Azithromycin
Azithromycin
Download as pdf or txt
You might also like
- Drug Study CADocument8 pagesDrug Study CAAna Marie Besa Battung-ZalunNo ratings yet
- Cva NCPDocument1 pageCva NCPxiang jinNo ratings yet
- Drug Study-Med WardDocument2 pagesDrug Study-Med WardErnest Brian FernandezNo ratings yet
- Drug Study MontanoDocument4 pagesDrug Study Montanokarl montanoNo ratings yet
- Sapamine CSN Textile Softener: Technical Data SheetDocument5 pagesSapamine CSN Textile Softener: Technical Data Sheetsasko100% (1)
- AzithromycinDocument3 pagesAzithromycinapi-3797941100% (2)
- Acetaminophen (Tylenol)Document2 pagesAcetaminophen (Tylenol)amelia hearonNo ratings yet
- Go Piperacillin-TazobactamDocument4 pagesGo Piperacillin-TazobactamSAMANTHA T. MODESTONo ratings yet
- Grand Case (Sigmoid Adenocarcinoma)Document24 pagesGrand Case (Sigmoid Adenocarcinoma)Leslee Amor EspirituNo ratings yet
- Indacaterol GlycopyrroniumDocument1 pageIndacaterol GlycopyrroniumNeulAskiel FloresNo ratings yet
- NCP Impaired Physical MobilityDocument1 pageNCP Impaired Physical MobilityLorraine Punla PanganNo ratings yet
- Losartan Plus HydrochlorothiazideDocument18 pagesLosartan Plus Hydrochlorothiazidegmsanto7No ratings yet
- Tramadol, Ketorolac, EterocoxibDocument4 pagesTramadol, Ketorolac, EterocoxibEric de JulianNo ratings yet
- NCP OsteosarcomaDocument6 pagesNCP OsteosarcomaNiksNo ratings yet
- SimvastatinDocument1 pageSimvastatinLyka Mae Imbat - PacnisNo ratings yet
- Mucoviscidosis: Children 6 Years: 1 Capsule 2 Times Daily. Capsule Should Be Taken AfterDocument3 pagesMucoviscidosis: Children 6 Years: 1 Capsule 2 Times Daily. Capsule Should Be Taken AfterMary Pauline MacaspacNo ratings yet
- MethimazoleDocument5 pagesMethimazoleapi-300595323No ratings yet
- Discharge PlanDocument1 pageDischarge PlanJullie Anne SantoyoNo ratings yet
- Urinalysis: PurposeDocument6 pagesUrinalysis: PurposebobtagubaNo ratings yet
- 500 Medical Surgical Sample QuestionDocument323 pages500 Medical Surgical Sample QuestionElizabella Henrietta TanaquilNo ratings yet
- NCP HemorrhoidsDocument2 pagesNCP Hemorrhoidsnurse_yramenaj0% (1)
- Ortho HypoCase Drug StudyDocument10 pagesOrtho HypoCase Drug StudySolsona Natl HS MaanantengNo ratings yet
- 6 EsomeprazolDocument2 pages6 EsomeprazolHaring Jamir SendadNo ratings yet
- Drug StudyDocument5 pagesDrug StudyMadsNo ratings yet
- CLobazamDocument7 pagesCLobazamnika0126No ratings yet
- Drug Study (Pedia)Document7 pagesDrug Study (Pedia)Caurrine Monsalud100% (1)
- Sal But AmolDocument2 pagesSal But AmolCalimlim KimNo ratings yet
- Drug 101Document12 pagesDrug 101Alyzza DagoyNo ratings yet
- Kabiven: (Amino Acids, Electrolytes, Dextrose and Lipid Injectable Emulsion), For Intravenous UseDocument24 pagesKabiven: (Amino Acids, Electrolytes, Dextrose and Lipid Injectable Emulsion), For Intravenous UseDivine Mercy De JulianNo ratings yet
- Seizure Disorders and Management in Primary Health CareDocument83 pagesSeizure Disorders and Management in Primary Health CareChidi MbatuegwuNo ratings yet
