Caso Clinico Clinica Mayo 2
Caso Clinico Clinica Mayo 2
Download as pdf or txt
You might also like
- PEER IX-Physician Evaluation and Educational Review in Emergency Medicine PDFDocument627 pagesPEER IX-Physician Evaluation and Educational Review in Emergency Medicine PDFAbdullah Ali Baksh100% (7)
- PANCE Prep Pearls Cardio Questions PDFDocument9 pagesPANCE Prep Pearls Cardio Questions PDFkat100% (3)
- Heartbeat SensorDocument13 pagesHeartbeat Sensorkrishna mohan pandeyNo ratings yet
- Blood Pressure Sensor User Guide and Arduino Code PDFDocument13 pagesBlood Pressure Sensor User Guide and Arduino Code PDFhyhyhyhyhy50% (2)
- ST Elevation Not Only AcsDocument3 pagesST Elevation Not Only AcsRika MeliauwatiNo ratings yet
- Does This Dyspneic Patient in The Emergency Department Have Congestive Heart Failure?Document13 pagesDoes This Dyspneic Patient in The Emergency Department Have Congestive Heart Failure?Jorge MéndezNo ratings yet
- Dor No Peito em Paciente Com CoronariopatiaDocument7 pagesDor No Peito em Paciente Com CoronariopatiacaioaccorsiNo ratings yet
- Survival of A Neurologically Intact Patient With Subarachnoid Hemorrhage and Cardiopulmonary ArrestDocument4 pagesSurvival of A Neurologically Intact Patient With Subarachnoid Hemorrhage and Cardiopulmonary ArrestDino RatnamNo ratings yet
- Massive Pulmonary Embolism Presenting As Seizures: December 2008 Vol 10 No 4Document4 pagesMassive Pulmonary Embolism Presenting As Seizures: December 2008 Vol 10 No 4BelladonnaRoxNo ratings yet
- Casoclincio de TepDocument3 pagesCasoclincio de TepArturo Vargas AguilarNo ratings yet
- Nejmcps 2116690Document8 pagesNejmcps 2116690Luis MadrigalNo ratings yet
- Is It Always Anterior Chest Pain Angina Pectoris?Document7 pagesIs It Always Anterior Chest Pain Angina Pectoris?Diana MinzatNo ratings yet
- 61a Woman LES N Chest PainDocument6 pages61a Woman LES N Chest PainGabriel MouraNo ratings yet
- Criem2015 868519Document4 pagesCriem2015 868519m.fahimsharifiNo ratings yet
- 03ma NonDocument3 pages03ma NonsreeeeeNo ratings yet
- (Mayo Clinic Proceedings, Dec 2022) - 82 Year Old Man With Chest Pain and Shortness of BreathDocument5 pages(Mayo Clinic Proceedings, Dec 2022) - 82 Year Old Man With Chest Pain and Shortness of BreathNigelyulNo ratings yet
- Recurrent Unilateral Pleural Effusion From Constrictive Pericarditis of Unknown Etiology Requiring PericardiectomyDocument3 pagesRecurrent Unilateral Pleural Effusion From Constrictive Pericarditis of Unknown Etiology Requiring PericardiectomyJaya Semara PutraNo ratings yet
- Tuberculous Pericarditis Leading To Cardiac Tamponade Importance of Screening Prior To ImmunosuppressionDocument3 pagesTuberculous Pericarditis Leading To Cardiac Tamponade Importance of Screening Prior To ImmunosuppressionLink BuiNo ratings yet
- Troponin Assays: More Questions Than Answers?: Doi: 10.1111/j.1742-6723.2009.01225.xDocument2 pagesTroponin Assays: More Questions Than Answers?: Doi: 10.1111/j.1742-6723.2009.01225.xprashsubbuNo ratings yet
- Pulmonary Thromboembolism MCQ PDFDocument8 pagesPulmonary Thromboembolism MCQ PDFPradeep Gupt100% (2)
- Case I IIDocument9 pagesCase I IIDINDA PUTRI SAVIRANo ratings yet
- Cric2018 7237454Document4 pagesCric2018 7237454Muhammad Nur Ardhi LahabuNo ratings yet
- Banchi Final VTEDocument93 pagesBanchi Final VTEBanchiamlak AbieNo ratings yet
- 1153-Article Text-4888-1-10-20200206 PDFDocument6 pages1153-Article Text-4888-1-10-20200206 PDFAdrian CaballesNo ratings yet
- Criem2020 4159526Document5 pagesCriem2020 4159526m.fahimsharifiNo ratings yet
- Acute Pericarditis: Clinical PracticeDocument8 pagesAcute Pericarditis: Clinical PracticeGaby Alejandra Ordonez AndradeNo ratings yet
- Electrocardiographic Changes and Intracranial Pathology: Geraldine Syverud, Crna, BSNDocument4 pagesElectrocardiographic Changes and Intracranial Pathology: Geraldine Syverud, Crna, BSNchuck55No ratings yet
