Open Access Atlas of Otolaryngology, Head & Neck Operative Surgery
Open Access Atlas of Otolaryngology, Head & Neck Operative Surgery
Download as pdf or txt
You might also like
- The Dangers of Sitting - Why Sitting Is The New Smoking - Better Health ChannelDocument10 pagesThe Dangers of Sitting - Why Sitting Is The New Smoking - Better Health ChannelMOHAMED CHERIFINo ratings yet
- Robbins Pathology Chapter 14 - RBCsDocument7 pagesRobbins Pathology Chapter 14 - RBCsscorpiosphinx79100% (10)
- Open Complex Abdominal Wall ReconstructionDocument16 pagesOpen Complex Abdominal Wall ReconstructionpipeudeaNo ratings yet
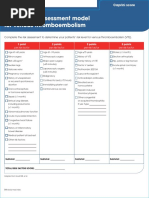
- VTE Risk Assessment Tool Caprini Score Card Eng 30apr2018Document2 pagesVTE Risk Assessment Tool Caprini Score Card Eng 30apr2018Ahmed MohammedNo ratings yet
- 56169572-Selected-Readings-in-Plastic-Surgery TextDocument132 pages56169572-Selected-Readings-in-Plastic-Surgery TextyellowbieNo ratings yet
- BY DR Jahangir Hammad BDS, FcpsDocument110 pagesBY DR Jahangir Hammad BDS, FcpsAtika Iftikhar MirNo ratings yet
- Purpura Retiforme EnfrentamientoDocument14 pagesPurpura Retiforme EnfrentamientoalejandroNo ratings yet
- Gluteal Artery Perforator FlapsDocument8 pagesGluteal Artery Perforator FlapsJose Mauricio Suarez BecerraNo ratings yet
- Key StoneDocument59 pagesKey StoneJannat JeebaNo ratings yet
- Use of Retroauricular Temporal Flap For Large Post Oncosurgical Glabellar and Forehead DefectsDocument4 pagesUse of Retroauricular Temporal Flap For Large Post Oncosurgical Glabellar and Forehead DefectsPalwasha Malik100% (1)
- Nasolabial Flap For Oral Cavity ReconstructionDocument10 pagesNasolabial Flap For Oral Cavity ReconstructionJamesNo ratings yet
- Submental Artery Island Flap Technique For Head Neck ReconstructionDocument18 pagesSubmental Artery Island Flap Technique For Head Neck ReconstructionMahir NuredinNo ratings yet
- Auric Recon Slides 070516Document92 pagesAuric Recon Slides 070516Yudhistira AdeNo ratings yet
- Neligan Vol 4 Chapter 10 MainDocument20 pagesNeligan Vol 4 Chapter 10 MainisabelNo ratings yet
- Clinical Atlas of Preservation Rhinoplasty Steps For Surgeons in Training 9783031299766 9783031299773 Compress 1Document215 pagesClinical Atlas of Preservation Rhinoplasty Steps For Surgeons in Training 9783031299766 9783031299773 Compress 1nilfacioNo ratings yet
- Lower Third Leg Defects: Anurag Pandey Moderator: DR Deepak NandaDocument59 pagesLower Third Leg Defects: Anurag Pandey Moderator: DR Deepak Nandaanu_ragNo ratings yet
- Oral LymphangiomaDocument8 pagesOral LymphangiomasevattapillaiNo ratings yet
- Submental Flap in Head and Neck Reconstruction An Alternative To Microsurgical Flap - February - 2020 - 1580559115 - 2824301Document3 pagesSubmental Flap in Head and Neck Reconstruction An Alternative To Microsurgical Flap - February - 2020 - 1580559115 - 2824301Karan HarshavardhanNo ratings yet
- Scalp Reconstruction An Algorithmic Approach and Systematic ReviewDocument11 pagesScalp Reconstruction An Algorithmic Approach and Systematic Reviewahmed atefNo ratings yet
- Cleft Rhinoplasty CMEDocument13 pagesCleft Rhinoplasty CMENaveed KhanNo ratings yet
- A Classification System of DefectsDocument12 pagesA Classification System of DefectsPrana SkyaNo ratings yet
- Regional Flaps in Head and Neck ReconstructionDocument11 pagesRegional Flaps in Head and Neck ReconstructionBenedetta GuarinoNo ratings yet
- Lasers in Plastic Surgery - Srps. 2018 11 (10C) 1-53Document53 pagesLasers in Plastic Surgery - Srps. 2018 11 (10C) 1-5376j9qvh29rNo ratings yet
- Modified & Radical Neck Dissection: Johan FaganDocument18 pagesModified & Radical Neck Dissection: Johan FaganGeorgetaGeorgyNo ratings yet
- Local Skin Flaps: Kevin Katzenmeyer, MD Karen Calhoun, MD June 21, 2000Document71 pagesLocal Skin Flaps: Kevin Katzenmeyer, MD Karen Calhoun, MD June 21, 2000IqbalurNo ratings yet
- Classification of FlapsDocument10 pagesClassification of FlapsDavid Sidhom100% (1)
