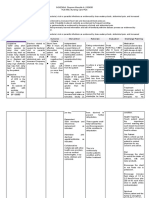
Planning Intervention Rationale Evaluation: Nursing Care Plan Problem Diagnosis
Planning Intervention Rationale Evaluation: Nursing Care Plan Problem Diagnosis
Download as docx, pdf, or txt
You might also like
- Diploma in Nursing AssistantDocument8 pagesDiploma in Nursing Assistantncitindia100% (1)
- Acute Myeloid Leukemia (NCP)Document4 pagesAcute Myeloid Leukemia (NCP)Krisianne Mae Lorenzo Francisco100% (1)
- Rle Worksheet Nursing ProcessDocument6 pagesRle Worksheet Nursing ProcessMARVIE JOY BALUMA CABIOCNo ratings yet
- Guillermo Clinical PathwayDocument5 pagesGuillermo Clinical PathwayLemuel Glenn Bautista100% (1)
- Gonzaga Rlems - NCPDocument3 pagesGonzaga Rlems - NCPShaynne Wencille A. GONZAGANo ratings yet
- NCP-fluid Volume DeficitDocument4 pagesNCP-fluid Volume DeficitChrissa Mae Aranilla MayoNo ratings yet
- DiarrheaDocument3 pagesDiarrheaBert GasalNo ratings yet
- For Printing Jan23Document3 pagesFor Printing Jan23Jhoan OllanoNo ratings yet
- HTP HemoptysisDocument10 pagesHTP HemoptysisみずNo ratings yet
- NCPDocument3 pagesNCPJefferson ManasanNo ratings yet
- NCP: Puerperal InfectionDocument8 pagesNCP: Puerperal InfectionJavie83% (12)
- NCP PediatricDocument5 pagesNCP PediatricSL Hanna NebridaNo ratings yet
- AppendectomyDocument6 pagesAppendectomyapi-3797941100% (10)
- Nursing Care Plan TemplateDocument4 pagesNursing Care Plan TemplatetonnifritzcutamoraNo ratings yet
- Nursing Care Plan: IndependentDocument1 pageNursing Care Plan: IndependentJay Mar BabateNo ratings yet
- Pueperal Sepsis 2022Document42 pagesPueperal Sepsis 2022Joseph MuzabulaNo ratings yet
- 11/04/2019 14/04/2019 Lê Phương Thảo: Present historyDocument7 pages11/04/2019 14/04/2019 Lê Phương Thảo: Present historyThảo LÊNo ratings yet
- Peace Corps MTG 810 Tropical MedicineDocument95 pagesPeace Corps MTG 810 Tropical MedicineAccessible Journal Media: Peace Corps DocumentsNo ratings yet
- Risk For Infection: Objective: - Fever - Lower Back Pain - Pain in Urinating For 1 WeekDocument8 pagesRisk For Infection: Objective: - Fever - Lower Back Pain - Pain in Urinating For 1 WeekJamie HaravataNo ratings yet
- N039-N040 Rejano Nursing Care PlanDocument3 pagesN039-N040 Rejano Nursing Care PlanBianca Marithè RejanoNo ratings yet
- Infection 2Document1 pageInfection 2josh2424No ratings yet
- Marquez, C. BSN 2B Case Study 104Document5 pagesMarquez, C. BSN 2B Case Study 104Caren MarquezNo ratings yet
- Gastrointestinal Tract Infections 1Document17 pagesGastrointestinal Tract Infections 1Sheika Briones GalletaNo ratings yet
- Ob Topic 1 - Pprom - NCPDocument2 pagesOb Topic 1 - Pprom - NCPThelly MargalloNo ratings yet
- CDU Care Plan. UTIDocument7 pagesCDU Care Plan. UTImutiso mutieNo ratings yet
- Dhan Chan NCPDocument3 pagesDhan Chan NCPDhaneanne Marie ChanNo ratings yet
- Potential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Document2 pagesPotential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Karl KiwisNo ratings yet
- F. NCP ProperDocument4 pagesF. NCP ProperAle SandraNo ratings yet
- Candidiasis RHUDocument11 pagesCandidiasis RHUaisa baladjiNo ratings yet
- Discharge Plan (Woundcare)Document3 pagesDischarge Plan (Woundcare)borikaw15No ratings yet
- DX Diarrhea PDFDocument11 pagesDX Diarrhea PDFSherree HayesNo ratings yet
- SIR Q NCM109 Gastrointestinal DisordersDocument9 pagesSIR Q NCM109 Gastrointestinal Disorderssyroise margauxNo ratings yet
- Pae Risk of InfectionDocument3 pagesPae Risk of InfectionScribdTranslationsNo ratings yet