- Dengue Myocarditis: Case ReportDocument3 pagesDengue Myocarditis: Case Reportallfanz_krenNo ratings yet
- Ecocardiografia Monitoreo Hemodinamico en Critico..Document12 pagesEcocardiografia Monitoreo Hemodinamico en Critico..cositaamorNo ratings yet
- Omur - Tc-99m MIBI Myocard Perfusion SPECT Findings in Patients With Typical Chest Pain and Normal Coronary ArteriesDocument8 pagesOmur - Tc-99m MIBI Myocard Perfusion SPECT Findings in Patients With Typical Chest Pain and Normal Coronary ArteriesM. PurnomoNo ratings yet
- PDF File 22Document1 pagePDF File 22KpavanSaireddyNo ratings yet
- Regurgitação AorticaDocument8 pagesRegurgitação AorticaBiancaNo ratings yet
- Case Wecoc FinalDocument4 pagesCase Wecoc Finalfatmaasri112No ratings yet
- Case Reports AbstractsDocument7 pagesCase Reports AbstractsNovie AstiniNo ratings yet
- Oncologic Mechanical Emergencies 2014 Emergency Medicine Clinics of North AmericaDocument14 pagesOncologic Mechanical Emergencies 2014 Emergency Medicine Clinics of North AmericamarcosjuniormutucaNo ratings yet
- 2018 Article 1648Document5 pages2018 Article 1648Dewi NurfadilahNo ratings yet
- Idiopathic Pre-Capillary Pulmonary Hypertension in Patients With End-Stage Kidney Disease - Effect of Endothelin Receptor AntagonistsDocument9 pagesIdiopathic Pre-Capillary Pulmonary Hypertension in Patients With End-Stage Kidney Disease - Effect of Endothelin Receptor AntagonistsyuliaNo ratings yet
- Summer 2021 FinalDocument16 pagesSummer 2021 FinalJuan Carlos LopezNo ratings yet
- 67-Article Text-115-1-10-20171026Document5 pages67-Article Text-115-1-10-20171026Maria MiripNo ratings yet
- Broken: Diagnosis and ReasoningDocument3 pagesBroken: Diagnosis and ReasoningSYED SHAZIYANo ratings yet
- Transesophageal Echocardiography: The Hemodynamic Monitoring UtilizingDocument14 pagesTransesophageal Echocardiography: The Hemodynamic Monitoring UtilizingvegasbabyNo ratings yet
- Recurrent Takotsubo CardiomyopathyDocument6 pagesRecurrent Takotsubo CardiomyopathyProdi S1- 1BNo ratings yet
- 1Document4 pages1Mirla Castellanos JuradoNo ratings yet
- Assignment: Applied MedicineDocument13 pagesAssignment: Applied MedicineKhadija BakhtawarNo ratings yet
- JURNALDocument7 pagesJURNALHarlina NurlitaNo ratings yet
- Topic 10 Internal Medicine Ali SaifDocument5 pagesTopic 10 Internal Medicine Ali SaifAnkit Kumar PatelNo ratings yet
- Badertscher Et Al 2019 Prevalence of Pulmonary Embolism in Patients With SyncopeDocument11 pagesBadertscher Et Al 2019 Prevalence of Pulmonary Embolism in Patients With SyncopeNJEBARIKANUYE EugèneNo ratings yet
- Case Report Cteph EditDocument13 pagesCase Report Cteph EditapekzzzzNo ratings yet
- 1 s2.0 S0735675715005483 MainDocument3 pages1 s2.0 S0735675715005483 Mainfebriandika gawlNo ratings yet
- A Case of Complete Heart Block With Diagnostic Challenge and Therapeutic DilemmaDocument4 pagesA Case of Complete Heart Block With Diagnostic Challenge and Therapeutic DilemmaXo YemNo ratings yet
- BCR 2012 007205Document4 pagesBCR 2012 007205shofidhiaaaNo ratings yet
- A Detail of The Molecular AnatomyDocument5 pagesA Detail of The Molecular AnatomyMihaela Simona IsacNo ratings yet
- Chest 06-1281Document4 pagesChest 06-1281egagusmelaNo ratings yet
- Resident Chest Pain ModuleDocument7 pagesResident Chest Pain ModuleFatima ShoukatNo ratings yet
- 210 Acute Coronary SyndromeDocument7 pages210 Acute Coronary SyndromeMuhammad Umer SaeedNo ratings yet
- 2017 17 4 148 150 EngDocument3 pages2017 17 4 148 150 Engخالد العيلNo ratings yet
- Harmony in Flutter: A Comprehensive Exploration of Atrial Flutter - From Molecular Insights to Holistic HealthFrom EverandHarmony in Flutter: A Comprehensive Exploration of Atrial Flutter - From Molecular Insights to Holistic HealthNo ratings yet
