Blood Collection: Routine Venipuncture and Specimen Handling
Blood Collection: Routine Venipuncture and Specimen Handling
Download as docx, pdf, or txt
At a glance
Powered by AI
The key takeaways are the proper procedures and techniques for performing routine venipuncture and handling blood specimens, including patient identification, equipment used, labeling samples, and common problems that may occur.
The essential steps for every successful blood collection procedure are: patient comfort, hand hygiene, patient identification, assessing patient disposition, checking requisition form, labeling tubes, selecting puncture site, preparing equipment/patient/site, performing puncture and collecting sample(s), recognizing complications, and assessing need for re-collection.
The key elements that must be included on a requisition form are: patient name, ID number, date of birth, sex, requesting physician name, source of specimen, date and time of collection, phlebotomist initials, and requested test(s).
You might also like
- Hesi Exit Exam ReviewDocument35 pagesHesi Exit Exam ReviewIndia91% (92)
- Sample Policy: Reporting Test Results: Philosophy and PurposeDocument8 pagesSample Policy: Reporting Test Results: Philosophy and PurposeDarren CariñoNo ratings yet
- Service Manual: Volumetric Infusion PumpsDocument60 pagesService Manual: Volumetric Infusion PumpsPiotr Okorski100% (2)
- Venipuncture YmcDocument7 pagesVenipuncture Ymcdondon nobleNo ratings yet
- Lab Policies Urinalysis - Clinetek Status and Visual Lab 1583Document17 pagesLab Policies Urinalysis - Clinetek Status and Visual Lab 1583hunnylandNo ratings yet
- Phlebotomy CompetencyDocument4 pagesPhlebotomy Competencyjon dowNo ratings yet
- Phlebotomy Lab 1Document34 pagesPhlebotomy Lab 1Iris Barrera100% (1)
- Aubf Mid PPT Topic 2 (Part 2)Document12 pagesAubf Mid PPT Topic 2 (Part 2)Lovely B. AlipatNo ratings yet
- 3M Ranger Fluid Warmer - Quick Troubleshooting GuideDocument4 pages3M Ranger Fluid Warmer - Quick Troubleshooting GuideJack WhitenerNo ratings yet
- L - ALANINE 8.2 G - 100 ML, L - GLUTAMINE 13.46 G - 100 ML (Dipeptiven Solution Injection)Document4 pagesL - ALANINE 8.2 G - 100 ML, L - GLUTAMINE 13.46 G - 100 ML (Dipeptiven Solution Injection)ddandan_2No ratings yet
- What Is Basic IV Therapy Training? TheDocument9 pagesWhat Is Basic IV Therapy Training? TheFilipino Nurses Central100% (2)
- Phlebotomy - Lab Draws Final 09.17.2015Document8 pagesPhlebotomy - Lab Draws Final 09.17.2015ashanti wrightNo ratings yet
- Specimen Collection PDFDocument33 pagesSpecimen Collection PDFadadan100% (1)
- 01 Blood CollectionDocument120 pages01 Blood CollectionBianca OcampoNo ratings yet
- PHLEBDocument23 pagesPHLEBYoussra MohamedNo ratings yet
- Blood CollectionDocument24 pagesBlood CollectionOla ALmadan100% (1)
- Influenza A+B-Product Insert-Acro BiotechDocument2 pagesInfluenza A+B-Product Insert-Acro BiotechNANTHA KUMARAN100% (1)
- Phlebotomy Review QuestionsDocument3 pagesPhlebotomy Review QuestionsMaria Isabel Trujillo ParralesNo ratings yet
- QA03005 Critical Testand Critical Result ReportingDocument7 pagesQA03005 Critical Testand Critical Result Reportingdebbie o. azcunaNo ratings yet
- Work Flow of Lab Duties and RespDocument6 pagesWork Flow of Lab Duties and RespKate Camat FaminialagaoNo ratings yet
