Blood Gas Analysis: Respiratory Disorders
Blood Gas Analysis: Respiratory Disorders
Download as docx, pdf, or txt
You might also like
- A Rational Approach 2 ND EditionDocument125 pagesA Rational Approach 2 ND Editionstephanie_bonner_2100% (2)
- Test Bank CardioDocument16 pagesTest Bank CardioLudwigJayBarayuga86% (7)
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Research Paper: How Using Art Making As A Coaching Tool Supports Client LearningDocument12 pagesResearch Paper: How Using Art Making As A Coaching Tool Supports Client LearningInternational Coach AcademyNo ratings yet
- Arterial Blood Gas.ppt1.Document52 pagesArterial Blood Gas.ppt1.Raj PandiyanNo ratings yet
- Arterial Blood Gas - ppt1Document53 pagesArterial Blood Gas - ppt1Madhuri100% (2)
- Arterialbloodgas 190213090749Document53 pagesArterialbloodgas 190213090749annisa pahlevianaNo ratings yet
- Acidosis Alkalosis BiochemistryDocument31 pagesAcidosis Alkalosis BiochemistryliyaNo ratings yet
- Biochemical Basis of Acidosis and Alkalosis: Evaluating Arterial Blood Gases Data & ABD'sDocument46 pagesBiochemical Basis of Acidosis and Alkalosis: Evaluating Arterial Blood Gases Data & ABD'sFaisal AliNo ratings yet
- Blood Gas AnalysisDocument5 pagesBlood Gas Analysissraji64No ratings yet
- Arterial Blood GasDocument33 pagesArterial Blood GaskartikaparamitaNo ratings yet
- Abg AnalysisDocument65 pagesAbg AnalysisSyed Farooque AliNo ratings yet
- Acid-Base DisorderDocument33 pagesAcid-Base DisorderSafaa AlzaiadyNo ratings yet
- Abg InterpretationDocument13 pagesAbg Interpretationgwapz23No ratings yet
- Blood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical CareDocument48 pagesBlood Gases (Abgs) Interpretation Dr/Baha Eldin Hassan Ahmed Fellow Paediatric Critical Carehagir alhajNo ratings yet
- Abg 151118185050 Lva1 App6891Document52 pagesAbg 151118185050 Lva1 App6891RAMJIBAN YADAVNo ratings yet
- Abg InterpretationDocument52 pagesAbg InterpretationRAMJIBAN YADAVNo ratings yet
- Arterial Blood Gas: Interpretation and Clinical ImplicationsDocument112 pagesArterial Blood Gas: Interpretation and Clinical ImplicationsmatrixtrinityNo ratings yet
- Acid Base InterpretationDocument46 pagesAcid Base InterpretationshikhaNo ratings yet
- Y5 RN - Abgs 27oct2010Document5 pagesY5 RN - Abgs 27oct2010Canh VanNo ratings yet
- Blood Gas AnalysisDocument52 pagesBlood Gas AnalysisKresna Dharma SuryanaNo ratings yet
- Acid-Base Balance & Blood GasesDocument39 pagesAcid-Base Balance & Blood GasesSulaiman TahsinNo ratings yet
- Abg 3Document43 pagesAbg 3Montasir AhmedNo ratings yet
- ABGS Arterial Blood GasesDocument27 pagesABGS Arterial Blood GasesMuhammad asif samiNo ratings yet
- Acid/Base and ABG Interpretation Made SimpleDocument45 pagesAcid/Base and ABG Interpretation Made SimpleekadtorNo ratings yet
- Arterial Blood Gas Analysis-1Document74 pagesArterial Blood Gas Analysis-1ArunNo ratings yet
- Acid Base BalanceDocument13 pagesAcid Base BalanceRashed ShatnawiNo ratings yet