- Coronary Vasomotion AbnormalitiesFrom EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaNo ratings yet
- Acute Cholecystitis Positive HIDA Scan - UpToDateDocument1 pageAcute Cholecystitis Positive HIDA Scan - UpToDateFrancisco HernandezNo ratings yet
- Ca de PeneDocument1 pageCa de PeneFrancisco HernandezNo ratings yet
- Caso Clinico Clnica Mayo 3Document6 pagesCaso Clinico Clnica Mayo 3Francisco HernandezNo ratings yet
- The Diagnosis and Treatment of Antisynthetase SyndromeDocument9 pagesThe Diagnosis and Treatment of Antisynthetase SyndromeFrancisco HernandezNo ratings yet
- ECG Mastery Yellow Belt CookbookDocument2 pagesECG Mastery Yellow Belt Cookbooktenny21092000No ratings yet
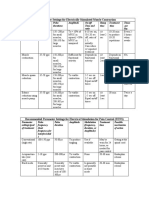
- Parameter Settings For Electrically Stimulated Muscle ContractionDocument3 pagesParameter Settings For Electrically Stimulated Muscle Contractionpallen100% (5)
- Cardiovascular DisordersDocument4 pagesCardiovascular DisordersJA BerzabalNo ratings yet
- Domain 4Document49 pagesDomain 4Ayu KrisNo ratings yet
- A Multiparameter Algorithm To Guide Repair of Degenerative Mitral RegurgitationDocument47 pagesA Multiparameter Algorithm To Guide Repair of Degenerative Mitral RegurgitationWilson BotelhoNo ratings yet
- Heart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesDocument10 pagesHeart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesAndhika DNo ratings yet
- Hemodinamik Dasar Invasive 2Document27 pagesHemodinamik Dasar Invasive 2Tkv UhamkaNo ratings yet
- L A Level Biology MS Jun 05Document180 pagesL A Level Biology MS Jun 05Shireen KaurooNo ratings yet
- Circulatory System (The Heart) 2Document20 pagesCirculatory System (The Heart) 2anuNo ratings yet
- As GCE Biology 2802 January 2007 Question PaperDocument12 pagesAs GCE Biology 2802 January 2007 Question PaperVeer RamloghunNo ratings yet
- 9-Medicine Allied SubjectsDocument75 pages9-Medicine Allied SubjectsAbdul QuaiyumNo ratings yet
- Common Emergency DrugsDocument1 pageCommon Emergency DrugsFreeNursingNotesNo ratings yet
- ASCITESDocument2 pagesASCITESCollen TinarwoNo ratings yet
- Theoretical Competition: - SolutionDocument12 pagesTheoretical Competition: - SolutionnazimNo ratings yet
- LFSC Grade 10 Step Ahead Learner Support Document 2023Document46 pagesLFSC Grade 10 Step Ahead Learner Support Document 2023AlanaDariesNo ratings yet
- Non Obstructive Versus Obstructive Coronary ArteryDocument7 pagesNon Obstructive Versus Obstructive Coronary ArteryAndreea LeonteNo ratings yet
- AS Biology Unit 2 NotesDocument34 pagesAS Biology Unit 2 NotesMehreenSaeedNo ratings yet
- Dtra For Ppci MD and Ac Jacc 2022Document2 pagesDtra For Ppci MD and Ac Jacc 2022marcos.danilloNo ratings yet
- Amprahan Bedah Jantung 1Document6 pagesAmprahan Bedah Jantung 1hybridNo ratings yet
- Medical+language+practice+ NotesDocument7 pagesMedical+language+practice+ NotesmanethNo ratings yet
- The ABCDE Assessment: Airway (A)Document10 pagesThe ABCDE Assessment: Airway (A)Kianne Rae Fernandez PalmaNo ratings yet
- CV DR IhabDocument4 pagesCV DR IhabIhab SulimanNo ratings yet
- Anatomy of Cardio Vascular System NotesDocument16 pagesAnatomy of Cardio Vascular System NotesAgleema AhmedNo ratings yet
- Mapeh 7 4TH TQDocument2 pagesMapeh 7 4TH TQJunrel SapantaNo ratings yet
- Homoeopathic Materia Medica PDFDocument595 pagesHomoeopathic Materia Medica PDFAdnan Rahat67% (3)
- CardiologyDocument4 pagesCardiologyPATEL NEHAKUMARI VIMALBHAINo ratings yet
- ABC of Clinical Electrocardiography Myocardial IschaemiaDocument6 pagesABC of Clinical Electrocardiography Myocardial IschaemiaShri Mahalaxmi HarishNo ratings yet
- Q2 Science Wk1 Lesson 1Document9 pagesQ2 Science Wk1 Lesson 1Kathleen ManglaasNo ratings yet