- Drug Study CytotecDocument2 pagesDrug Study CytotecJahmil DulatreNo ratings yet
- Drug StudyDocument5 pagesDrug StudyJanine Erika Julom BrillantesNo ratings yet
- Drug StudyDocument1 pageDrug StudyMaui LopezNo ratings yet
- Job Application Letter For Nurse SampleDocument1 pageJob Application Letter For Nurse SampleJose Luis HernandezNo ratings yet
- Introduction Acute BronchitisDocument19 pagesIntroduction Acute BronchitisFarida EbrahimNo ratings yet
- Warfarin - Drug InformationDocument23 pagesWarfarin - Drug InformationTestesteNo ratings yet
- VenoferDocument13 pagesVenoferLuciano H.Vivas M.No ratings yet
- JM CarbocisteineDocument1 pageJM CarbocisteineKatrina MagtalasNo ratings yet
- Drug StudyDocument2 pagesDrug Studydwyane0033No ratings yet
- Patient Education: by Dr. Nadia BassuoniDocument32 pagesPatient Education: by Dr. Nadia Bassuoniاسامة محمد السيد رمضانNo ratings yet
- Discharge PlanDocument5 pagesDischarge PlanrraksNo ratings yet
- PrednisoloneDocument4 pagesPrednisoloneUmemura-san SOkmo100% (1)
- CholelithiasisDocument6 pagesCholelithiasismarkzamNo ratings yet
- NCPDocument13 pagesNCPÍam KristineNo ratings yet
- Drug StudyDocument5 pagesDrug StudyRai D. MacapantonNo ratings yet
- Doxophylline Prescribing InformationDocument1 pageDoxophylline Prescribing InformationMohammed shamiul ShahidNo ratings yet
- Omacor: Municipal Planning and Development OfficeDocument9 pagesOmacor: Municipal Planning and Development OfficeArthur MericoNo ratings yet
- DexamethasoneDocument4 pagesDexamethasoneCatherine Anne Khan ClementeNo ratings yet
- Salbuterol Generic NameDocument4 pagesSalbuterol Generic NamejunieNo ratings yet
- Ketessee FCT Dexketoprofen Jul 2012Document8 pagesKetessee FCT Dexketoprofen Jul 2012Dhurai OnelyNo ratings yet
- Drug Study: West Visayas State UniversityDocument2 pagesDrug Study: West Visayas State Universityw dNo ratings yet
- Cefpodoxime Proxetil - Print VersionDocument5 pagesCefpodoxime Proxetil - Print Versionchristina_1990No ratings yet
- ARCOXIADocument22 pagesARCOXIATeresa JunioNo ratings yet
- Drug Study - CaseDocument9 pagesDrug Study - CaseMay EvelynNo ratings yet
- AnsimarDocument2 pagesAnsimarcop_perNo ratings yet
- CHA NCPDocument6 pagesCHA NCPMonty_Legaspi_5664No ratings yet
- HernioplastyDocument6 pagesHernioplastyCherry Delos ReyesNo ratings yet
- Nursong ResponsibilitiesDocument4 pagesNursong ResponsibilitiesMichaela JapsayNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- The politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840From EverandThe politics of hunger: Protest, poverty and policy in England, <i>c.</i> 1750–<i>c.</i> 1840No ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Fruit Jam & Jelly - Preparation1Document2 pagesFruit Jam & Jelly - Preparation1Iboyaima singhNo ratings yet
- Chapter 5 Regression AnalysisDocument14 pagesChapter 5 Regression AnalysisLeslie Anne BiteNo ratings yet