- Job Description:: Phlebotomists DutiesDocument7 pagesJob Description:: Phlebotomists DutiesRajeev PareekNo ratings yet
- Blood Specimen Collection and ProcessingDocument6 pagesBlood Specimen Collection and ProcessingIzkandar RitzzneyNo ratings yet
- Specimen Handling in Patho LabDocument23 pagesSpecimen Handling in Patho Labclaimstudent3515No ratings yet
- A) Purpose of The Examination:: Sop No. Imm /Qm/10 Issue No.: 04 ISSUE DATE: 15april 2015 REV. NO.: 00 Rev. Date: 00Document7 pagesA) Purpose of The Examination:: Sop No. Imm /Qm/10 Issue No.: 04 ISSUE DATE: 15april 2015 REV. NO.: 00 Rev. Date: 00prityNo ratings yet
- Review QuestionsDocument10 pagesReview Questionsmiguel gaquit100% (1)
- Week 1 Pmls2Document45 pagesWeek 1 Pmls2Dayledaniel SorvetoNo ratings yet
- Specimen Collection and Transporation Instructions-1Document6 pagesSpecimen Collection and Transporation Instructions-1Marvel Vision100% (1)
- Sample Collection, Handling and TransportationDocument34 pagesSample Collection, Handling and TransportationMuhammad ShoaibNo ratings yet
- Haematology 1st Ed. 2013Document83 pagesHaematology 1st Ed. 2013Bakht Beland100% (1)
- Microbiology Work InstructionsDocument58 pagesMicrobiology Work InstructionsJam SanchezNo ratings yet
- Needle Stick Injury & Fire SafetyDocument20 pagesNeedle Stick Injury & Fire SafetySayan GhoshalNo ratings yet
- Piccolo Xpress Chemistry Analyser SOPDocument16 pagesPiccolo Xpress Chemistry Analyser SOPBahamas Wellness Diagnostic ServicesNo ratings yet
- Phlebotomy Reminders By: Eugene VillanuevaDocument5 pagesPhlebotomy Reminders By: Eugene VillanuevaNix BatallerNo ratings yet
- Slide Preparation of Cerebrospinal Fluid For Cytological ExaminationDocument3 pagesSlide Preparation of Cerebrospinal Fluid For Cytological ExaminationMurshed HaidarNo ratings yet
- Pre-Analytical Consideration and Venipuncture ComplicationsDocument52 pagesPre-Analytical Consideration and Venipuncture ComplicationsVenom100% (1)
- Catheterisation Standard Operating ProcedureDocument27 pagesCatheterisation Standard Operating ProcedureSherly RositaNo ratings yet
- Quality Manual v10 PDFDocument34 pagesQuality Manual v10 PDFmissknowalotNo ratings yet
- Lesson-09 MODUL PDFDocument9 pagesLesson-09 MODUL PDFanggaririn100% (2)
- PhlebotomyDocument62 pagesPhlebotomyKristinaNo ratings yet
- Quality Control in Histopathology - PPTX Edited - PPTX No 1Document30 pagesQuality Control in Histopathology - PPTX Edited - PPTX No 1Medicine 0786No ratings yet
- Gynecological Specimens - Learning Module 4Document16 pagesGynecological Specimens - Learning Module 4vikithiruvarooran100% (1)
- SOP For ABO GroupingDocument5 pagesSOP For ABO GroupingDUKENo ratings yet
- Pro68-01 Manual Urin Micro SOPDocument20 pagesPro68-01 Manual Urin Micro SOPesraa asemNo ratings yet
- Strategies For Improving Operational Effectiveness in The Clinical Laboratoryat King Fahd Armed Forces Hospital (Kfafh)Document7 pagesStrategies For Improving Operational Effectiveness in The Clinical Laboratoryat King Fahd Armed Forces Hospital (Kfafh)IJAR JOURNALNo ratings yet
- Phlebotomy TechniquesDocument39 pagesPhlebotomy Techniquesnatalieshirley100% (1)
- Lab Manual 11102016 PDFDocument239 pagesLab Manual 11102016 PDFDesyAyu DzulfaAry EomutNo ratings yet
