Repetitve Nerve Stimulation (RNS) : By: Syed Irshad Murtaza Neurophysiology Dept AKUH Karachi Date:12-06-2013
Repetitve Nerve Stimulation (RNS) : By: Syed Irshad Murtaza Neurophysiology Dept AKUH Karachi Date:12-06-2013
Download as pdf or txt
You might also like
- 29.1.11 Lecture 7. Synapses, Properties & TransmissionDocument37 pages29.1.11 Lecture 7. Synapses, Properties & TransmissionAttiqaQureshiNo ratings yet
- Key of SEQs Heart, Nerve and Muscle Revision TestDocument11 pagesKey of SEQs Heart, Nerve and Muscle Revision TestMudassar Roomi100% (2)
- L2 Neurons and Neuronal NetworksDocument4 pagesL2 Neurons and Neuronal NetworksmoshlingmomoNo ratings yet
- Nerve Conduction Velocity: Karunakaran K MPT (Neuro) ., PGDMT Associate Professor, SvcoptDocument30 pagesNerve Conduction Velocity: Karunakaran K MPT (Neuro) ., PGDMT Associate Professor, SvcoptSineka 19170239No ratings yet
- NERVE & MUSCLE 45 Qs With Their Answer Keys by Dr. RoomiDocument54 pagesNERVE & MUSCLE 45 Qs With Their Answer Keys by Dr. RoomiMudassar Roomi100% (1)
- Synaptic Depression: Many Different Possible MechanismsDocument24 pagesSynaptic Depression: Many Different Possible MechanismsThe Panda EntertainerNo ratings yet
- A Review of Neuromuscular MonitoringDocument10 pagesA Review of Neuromuscular Monitoringdrcds99No ratings yet
- Estudios de Conduccion NerviosaDocument8 pagesEstudios de Conduccion NerviosaSoledad CáceresNo ratings yet
- 1Document4 pages1डा. सत्यदेव त्यागी आर्यNo ratings yet
- 5 - EMG+Nerve Conduction StudyDocument46 pages5 - EMG+Nerve Conduction Studyaishp2897No ratings yet
- Overview of Nerve Conduction StudiesDocument21 pagesOverview of Nerve Conduction Studiesชานนทร์ มรกตวิจิตรการNo ratings yet
- Myasthenia Gravis - PathophysiologyDocument3 pagesMyasthenia Gravis - PathophysiologyDill BadaróNo ratings yet
- Basics of Electrodiagnostic StudiesDocument39 pagesBasics of Electrodiagnostic StudiessisasuNo ratings yet
- Synaptic TransmissionDocument17 pagesSynaptic TransmissionbnmjgcNo ratings yet
- Basic NCS CourseDocument47 pagesBasic NCS Coursefaithless.kzNo ratings yet
- NCV PDFDocument99 pagesNCV PDFSukhman ChawlaNo ratings yet
- NCS FINALDocument48 pagesNCS FINALelsayed.aymanNo ratings yet
- .trashed-1688035334-RPSGT EXAM LATEST 2023Document18 pages.trashed-1688035334-RPSGT EXAM LATEST 2023elias njagiNo ratings yet
- 6 Evoked PotentialsDocument36 pages6 Evoked PotentialsRafael MenesesNo ratings yet
- Synaptic Transmission 4Document36 pagesSynaptic Transmission 4stehephNo ratings yet
- Tercer Resumen de Biomedica 2Document8 pagesTercer Resumen de Biomedica 2Dulce SaucedaNo ratings yet
- Evoked PotentialsDocument49 pagesEvoked PotentialsparuNo ratings yet
- Lecture On The Physiology of Neuromuscular Junction (NMJ) by Dr. RoomiDocument18 pagesLecture On The Physiology of Neuromuscular Junction (NMJ) by Dr. RoomiMudassar Roomi100% (3)
- Brain Res 1977 AghajanianDocument8 pagesBrain Res 1977 Aghajanianndyfk54dpgNo ratings yet
- Neuromuscular Junction by Dr. RoomiDocument20 pagesNeuromuscular Junction by Dr. RoomiMudassar Roomi100% (1)
- Sistem Saraf Pusat (Central Nervous System)Document23 pagesSistem Saraf Pusat (Central Nervous System)Ruspata BhyantariNo ratings yet
- Electrotonic Conduction, Myelin, and Multiple SclerosisDocument1 pageElectrotonic Conduction, Myelin, and Multiple Sclerosis6qhx62pr42No ratings yet