- Manual of Head and Neck ReconstructionDocument429 pagesManual of Head and Neck ReconstructionTanushka KukrejaNo ratings yet
- Mohs Micrographic Surgery From Layers To Reconstruction - Christopher B HarmonDocument272 pagesMohs Micrographic Surgery From Layers To Reconstruction - Christopher B HarmonLuis Ortiz AtienzaNo ratings yet
- Ijcmr 1538 3Document8 pagesIjcmr 1538 3drelvNo ratings yet
- Management of Segmental Bone DefectDocument11 pagesManagement of Segmental Bone DefectZin HtutNo ratings yet
- Masseter Muscle Reattachment After Mandibular Angle SurgeryDocument4 pagesMasseter Muscle Reattachment After Mandibular Angle Surgery洪侊增No ratings yet
- Complicated Facial WoundsDocument5 pagesComplicated Facial WoundsIJAR JOURNALNo ratings yet
- The Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic ReconstrDocument8 pagesThe Scip Propeller Flap Versatility For R - 2019 - Journal of Plastic Reconstrydk sinhNo ratings yet
- SAB HandbookDocument81 pagesSAB HandbookDalibor CetojevicNo ratings yet
- Cosmetic Surgery Today 1e WWW Bookbaz IrDocument222 pagesCosmetic Surgery Today 1e WWW Bookbaz Irazadparis66No ratings yet
- Tamai Zone 1 Fingertip Amputation: Reconstruction Using A Digital Artery Flap Compared With Microsurgical ReplantationDocument7 pagesTamai Zone 1 Fingertip Amputation: Reconstruction Using A Digital Artery Flap Compared With Microsurgical ReplantationFeliciaDewiNo ratings yet
- Basic Principles in Surgical Oncology - Cady1997 Arch Surg PDFDocument9 pagesBasic Principles in Surgical Oncology - Cady1997 Arch Surg PDFDiego EskinaziNo ratings yet
- Flap Basics I Rotation and Transposition FlapsDocument9 pagesFlap Basics I Rotation and Transposition FlapsariskaNo ratings yet
- Zygomatico-Maxillary Complex Fractures: A Retrospective Study On Etiology, Pattern and ManagementDocument12 pagesZygomatico-Maxillary Complex Fractures: A Retrospective Study On Etiology, Pattern and ManagementSweet SumanNo ratings yet
- Chest Wall ReconstrDocument20 pagesChest Wall ReconstrLuis A De la CubaNo ratings yet
- The Transverse Rectus Abdominus Myocutaneous (Tram) FlapDocument25 pagesThe Transverse Rectus Abdominus Myocutaneous (Tram) FlapyahyaNo ratings yet
- Harvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsDocument7 pagesHarvesting Rib Cartilage Grafts For Secondary Rhinoplasty: Background: MethodsLuiggi Fayad100% (1)
- Kaban 2009 TMJ ANKYLOSISDocument13 pagesKaban 2009 TMJ ANKYLOSISPorcupine TreeNo ratings yet
- s13023 015 0302 1 PDFDocument14 pagess13023 015 0302 1 PDFNur Alfia KusumaningsihNo ratings yet
- 2022+vitaly+ +Skin+Contour+Sutures+in+RhinoplastyDocument11 pages2022+vitaly+ +Skin+Contour+Sutures+in+RhinoplastyJackeline Lizbeth Anicama mendozaNo ratings yet
- Salivary Gland Neoplasm: Dr. Saad Al-Muhayawi. M.D., FRCSC Associate Professor & Consultant ORL Head & Neck SurgeryDocument43 pagesSalivary Gland Neoplasm: Dr. Saad Al-Muhayawi. M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgeryraishern5475No ratings yet
- Recent Advances in The Treatment of FracturesDocument29 pagesRecent Advances in The Treatment of Fracturesmanjunatha100% (1)
- Reconstrucción Defectos Nasales PDFDocument18 pagesReconstrucción Defectos Nasales PDFSara OmNo ratings yet
- Finger Amputations: Aviram M. Giladi and Kevin C. ChungDocument12 pagesFinger Amputations: Aviram M. Giladi and Kevin C. ChungREM biusNo ratings yet
- Tongue ResectionDocument13 pagesTongue Resectioncr89omfNo ratings yet
- Retromandibular ApproachesDocument8 pagesRetromandibular ApproachesfsjNo ratings yet
- PeritonectomiesDocument13 pagesPeritonectomiessrinivasfruNo ratings yet
- ACS Parotidectomy PDFDocument10 pagesACS Parotidectomy PDFadel santosNo ratings yet
- Instant Download Oxford Textbook of Plastic and Reconstructive Surgery 1st Edition Simon Kay PDF All ChapterDocument60 pagesInstant Download Oxford Textbook of Plastic and Reconstructive Surgery 1st Edition Simon Kay PDF All Chapterleatourojbi100% (3)
- Ranula and Sublingual Salivary Gland Excision PDFDocument5 pagesRanula and Sublingual Salivary Gland Excision PDFsusanti bulanNo ratings yet