- Place Risk of InfectionDocument3 pagesPlace Risk of InfectionScribdTranslationsNo ratings yet
- Enteric DiseaseDocument2 pagesEnteric DiseaseHazel ZullaNo ratings yet
- DRUG STUDE - CEFA (Echanique)Document1 pageDRUG STUDE - CEFA (Echanique)Echanique, James F.No ratings yet
- Laporan Pendahuluan Asuhan Keperawatan Bayi Dengan BBLR Di Ruang Cempaka 1 Neonatus Rsup SanglahDocument20 pagesLaporan Pendahuluan Asuhan Keperawatan Bayi Dengan BBLR Di Ruang Cempaka 1 Neonatus Rsup SanglahSutariniNo ratings yet
- Gastroenteritis HandoutDocument5 pagesGastroenteritis HandoutAndrea Jane T GarciaNo ratings yet
- Urinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Document9 pagesUrinary Catherization: St. Paul University Dumaguete College of Nursing Dumaguete City First Semester, 2021-2022Franz goNo ratings yet
- NCP (Revised)Document7 pagesNCP (Revised)Mary AllizaNo ratings yet
- Nursing Care Plan (NCP) For A Patient With Acute Renal FailureDocument3 pagesNursing Care Plan (NCP) For A Patient With Acute Renal FailureKian HerreraNo ratings yet
- Sample Case Pres - ScenarioDocument15 pagesSample Case Pres - ScenariogustomonglemonNo ratings yet
- NCP Neonatal SepsisDocument1 pageNCP Neonatal SepsisGen-GenMedranoGirayNo ratings yet
- UTI Nursing CareDocument1 pageUTI Nursing CareRaveenmayiNo ratings yet
- Invanz (Ertapenem)Document2 pagesInvanz (Ertapenem)E100% (1)
- NCP AppendicitisDocument2 pagesNCP Appendicitismnms0708100% (2)
- Rationale The Presence ofDocument24 pagesRationale The Presence ofPia CadornaNo ratings yet
- NCP - Villahermosa - Risk For InfectionDocument5 pagesNCP - Villahermosa - Risk For InfectionJv Jore VillahermosaNo ratings yet
- Fiona Lyca P. Lacson Bsn3D Health Teaching Plan Medication Exercise Treatment Hygiene Out-Patient DietDocument5 pagesFiona Lyca P. Lacson Bsn3D Health Teaching Plan Medication Exercise Treatment Hygiene Out-Patient DietGilianne JimeneaNo ratings yet
- Safari - 19 Apr 2020 at 18:27Document1 pageSafari - 19 Apr 2020 at 18:27Dream Big PrincessNo ratings yet
- XIV. TreatmentDocument2 pagesXIV. TreatmentCharlemagne Louise BuadaNo ratings yet
- Gastroenteritis: Diseases and Conditions: GastroenteritisDocument6 pagesGastroenteritis: Diseases and Conditions: GastroenteritisWen RodsaNo ratings yet
- Natural Treatments for Yeast Infection: How to Cure a Yeast Infection Using Home RemediesFrom EverandNatural Treatments for Yeast Infection: How to Cure a Yeast Infection Using Home RemediesNo ratings yet
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- Dr. Barbara Parasite Cleanse: The Nutritional Guide for Individuals to Treat and Eliminate Parasites and Parasitic Infections with Natural Barbara O’Neill Remedies,Diet and MethodFrom EverandDr. Barbara Parasite Cleanse: The Nutritional Guide for Individuals to Treat and Eliminate Parasites and Parasitic Infections with Natural Barbara O’Neill Remedies,Diet and MethodNo ratings yet
- On Guard: Build Resilience - Boost Immunity - Beat InfectionFrom EverandOn Guard: Build Resilience - Boost Immunity - Beat InfectionNo ratings yet
- The Wonder of Probiotics: A 30-Day Plan to Boost Energy, Enhance Weight Loss, Heal GI Problems, Prevent Disease, and Slow AgingFrom EverandThe Wonder of Probiotics: A 30-Day Plan to Boost Energy, Enhance Weight Loss, Heal GI Problems, Prevent Disease, and Slow AgingNo ratings yet
- Anti-Yeast Diet: A Beginner's 2-Week Step-by-Step for Women, with Curated Recipes and a Sample Meal PlanFrom EverandAnti-Yeast Diet: A Beginner's 2-Week Step-by-Step for Women, with Curated Recipes and a Sample Meal PlanNo ratings yet