- Synaptic IntegrationDocument5 pagesSynaptic Integrationryan100% (1)
- 5-Nerve Conduction Studies and EMGDocument16 pages5-Nerve Conduction Studies and EMGMustafa2392003aNo ratings yet
- Synapses and Synaptic Transmission: Dr. Eman El Eter Physiology Dep. College of Medicine KSUDocument43 pagesSynapses and Synaptic Transmission: Dr. Eman El Eter Physiology Dep. College of Medicine KSUraanja2No ratings yet
- Electrodiagnostic ProceduresDocument3 pagesElectrodiagnostic Proceduresakheel ahammedNo ratings yet
- Lecture 8ADocument17 pagesLecture 8AAbdullah EwaisNo ratings yet
- Quartarone 2004Document11 pagesQuartarone 2004vanogig777No ratings yet
- Transcranial Magnetic Stimulation (TMS) - AskDocument42 pagesTranscranial Magnetic Stimulation (TMS) - AskPersonal growthNo ratings yet
- LTPDocument6 pagesLTPsademcfadden757No ratings yet
- Physiology, Neuromuscular Junction of Skeletal MuscleDocument8 pagesPhysiology, Neuromuscular Junction of Skeletal Musclemethmal subasingheNo ratings yet
- Intraoperative Nerve MonitoringDocument47 pagesIntraoperative Nerve MonitoringAkhil Thomas JacobNo ratings yet
- Neuromuscular Junction Disorders Beyond Myasthenia GravisDocument11 pagesNeuromuscular Junction Disorders Beyond Myasthenia Gravisfaithless.kzNo ratings yet
- Clinical Electro Physiological TestingDocument22 pagesClinical Electro Physiological TestingPaul VkNo ratings yet
- Nerve Conduction VelocityDocument28 pagesNerve Conduction VelocitySheron MathewNo ratings yet
- Monitoring of Neuromuscular Junction: Dr. D. Padmaja Dr. Srinivas ManthaDocument10 pagesMonitoring of Neuromuscular Junction: Dr. D. Padmaja Dr. Srinivas ManthakoolstaroneNo ratings yet
- Overview Nerves ConectionDocument41 pagesOverview Nerves ConectionD Angelo Clavijo SalazarNo ratings yet
- 2022 Set-EXCITABLE TISSUES Membrane Potential & NeuronsDocument53 pages2022 Set-EXCITABLE TISSUES Membrane Potential & NeuronsSamuel BenjaminNo ratings yet
- Lin 1993Document13 pagesLin 1993Stress LessNo ratings yet
- Aqsa Ppt Final Synapse PropertiesDocument13 pagesAqsa Ppt Final Synapse PropertiesAmber AqsaNo ratings yet
- PT Notes: Electrodiagnostic Procedures: Traditional Electrical Evaluation TestsDocument4 pagesPT Notes: Electrodiagnostic Procedures: Traditional Electrical Evaluation TestsFaisal QureshiNo ratings yet
- The Auditory Middle Latency Response, Evoked UsingDocument4 pagesThe Auditory Middle Latency Response, Evoked UsingCabinet VeterinarNo ratings yet
- 4 NCV1Document115 pages4 NCV1sridhar100% (2)
- Electrotherapy 1 Viva QuestionsDocument9 pagesElectrotherapy 1 Viva QuestionsAmaan Shafique100% (3)
- Lecture Synapses, Properties & Transmission Dr. RoomiDocument22 pagesLecture Synapses, Properties & Transmission Dr. RoomiMudassar Roomi100% (2)
- Fundamentals of Medical Physiology Harminder - Unlocked - Split - 86Document5 pagesFundamentals of Medical Physiology Harminder - Unlocked - Split - 86maruf141992No ratings yet
- Nerve 1 ST 2000Document6 pagesNerve 1 ST 2000Mkhize KhabazelaNo ratings yet
- Neural Signaling Med 1Document42 pagesNeural Signaling Med 1sally.kh.mhNo ratings yet
- PHYANA Reviwer: Frog 8-16, 35Document4 pagesPHYANA Reviwer: Frog 8-16, 35BadethNo ratings yet
- PsychpharmDocument3 pagesPsychpharmTVISHA SINGH 2337563No ratings yet