- Trauma ZygomaDocument9 pagesTrauma ZygomarezaaamuhammadNo ratings yet
- Orthognathic Surgery For MandibleDocument36 pagesOrthognathic Surgery For MandibleHartomo BenxNo ratings yet
- Reconstructive Surgery - Lower Extremity CoverageDocument29 pagesReconstructive Surgery - Lower Extremity Coverage정형화No ratings yet
- RtyvhDocument14 pagesRtyvhBibek RajNo ratings yet
- Role of Corticosteroids in Functional Endoscopic Sinus Surgery A Systematic Review and Meta Analysis AcceptedDocument39 pagesRole of Corticosteroids in Functional Endoscopic Sinus Surgery A Systematic Review and Meta Analysis AcceptedTIkaNo ratings yet
- Lip ReconstructionDocument42 pagesLip ReconstructionReema ChawlaNo ratings yet
- GraftsDocument23 pagesGraftsLinngamuNo ratings yet
- Full Download Facial Trauma Surgery: From Primary Repair To Reconstruction 1st Edition Amir Dorafshar PDFDocument58 pagesFull Download Facial Trauma Surgery: From Primary Repair To Reconstruction 1st Edition Amir Dorafshar PDFninetusaid100% (4)
- 2022 CFE H Human Biology Paper 2 AnswersDocument21 pages2022 CFE H Human Biology Paper 2 AnswersDhrgrb SvdhNo ratings yet
- Non-Hepatic Hyperammonaemia: An Important, Potentially Reversible Cause of EncephalopathyDocument7 pagesNon-Hepatic Hyperammonaemia: An Important, Potentially Reversible Cause of EncephalopathyJoemon K JoyNo ratings yet
- Warfarin Reversal Guideline 2012 PDFDocument8 pagesWarfarin Reversal Guideline 2012 PDFVlady78No ratings yet
- Case Study CvaDocument6 pagesCase Study Cvajing_elizabethNo ratings yet
- 3 s2.0 B9780323530422002364 PDFDocument6 pages3 s2.0 B9780323530422002364 PDFMichaella AlmirahNo ratings yet
- Inflammatory Valvular and Vascular Disease STUDENT FA24Document47 pagesInflammatory Valvular and Vascular Disease STUDENT FA24jdounethkaNo ratings yet
- GS 201-250Document19 pagesGS 201-250Sara Abdul RahmanNo ratings yet
- Anemia PDFDocument36 pagesAnemia PDFJANo ratings yet
- MK Thrombotic Disorders PDFDocument10 pagesMK Thrombotic Disorders PDFMoses Jr KazevuNo ratings yet
- Ethinylestradiol 0.02mg + Gestodene 0.075mg (Meliane)Document18 pagesEthinylestradiol 0.02mg + Gestodene 0.075mg (Meliane)asdwasdNo ratings yet
- Case Study Cva Gr1Document72 pagesCase Study Cva Gr1Divina Gracia Fabicon Arana100% (1)
- Frizzell 2005Document20 pagesFrizzell 2005GiorgianaNo ratings yet
- Acog Committee Opinion: Uterine Morcellation For Presumed LeiomyomasDocument12 pagesAcog Committee Opinion: Uterine Morcellation For Presumed LeiomyomasYo MeNo ratings yet
- 11 Anti-Coagulants & FibrinolyticsDocument52 pages11 Anti-Coagulants & FibrinolyticsUmmuShefaNo ratings yet
- Pathophysiology of Acute Ischemic Stroke: Continuum Lifelong Learning Neurol 2008 14 (6) :28-45Document18 pagesPathophysiology of Acute Ischemic Stroke: Continuum Lifelong Learning Neurol 2008 14 (6) :28-45Hector SaavedraNo ratings yet
- Vet PathologyDocument128 pagesVet PathologyMegarsaNo ratings yet
- Pathophysiology of StrokeDocument9 pagesPathophysiology of StrokeAnj MandeoyaNo ratings yet
- 2014surgery2 (6 Files Merged)Document221 pages2014surgery2 (6 Files Merged)Hannan SyedNo ratings yet
- Iritis 6Document6 pagesIritis 6Alvis KurniawanNo ratings yet
- Florin Bzovii Abstract enDocument38 pagesFlorin Bzovii Abstract enVasile Pogor ISNo ratings yet
- 2 - Pulmonary HypertensionDocument9 pages2 - Pulmonary Hypertensionpuskommedic 003No ratings yet
- 863 How To Prevent Heart Attacks BEN SANDLER MD 1958Document63 pages863 How To Prevent Heart Attacks BEN SANDLER MD 1958Konstantin SurkovNo ratings yet
- Preoperative Pain Management Education An Evidence-Based Practice ProjectDocument8 pagesPreoperative Pain Management Education An Evidence-Based Practice Projectfachrudin arNo ratings yet
- Rodaks Hema 2 Lec Chapter 39&40Document45 pagesRodaks Hema 2 Lec Chapter 39&40Ivory Mae Verona AndayaNo ratings yet
- Perioperative CareDocument18 pagesPerioperative CareCo Pablico EricNo ratings yet
- Product InformationDocument6 pagesProduct Informationciaocat2018No ratings yet