- Optimization For ML (2) : CS771: Introduction To Machine Learning Piyush RaiDocument14 pagesOptimization For ML (2) : CS771: Introduction To Machine Learning Piyush RaiRajaNo ratings yet
- Asset Masterlist - NBEHPPDocument248 pagesAsset Masterlist - NBEHPPSamsudin Ahmad100% (1)
- Plet TB 1a MTDocument12 pagesPlet TB 1a MTohmygod622No ratings yet
- Lake Macquarie Crime Prevention Strategy 2021 2024Document24 pagesLake Macquarie Crime Prevention Strategy 2021 2024DorjeNo ratings yet
- Chapter 5 Equilibrium Part 2Document29 pagesChapter 5 Equilibrium Part 2danicagregorio052003No ratings yet
- Predicate Logic 18. Free and Bound Variables: The LectureDocument21 pagesPredicate Logic 18. Free and Bound Variables: The LectureNidhi DivechavaluNo ratings yet
- Childcare Question-ABC NanniesDocument3 pagesChildcare Question-ABC NanniesLuther AnyaipomaNo ratings yet
- Chapter 1 - Computers and The Health ProfessionalsDocument53 pagesChapter 1 - Computers and The Health ProfessionalsIreneo BesingaNo ratings yet
- The Death of Grace Miller (Draft 1)Document104 pagesThe Death of Grace Miller (Draft 1)Allen AvilaNo ratings yet
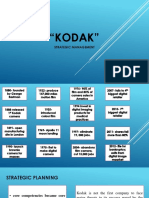
- "Kodak": Strategic ManagementDocument9 pages"Kodak": Strategic ManagementKyohyunNo ratings yet
- "Recruitment Process in Halonix Limited" Sumitted To: Summer Traiing Report OnDocument7 pages"Recruitment Process in Halonix Limited" Sumitted To: Summer Traiing Report Onankurk124No ratings yet
- Biochem 2Document1 pageBiochem 2กรวรินทร์ ชำนาญกุลNo ratings yet
- Orientation: Grade 7-Drama Unit 1Document14 pagesOrientation: Grade 7-Drama Unit 1api-377114739100% (1)
- CPU Business and Information Technology CollegeDocument40 pagesCPU Business and Information Technology CollegeDejeneNo ratings yet
- Recapitulation Sheet Class IV 06.04.21Document4 pagesRecapitulation Sheet Class IV 06.04.21Anishka GuptaNo ratings yet
- Vấn đápDocument41 pagesVấn đápKhắc Trung NguyễnNo ratings yet
- Using Dali in HwqsDocument18 pagesUsing Dali in HwqsRadhi HirziNo ratings yet
- Introduction To ArchaebacteriaDocument12 pagesIntroduction To Archaebacteriakanchan sharmaNo ratings yet
- Term Paper Format TagalogDocument7 pagesTerm Paper Format Tagalogafdtrajxq100% (1)
- Allergic PDFDocument17 pagesAllergic PDFSiska HarapanNo ratings yet
- Sin 2 1 Cos 2: Graphing Sine and Cosine Worksheet #1 Fill in The Blanks and GraphDocument4 pagesSin 2 1 Cos 2: Graphing Sine and Cosine Worksheet #1 Fill in The Blanks and GraphAPCommentatorNo ratings yet
- DBMS Notes For BCADocument9 pagesDBMS Notes For BCAarndm8967% (6)
- Sprint - Volte Kpi'sDocument3 pagesSprint - Volte Kpi'sSreeNo ratings yet
- GRADE 5 Science DLL Whole Year Grade 5Document161 pagesGRADE 5 Science DLL Whole Year Grade 5Angelica DionisioNo ratings yet
- HTD PulleysDocument30 pagesHTD Pulleysspeed844100% (1)
- Dental Assisting: A Comprehensive Approach. 5th Edition. ISBN 1305967631, 978-1305967632Document23 pagesDental Assisting: A Comprehensive Approach. 5th Edition. ISBN 1305967631, 978-1305967632gertrudnazlerv100% (19)