- Oladapo Olayemi Fwacs, Fmcog (Nig), MPH (Johns Hopkins) Professor Dept of Obstetrics and Gynaecology, University College Hospital, IbadanDocument30 pagesOladapo Olayemi Fwacs, Fmcog (Nig), MPH (Johns Hopkins) Professor Dept of Obstetrics and Gynaecology, University College Hospital, IbadanDayo IdowuNo ratings yet
- Abg by DR Manna, Department of Emergency Medicine, Amrita Institute of Medical Sceinces, Kochi, KeralaDocument50 pagesAbg by DR Manna, Department of Emergency Medicine, Amrita Institute of Medical Sceinces, Kochi, KeralaAETCM Emergency medicine100% (1)
- ABG HandoutDocument7 pagesABG HandoutmarmarminanoNo ratings yet
- 06 PDR3-IM-Arterial-Blood-Gas-ABGDocument7 pages06 PDR3-IM-Arterial-Blood-Gas-ABGAlyanna BlanciaNo ratings yet
- ABG Interpretation FINALDocument41 pagesABG Interpretation FINALmrbalwa419No ratings yet
- Interpretation of Arterial Blood Gases and Acid-Base DisordersDocument44 pagesInterpretation of Arterial Blood Gases and Acid-Base DisordersSuren VishvanathNo ratings yet
- Arterial Blood Gas.Document4 pagesArterial Blood Gas.Sathish KumarNo ratings yet
- ABG InterpretationDocument51 pagesABG InterpretationRaj KumarNo ratings yet
- Acid Base Disorder Practice Problems Notes by Giuls 30Document6 pagesAcid Base Disorder Practice Problems Notes by Giuls 30marcoNo ratings yet
- Acid Base BalaneceDocument11 pagesAcid Base BalaneceHAMMYER ALROKHAMINo ratings yet
- Arterial Blood Gas Interpretation: Presenter-Dr. Garima Aggarwal Resident Iind Yr Department of MedicineDocument43 pagesArterial Blood Gas Interpretation: Presenter-Dr. Garima Aggarwal Resident Iind Yr Department of Medicinefirdaus che daud100% (1)
- Respiratory Acid-Base DisordersDocument13 pagesRespiratory Acid-Base DisordersAlfredo PreciadoNo ratings yet
- Acid BaseDocument6 pagesAcid BaseCarol Solanyi Gacha QuinteroNo ratings yet
- Arterial Blood Gas AnalysisDocument48 pagesArterial Blood Gas AnalysisRishu BujjuNo ratings yet
- Abg Analysis ReviewerDocument21 pagesAbg Analysis ReviewerAyiessa_AJNo ratings yet
- Arterial Blood GasesDocument9 pagesArterial Blood GasesJohn BattleNo ratings yet
- Abg InterpretationDocument52 pagesAbg InterpretationCirugia Cardiovascular NeivaNo ratings yet
- ABG InterpertationDocument14 pagesABG Interpertationapi-3757039100% (1)
- Acid-Base - FDocument14 pagesAcid-Base - Fotiang deniceNo ratings yet
- Stepwise Approach To Acid-Base AnalysisDocument16 pagesStepwise Approach To Acid-Base AnalysisTryanto Amrisal MohammadNo ratings yet
- AbgDocument38 pagesAbgroopaNo ratings yet
- How To Read Arterial Blood Gas .PTDocument36 pagesHow To Read Arterial Blood Gas .PTMohd Erham bin JonohNo ratings yet
- Blood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIDocument39 pagesBlood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIIQBAL HAKKIKINo ratings yet
- Keseimbangan Asam BasaDocument33 pagesKeseimbangan Asam BasaTeguh winarsoNo ratings yet
- LRP CriticalCare Sample2Document46 pagesLRP CriticalCare Sample2Aniket ChoudharyNo ratings yet
- Acid-Base Analysis ExamplesDocument46 pagesAcid-Base Analysis Examplespavi shan gayaNo ratings yet