- L1 Neurons and Neuronal NetworksDocument4 pagesL1 Neurons and Neuronal NetworksmoshlingmomoNo ratings yet
- Sources of Biomedical SignalsDocument22 pagesSources of Biomedical Signalsshamyu dhiyaNo ratings yet
- Chapter 3 and 4 - Muscles and NerveDocument19 pagesChapter 3 and 4 - Muscles and Nervetahira UroojNo ratings yet
- Chasing Men on Fire: The Story of the Search for a Pain GeneFrom EverandChasing Men on Fire: The Story of the Search for a Pain GeneNo ratings yet
- Jaques Dalcroze S Music Based Rhythmic Training Affects Gait Parameters and Quality of Life in Parkinson S Disease 11687Document19 pagesJaques Dalcroze S Music Based Rhythmic Training Affects Gait Parameters and Quality of Life in Parkinson S Disease 11687Raghu NadhNo ratings yet
- No Data FoundDocument1 pageNo Data FoundRaghu NadhNo ratings yet
- Provisional Merit List For The Post Code: 1 - ConsultantsDocument73 pagesProvisional Merit List For The Post Code: 1 - ConsultantsRaghu NadhNo ratings yet
- Cancerandexercise 161004225344Document30 pagesCancerandexercise 161004225344Raghu Nadh100% (1)
- Tools and ScalesDocument47 pagesTools and ScalesRaghu NadhNo ratings yet
- General Neurological Assessment: Shemjaz Arakkal MDocument54 pagesGeneral Neurological Assessment: Shemjaz Arakkal MRaghu NadhNo ratings yet
- MPT-1st Year 19pDocument19 pagesMPT-1st Year 19pRaghu Nadh50% (2)
- NHM Spmu Recruitment Notification 2020Document6 pagesNHM Spmu Recruitment Notification 2020Raghu NadhNo ratings yet
- NHM Information To The Candidates 2020 PDFDocument1 pageNHM Information To The Candidates 2020 PDFRaghu NadhNo ratings yet
- Tendon Transfers and Upper Limb Disorders: Aws KhanfarDocument41 pagesTendon Transfers and Upper Limb Disorders: Aws KhanfarRaghu Nadh100% (1)
- Egen Klassifikation Scale Version 2 (EK2) Steffensen 2008Document2 pagesEgen Klassifikation Scale Version 2 (EK2) Steffensen 2008Raghu NadhNo ratings yet
- DR M Ushashree 1 Yr PG Gandhi Medical CollegeDocument58 pagesDR M Ushashree 1 Yr PG Gandhi Medical CollegeRaghu Nadh100% (1)
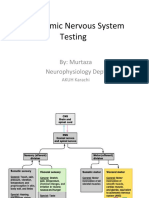
- Autonomic Nervous System Testing: By: Murtaza Neurophysiology DeptDocument41 pagesAutonomic Nervous System Testing: By: Murtaza Neurophysiology DeptRaghu NadhNo ratings yet
- NSAA Only ManualVersion-2.0 May-2017Document19 pagesNSAA Only ManualVersion-2.0 May-2017Raghu NadhNo ratings yet
- The Immune Hallmarks of Severe CovidDocument30 pagesThe Immune Hallmarks of Severe CovidRaghu NadhNo ratings yet
- Guidance On Rapid Antibody Test Kits For Covid-19: S. No. Name of Company Name of Kit Lot No./batch NoDocument2 pagesGuidance On Rapid Antibody Test Kits For Covid-19: S. No. Name of Company Name of Kit Lot No./batch NoRaghu NadhNo ratings yet
- Issuance of SC or ST CertificatesDocument32 pagesIssuance of SC or ST CertificatesRaghu NadhNo ratings yet
- CTH D Dimers May 2 2013 PDFDocument42 pagesCTH D Dimers May 2 2013 PDFRaghu NadhNo ratings yet
- MPTH Thesis Topic List 2010 - : Name of The Student Department Name of Thesis Topic StatusDocument6 pagesMPTH Thesis Topic List 2010 - : Name of The Student Department Name of Thesis Topic StatusRaghu NadhNo ratings yet
- RPH Clasp Assembly - A Simple Alternative To Traditional DesignsDocument3 pagesRPH Clasp Assembly - A Simple Alternative To Traditional DesignsFaheemuddin Muhammad0% (1)