- Anti-Yeast Diet for Women: A Beginner's 2-Week Step-by-Step for Women, with Curated Recipes and a Sample Meal PlanFrom EverandAnti-Yeast Diet for Women: A Beginner's 2-Week Step-by-Step for Women, with Curated Recipes and a Sample Meal PlanNo ratings yet
- Comprehensive Insights into Gastroenteritis: Pathogenesis, Management, and Future DirectionsFrom EverandComprehensive Insights into Gastroenteritis: Pathogenesis, Management, and Future DirectionsNo ratings yet
- PBL and NDXDocument15 pagesPBL and NDXJasmin AdoraNo ratings yet
- Guidelines For Management of Endometrial CarcinomaDocument41 pagesGuidelines For Management of Endometrial CarcinomaVeenaNo ratings yet
- Hirschsprung DiseaseDocument44 pagesHirschsprung DiseaseAhmad Abu KushNo ratings yet
- CataractDocument6 pagesCataractSairileenDoradoNo ratings yet
- Gastroenteritis in ChildrenDocument4 pagesGastroenteritis in ChildrenDennifer MadayagNo ratings yet
- Siadh Patient Case - Final1Document43 pagesSiadh Patient Case - Final1api-589685298No ratings yet
- Brain Stem Infarction Clinical CluesDocument9 pagesBrain Stem Infarction Clinical CluesAR KarthickNo ratings yet
- Management of Third Molar Surgery in HIV Positive PatientsDocument4 pagesManagement of Third Molar Surgery in HIV Positive Patientskiara wardanaNo ratings yet
- Ayurvedic Medicine Herbal ProductsDocument26 pagesAyurvedic Medicine Herbal ProductsBond Back CleanersNo ratings yet
- CA Stomach FinalDocument83 pagesCA Stomach Finalrajmv7No ratings yet
- 116 Theory NotesDocument84 pages116 Theory NotesKirstie Goc-ongNo ratings yet
- CH 19 Non-Neoplastic Diseases of Salivary GlandsDocument55 pagesCH 19 Non-Neoplastic Diseases of Salivary GlandsReem E.MNo ratings yet
- Pathology IcsmDocument84 pagesPathology IcsmAlice TangNo ratings yet
- 52 DEPRESSION Yy Edit - 1Document3 pages52 DEPRESSION Yy Edit - 1besar yogyaNo ratings yet
- Depression ToolkitDocument16 pagesDepression ToolkitKaren Raskin Kleiman100% (1)
- 53 Medicine QuestionsDocument27 pages53 Medicine QuestionsFahad2036No ratings yet
- Biology Investigatory ProjectDocument19 pagesBiology Investigatory ProjectSenthil KumarNo ratings yet
- 655 1767 1 PBDocument9 pages655 1767 1 PBFARMASI PRIMA HUSADA SUKOREJONo ratings yet
- BPC-157 A Collection of StudiesDocument28 pagesBPC-157 A Collection of StudiesscribdNo ratings yet
- 2020 Coronavirus Pandemic in Vietnam PDFDocument49 pages2020 Coronavirus Pandemic in Vietnam PDFchandra mohanNo ratings yet
- TiKi TaKa CK Preventive MedicineDocument3 pagesTiKi TaKa CK Preventive MedicinenonsNo ratings yet
- 01 - Measures of Disease OccurrenceDocument16 pages01 - Measures of Disease OccurrenceSaad MotawéaNo ratings yet
- Salmonella IgM ELISA Package InsertDocument2 pagesSalmonella IgM ELISA Package InsertHarnadi WonogiriNo ratings yet
- New Patient Nutrition Assessment Form: Goals and Readiness AssessmentDocument11 pagesNew Patient Nutrition Assessment Form: Goals and Readiness AssessmentAyesha Khan100% (1)
- Cigna Medical Coverage Policy: Electrical Stimulation Therapy and DevicesDocument55 pagesCigna Medical Coverage Policy: Electrical Stimulation Therapy and DevicesDidik HariadiNo ratings yet
- Biliary Tract Surgery in Dogs and CatsDocument5 pagesBiliary Tract Surgery in Dogs and CatsEsther ArifinNo ratings yet
- Summary Mindfulnes SetDocument1 pageSummary Mindfulnes Setjōōstech SLNo ratings yet
- Current Management Strategies For Autonomic DysreflexiaDocument6 pagesCurrent Management Strategies For Autonomic DysreflexiamoutranhabibNo ratings yet