- Arterial Blood Gas: AnalysisDocument51 pagesArterial Blood Gas: Analysisnaven100% (2)
- Acid-Base Principles and Practical Interpretation in Small Animals - WSAVA2005 - VINDocument9 pagesAcid-Base Principles and Practical Interpretation in Small Animals - WSAVA2005 - VINRhyko DangkuNo ratings yet
- Metabolic AcidosisDocument102 pagesMetabolic AcidosisShajahan SideequeNo ratings yet
- Abg SakshiDocument59 pagesAbg SakshiSakshi GuptaNo ratings yet
- 2016 Acid Base DisordersDocument48 pages2016 Acid Base DisordersbellabelbonNo ratings yet
- Acid-Base (Anesthesia Text) - OpenAnesthesiaDocument12 pagesAcid-Base (Anesthesia Text) - OpenAnesthesiaReddyNo ratings yet
- Acid Base BalanceDocument18 pagesAcid Base BalanceRichard PoonNo ratings yet
- Arterial Blood Gas Analysis: DR - Rakesh Chandra Chaurasia PGT 3 Ims, Bhu Moderator: DR - Manjaree Mishra Asset - ProfDocument64 pagesArterial Blood Gas Analysis: DR - Rakesh Chandra Chaurasia PGT 3 Ims, Bhu Moderator: DR - Manjaree Mishra Asset - ProfArmaanjeet SinghNo ratings yet
- Latchscore Cheat SheetAA95D87460A7Document1 pageLatchscore Cheat SheetAA95D87460A7YogeshRavalNo ratings yet
- EarDocument3 pagesEarYogeshRavalNo ratings yet
- stridor -4Document4 pagesstridor -4YogeshRavalNo ratings yet
- Vascular Lesions in NeonatesDocument15 pagesVascular Lesions in NeonatesYogeshRavalNo ratings yet
- HypocalcemiaDocument3 pagesHypocalcemiaYogeshRavalNo ratings yet
- Ambiguous Genitalia in NeonatesDocument6 pagesAmbiguous Genitalia in NeonatesYogeshRavalNo ratings yet
- Which Is A Really Long Time For A Parent To Count When Their Kid Is Not BreathingDocument6 pagesWhich Is A Really Long Time For A Parent To Count When Their Kid Is Not BreathingYogeshRavalNo ratings yet
- Accidental ExtubationDocument2 pagesAccidental ExtubationYogeshRavalNo ratings yet
- Gastro Oesophageal Reflux (GOR) in Neonates Key MessagesDocument5 pagesGastro Oesophageal Reflux (GOR) in Neonates Key MessagesYogeshRavalNo ratings yet
- Interpret The Abgs in A Stepwise Manner:: Reference ReferenceDocument6 pagesInterpret The Abgs in A Stepwise Manner:: Reference ReferenceYogeshRavalNo ratings yet
- Interpret The Abgs in A Stepwise Manner:: Reference ReferenceDocument3 pagesInterpret The Abgs in A Stepwise Manner:: Reference ReferenceYogeshRavalNo ratings yet
- Developmental DelayDocument4 pagesDevelopmental DelayYogeshRavalNo ratings yet
- Summary of Neurodisability WorkshopDocument6 pagesSummary of Neurodisability WorkshopYogeshRavalNo ratings yet
- Neonatal Stroke (AutoRecovered)Document1 pageNeonatal Stroke (AutoRecovered)YogeshRavalNo ratings yet
- URTIDocument2 pagesURTIYogeshRavalNo ratings yet
- Agenda Peds Update 2018Document1 pageAgenda Peds Update 2018YogeshRavalNo ratings yet
- Important Pediatrics SyndromesDocument11 pagesImportant Pediatrics SyndromesYogeshRavalNo ratings yet
- Research Methodology SyllabusDocument1 pageResearch Methodology SyllabusYogeshRavalNo ratings yet
- IVH Prevention Guidleines1Document3 pagesIVH Prevention Guidleines1YogeshRavalNo ratings yet
- Developmental DelayDocument4 pagesDevelopmental DelayYogeshRavalNo ratings yet