- Biology Paper 1 - Lesson ListDocument2 pagesBiology Paper 1 - Lesson ListamaarNo ratings yet
- Crisis CounselingDocument60 pagesCrisis Counselingpaul macharia100% (6)
- The Circulatory System (Heart)Document3 pagesThe Circulatory System (Heart)NinaNo ratings yet
- đề 27Document8 pagesđề 27bichngocvonagiNo ratings yet
- Migration in FishesDocument1 pageMigration in FishesSadiq MakandarNo ratings yet
- Kci Fi002028796Document31 pagesKci Fi002028796hfkhgyNo ratings yet
- Lehmann Et Al - 2020Document24 pagesLehmann Et Al - 2020zeinab.smillieNo ratings yet
- SULIET NEW YR RinaDocument15 pagesSULIET NEW YR RinaWahyuningsiNo ratings yet
- Kunal Narayan 6th SemDocument14 pagesKunal Narayan 6th SemSpriha GogoiNo ratings yet
- Stress and Coping Styles To StudentsDocument8 pagesStress and Coping Styles To StudentsArien Kaye VallarNo ratings yet
- 0610 s12 QP 12 PDFDocument20 pages0610 s12 QP 12 PDFmath magicNo ratings yet
- Biology Practical Exam 51 QuestionsDocument6 pagesBiology Practical Exam 51 Questionstrizahk886No ratings yet
- Yousef Lababneh - Midterm - G.18Document26 pagesYousef Lababneh - Midterm - G.18Ahmad SobihNo ratings yet
- Case Presentation On Birth AsphyxiaDocument4 pagesCase Presentation On Birth AsphyxiaMary MenuNo ratings yet
- Test Bank For Biochemistry A Short Course 2nd Edition John L Tymoczko Isbn 10 1429283602 Isbn 13 9781429283601Document13 pagesTest Bank For Biochemistry A Short Course 2nd Edition John L Tymoczko Isbn 10 1429283602 Isbn 13 9781429283601Donald Pizzo100% (45)
- Pathophysiology-LCHFDocument2 pagesPathophysiology-LCHFNicole Villanueva, BSN - Level 3ANo ratings yet
- GenBio 3rd QDocument5 pagesGenBio 3rd QQueng ElediaNo ratings yet
- Absorbent CottonDocument2 pagesAbsorbent CottonsanketgroverNo ratings yet
- Breathing at Depth Physiologic and Clinical Aspects of Diving While Breathing Compressed Gas.Document26 pagesBreathing at Depth Physiologic and Clinical Aspects of Diving While Breathing Compressed Gas.FebyNo ratings yet
- Finalppt 2Document16 pagesFinalppt 2priyankaNo ratings yet
- Fish ProductionDocument34 pagesFish Productionit rewa100% (1)
- Detailed Notes - Topic 1 The Nature and Variety of Living Organisms - Edexcel Biology IGCSEDocument4 pagesDetailed Notes - Topic 1 The Nature and Variety of Living Organisms - Edexcel Biology IGCSEpreet kaurNo ratings yet
- Anatomy Physiology of The SkinDocument52 pagesAnatomy Physiology of The SkinRune_Zeit100% (1)
- Assessment of Various Heavy Metals in Surface Water of Polluted Sites in The Lower Stretch of River Ganga, West Bengal: A Study For Ecological ImpactDocument6 pagesAssessment of Various Heavy Metals in Surface Water of Polluted Sites in The Lower Stretch of River Ganga, West Bengal: A Study For Ecological ImpactpseudomonasaeruginosaNo ratings yet
- B Blab 7 Panel Spring 2012Document16 pagesB Blab 7 Panel Spring 2012pzaballero7063No ratings yet
- Leaf Cutter Ants: by Mikki SadilDocument5 pagesLeaf Cutter Ants: by Mikki SadilAlle LunagNo ratings yet
- Acid Base BalanceDocument56 pagesAcid Base BalanceVirendra Joshi100% (2)
- Learning Activity Sheet in TLE (Wellness Massage) : Third Quarter-Week 5Document12 pagesLearning Activity Sheet in TLE (Wellness Massage) : Third Quarter-Week 5Kim Caguioa100% (2)
- Finkeldey - Tropical Forest Genetics PDFDocument318 pagesFinkeldey - Tropical Forest Genetics PDFLewisKarl100% (1)