanNo ratings yet
- Superficial and Deep Perivascular DermatitisDocument55 pagesSuperficial and Deep Perivascular DermatitisMarnie RoviraNo ratings yet
- Infectious DermatologyDocument206 pagesInfectious DermatologyAaron Christian Earl VillosoNo ratings yet
- Steroid Pulse Therapies in DermatologyDocument4 pagesSteroid Pulse Therapies in DermatologyWelly WijayantiNo ratings yet
- Srinadh Neonatal Skin Conditions FinalDocument110 pagesSrinadh Neonatal Skin Conditions FinalSrinadh Pragada100% (1)
- Erythema MultiformeDocument29 pagesErythema MultiformeSurabhi Sharma100% (1)
- 3) Genodermatosis - Dr. Darseem: NeurofibromatosisDocument4 pages3) Genodermatosis - Dr. Darseem: NeurofibromatosisOman ArifNo ratings yet
- What Is A RashDocument8 pagesWhat Is A RashJudi Ann MagsacayNo ratings yet
- Miliaria, Leucoplakia, PPPDocument44 pagesMiliaria, Leucoplakia, PPPcute100% (1)
- Dermatology PDFDocument23 pagesDermatology PDFjonyNo ratings yet
- 9-Patologi Skin PDFDocument34 pages9-Patologi Skin PDFririnNo ratings yet
- New Criteria For Lupus: The Author(s) 2020Document8 pagesNew Criteria For Lupus: The Author(s) 2020Kok Hui DiongNo ratings yet
- Fungal InfectionsDocument9 pagesFungal InfectionsCoral Srinivasa RamaluNo ratings yet
- Introduction To Dermatology Assessment of A Dermatologic PatientDocument86 pagesIntroduction To Dermatology Assessment of A Dermatologic PatientAtif100% (1)
- Vesiculobullous Disorders in Children2Document5 pagesVesiculobullous Disorders in Children2Luciana FernandesNo ratings yet
- Dermatology Revision E6.5 @theboggusdocDocument36 pagesDermatology Revision E6.5 @theboggusdockhushi koliNo ratings yet
- Clinico-Epidemiological Study of Dermatophytosis in Teaching Hospital of North KarnatakaDocument4 pagesClinico-Epidemiological Study of Dermatophytosis in Teaching Hospital of North KarnatakaAldo NovaNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMishaNo ratings yet
- Sqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZDocument19 pagesSqweqwesf Erwrewfsdfs Adasd Dhe: Dermnet NZkdwazirNo ratings yet
- Dermatology and Venerology Notes 4Document111 pagesDermatology and Venerology Notes 4SpyrosNo ratings yet
- Gyne - Case 15 Benign Lesions of The Vulva & VaginaDocument2 pagesGyne - Case 15 Benign Lesions of The Vulva & Vaginacbac1990No ratings yet
- Leishmaniasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLeishmaniasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Clinical Cases in Pigmentary DisordersFrom EverandClinical Cases in Pigmentary DisordersTorello LottiNo ratings yet
- SLE SketchyDocument2 pagesSLE SketchyLanaAmerieNo ratings yet
- Ah PDFDocument134 pagesAh PDFLanaAmerieNo ratings yet
- Truelearn Stuff PDFDocument16 pagesTruelearn Stuff PDFLanaAmerieNo ratings yet
- Cluster of Lesions, PapularDocument3 pagesCluster of Lesions, PapularLanaAmerieNo ratings yet
- Congenital Anomalies of Kidney and Lowe Urinary TractDocument2 pagesCongenital Anomalies of Kidney and Lowe Urinary TractLanaAmerieNo ratings yet
- Table 1: Infective Endocarditis Non Infective Myocarditis Myocardidits PericarditisDocument3 pagesTable 1: Infective Endocarditis Non Infective Myocarditis Myocardidits PericarditisLanaAmerieNo ratings yet
- "Mapping The Nephron" Cellular Templates: Gina Bartoni Lana Daniel ShinDocument11 pages"Mapping The Nephron" Cellular Templates: Gina Bartoni Lana Daniel ShinLanaAmerieNo ratings yet
- Macules Macules and Papules Papules VesiclesDocument6 pagesMacules Macules and Papules Papules VesiclesLanaAmerieNo ratings yet
- RNL DruDocument1 pageRNL DruLanaAmerieNo ratings yet