- Generic Care PlanDocument30 pagesGeneric Care PlanMaria Belen Rivera PaspuelNo ratings yet
- What Is A Pilonidal Sinus, What Causes Them and What Are The Symptoms of Pilonidal SinusDocument4 pagesWhat Is A Pilonidal Sinus, What Causes Them and What Are The Symptoms of Pilonidal SinusThavam RatnaNo ratings yet
- Fisiopatología Del Paciente Crítico en 1000 PalabrasDocument14 pagesFisiopatología Del Paciente Crítico en 1000 Palabrascolo_med1077No ratings yet
- Resilienceself-Care ChecklistDocument1 pageResilienceself-Care Checklistapi-743546958No ratings yet
- Soluvit N PIDocument3 pagesSoluvit N PIsigitNo ratings yet
- Chapter 001Document8 pagesChapter 001Lisa SzyszkaNo ratings yet
- IPR2015 00643 FinalDeterminationDocument39 pagesIPR2015 00643 FinalDeterminationTradeHawkNo ratings yet
- TLEDocument13 pagesTLEAnonymous lim7qKW1No ratings yet
- Sekilas Akupunktur Lembaga EstetikDocument30 pagesSekilas Akupunktur Lembaga Estetikiwan santosopsNo ratings yet
- Supportive Psychotherapy in Dementia PDFDocument7 pagesSupportive Psychotherapy in Dementia PDFАнастасия МалащекноNo ratings yet
- 2002 Solution-Focused Brief TherapyDocument9 pages2002 Solution-Focused Brief Therapymgnpni100% (1)
- DengueDocument46 pagesDengueMuhammad Ayub Khan100% (1)
- Aplastic AnemiaDocument26 pagesAplastic AnemiaIrina Moldovan100% (2)
- The Rhinoplasty (Nose Job) ProcedureDocument13 pagesThe Rhinoplasty (Nose Job) ProcedureMart UrsuNo ratings yet
- Notes On Formulation & Evaluation of Floating Microspheres of An Antibiotic DrugDocument66 pagesNotes On Formulation & Evaluation of Floating Microspheres of An Antibiotic DrugkeyurNo ratings yet
- EBOOK - Tinnitus-Miracle - Thomas Coleman 2014Document334 pagesEBOOK - Tinnitus-Miracle - Thomas Coleman 2014Pieter SteenkampNo ratings yet
- Drug Study AdenocarcinomaDocument3 pagesDrug Study AdenocarcinomaJoyce AgorNo ratings yet
- Textbook of Psychological Medicine Fifth EditionDocument44 pagesTextbook of Psychological Medicine Fifth EditionalansparrowhawkNo ratings yet
- Notes For Phar110Document22 pagesNotes For Phar110Abhashni NandaaniNo ratings yet
- Definition and Scope PharmacoepidemiologyDocument23 pagesDefinition and Scope PharmacoepidemiologyKanav Khera100% (7)
- Ayurvedic AcupressureDocument6 pagesAyurvedic AcupressureRana Bose80% (10)
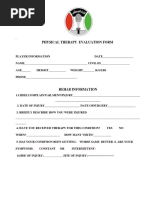
- Physical Therapy Evaluation FormDocument6 pagesPhysical Therapy Evaluation FormRobin MathewNo ratings yet
- Chlamydia GonorrheaDocument3 pagesChlamydia GonorrheaAugene ToribioNo ratings yet
- Proprioceptive Neuromuscular Facilitation (PNF) Lecture (5)Document13 pagesProprioceptive Neuromuscular Facilitation (PNF) Lecture (5)Nistara Singh ChawlaNo ratings yet
- Occupational Therapy Marketing Indian Prospective SRJI Vol 2 Issue 3 Year 2013Document8 pagesOccupational Therapy Marketing Indian Prospective SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNo ratings yet
- STEMI Thrombolysis Protocol STElevation MIDocument6 pagesSTEMI Thrombolysis Protocol STElevation MISurya AtmajaNo ratings yet