- OPP - Lab - Counterstrain - Ribs, Anterior, PosteriorDocument1 pageOPP - Lab - Counterstrain - Ribs, Anterior, PosteriorLanaAmerieNo ratings yet
- Integumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemDocument6 pagesIntegumentary Lec 1: Overview of The Integument: A-Integumentary (Skin) SystemLanaAmerieNo ratings yet
- Urinery IncontinsetenceDocument1 pageUrinery IncontinsetenceLanaAmerieNo ratings yet
- AvianInsightVol1 05Document2 pagesAvianInsightVol1 05Bryan NicollNo ratings yet
- What Is The Flu? How Is The Flu Spread?Document2 pagesWhat Is The Flu? How Is The Flu Spread?porfirio ruizNo ratings yet
- Aprendo en Casa Semana 2Document7 pagesAprendo en Casa Semana 2Yesi GNo ratings yet
- Pns Code of Good Animal Husbandry Practices For Chicken - Broilers and LayersDocument10 pagesPns Code of Good Animal Husbandry Practices For Chicken - Broilers and LayersOliver TalipNo ratings yet
- Directory of Avma Listed Veterinary Colleges of The World: NangarharDocument23 pagesDirectory of Avma Listed Veterinary Colleges of The World: NangarharMuneebNo ratings yet
- Biologi Bordetella PertussisDocument7 pagesBiologi Bordetella PertussisSetyadinda Putri MalindaNo ratings yet
- Avion FluDocument1 pageAvion FluImaan RiazNo ratings yet
- The Rise of Veterinary ForensicsDocument40 pagesThe Rise of Veterinary ForensicsMateoNo ratings yet
- English Task "Factual Report" About Coronaviruses: / By: M.Aijul Furqan Xiipa2Document3 pagesEnglish Task "Factual Report" About Coronaviruses: / By: M.Aijul Furqan Xiipa2Aijul FurqanNo ratings yet
- Febrele HemoragiceDocument23 pagesFebrele HemoragicegvfhgNo ratings yet
- Research Assessment 10Document2 pagesResearch Assessment 10api-523475875No ratings yet
- Animal Movements WorkbookDocument20 pagesAnimal Movements WorkbookAdam AdhaNo ratings yet
- Daftar Pustaka PertusisDocument1 pageDaftar Pustaka PertusisErica PuteriNo ratings yet
- Introduction To ImmunologyDocument9 pagesIntroduction To ImmunologyDr-Rmz RabadiNo ratings yet
- ToxoplasmosisDocument27 pagesToxoplasmosisKnjigeNo ratings yet
- PNS - Bafs 267.2022 - PNS Swine - Good Animal Husbandry Practices (GAHP)Document25 pagesPNS - Bafs 267.2022 - PNS Swine - Good Animal Husbandry Practices (GAHP)Johana Pinagayao AngkadNo ratings yet
- Canine DiseasesDocument5 pagesCanine Diseasessambhaji1976No ratings yet
- Acute Respiratory InfectionsDocument22 pagesAcute Respiratory InfectionsKumara GuruNo ratings yet
- Control of Drugs and Cosmetics Regulations 1984 (Amendment 2009)Document16 pagesControl of Drugs and Cosmetics Regulations 1984 (Amendment 2009)NasuhaNo ratings yet
- CV - DR Rahul UpdatedDocument3 pagesCV - DR Rahul UpdatedDrRahul PaulNo ratings yet
- MumpsDocument1 pageMumpsFikri PutroNo ratings yet
- @heto Pala Ung Unang Comment Ni Sir Sa Inot Kong Consultation Na Yaon Dyan Sa Baba Kang Comment Ni Sir,,, Hahah, Thank You AiraDocument6 pages@heto Pala Ung Unang Comment Ni Sir Sa Inot Kong Consultation Na Yaon Dyan Sa Baba Kang Comment Ni Sir,,, Hahah, Thank You Airabaoshi3382No ratings yet
- Herpes Simplex SymptomsDocument3 pagesHerpes Simplex SymptomsInes JianaNo ratings yet
- Resume Holly Standeford For KisdDocument3 pagesResume Holly Standeford For Kisdapi-340637026No ratings yet
- Gape WormDocument4 pagesGape WormNjoku IykeNo ratings yet
- WSJ - Printing Declawing Cats Provokes A Billion-Dollar DebateDocument4 pagesWSJ - Printing Declawing Cats Provokes A Billion-Dollar DebateTesy MctestersonNo ratings yet
- K - 12 Grade: California Immunization Requirements ForDocument2 pagesK - 12 Grade: California Immunization Requirements Forjulian14No ratings yet
- tmp8237 TMPDocument10 pagestmp8237 TMPFrontiersNo ratings yet