- Self Assessment - LabDocument6 pagesSelf Assessment - LabHend SalahNo ratings yet
- Tissue Processing For TEM: Fixation, Rinsing, Dehydration and EmbeddingDocument30 pagesTissue Processing For TEM: Fixation, Rinsing, Dehydration and EmbeddingBhaskar Ganguly100% (1)
- Quality Manual BacteriologyDocument126 pagesQuality Manual BacteriologyJam SanchezNo ratings yet
- Chapter 7 PHLEBDocument34 pagesChapter 7 PHLEBCess PadillaNo ratings yet
- Specimen Rejection Criteria - The Doctors LaboratoryDocument2 pagesSpecimen Rejection Criteria - The Doctors LaboratoryRevathyNo ratings yet
- Manual, Blood CultureDocument41 pagesManual, Blood CultureFilipus HendiantoNo ratings yet
- 300-5208 B BFM Clsi SopDocument23 pages300-5208 B BFM Clsi SopnjujjnjnjjnnjNo ratings yet
- Poct - QCDocument43 pagesPoct - QCKinjalka GhoshNo ratings yet
- Blood Collection TechniquesDocument26 pagesBlood Collection TechniquesJoe A QuintanaNo ratings yet
- Lecture 30-Basic Principles of Blood Gas Examination-Dr. Windarwati, SP - PK (K), M.SC (2018)Document76 pagesLecture 30-Basic Principles of Blood Gas Examination-Dr. Windarwati, SP - PK (K), M.SC (2018)NOVI UMAMI UMAMINo ratings yet
- Blood Sample Collection ProcedureDocument7 pagesBlood Sample Collection Procedurekavaim001No ratings yet
- Sabouraud AgarDocument6 pagesSabouraud AgarFrancesca Pereda100% (1)
- Maintenance of The Essential Equipment in Labs BBsDocument14 pagesMaintenance of The Essential Equipment in Labs BBsRam Mohan SNo ratings yet
- Phlebotomy: Diagnose and Monitor Medical ConditionsDocument2 pagesPhlebotomy: Diagnose and Monitor Medical ConditionsVera June RañesesNo ratings yet
- Lyle E. Lundblad, MD Disciplinary ActionDocument9 pagesLyle E. Lundblad, MD Disciplinary ActionjanefdocsNo ratings yet
- Clinical Chemistry - Introduction To Clinical ChemistryDocument6 pagesClinical Chemistry - Introduction To Clinical Chemistryrosellae.No ratings yet
- Division of Pathology Laboratory HandbookDocument46 pagesDivision of Pathology Laboratory HandbookIsmail Kader NitteNo ratings yet
- Objectives: Pre-Analytical Considerations in PhlebotomyDocument9 pagesObjectives: Pre-Analytical Considerations in PhlebotomyMr. Potatohead100% (1)
- Preview H03-A6Document11 pagesPreview H03-A6Khatapk DotcomNo ratings yet
- Atlas of Surgical Pathology GrossingFrom EverandAtlas of Surgical Pathology GrossingMonica B. LemosNo ratings yet
- Lecture Notes BacteriologyDocument133 pagesLecture Notes BacteriologyLovely B. AlipatNo ratings yet
- 4 Chemical Examination of Urine PDFDocument12 pages4 Chemical Examination of Urine PDFLovely B. AlipatNo ratings yet
- Imvic Reaction (Indole, Methyl Red, Voges-Proskauer, Citrate)Document1 pageImvic Reaction (Indole, Methyl Red, Voges-Proskauer, Citrate)Lovely B. AlipatNo ratings yet
- Hematology Terms and DefinitionsDocument9 pagesHematology Terms and DefinitionsLovely B. AlipatNo ratings yet
- Family of StreptococcaceaeDocument10 pagesFamily of StreptococcaceaeLovely B. AlipatNo ratings yet
- Hemoglobin and HematocritDocument9 pagesHemoglobin and HematocritLovely B. AlipatNo ratings yet
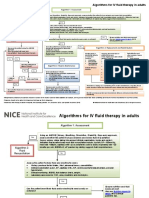
- Intravenous Fluid Therapy in Adults in Hospital Algorithm Poster Set 191627821Document5 pagesIntravenous Fluid Therapy in Adults in Hospital Algorithm Poster Set 191627821Wira Sasmita P100% (1)
- DoxorubicinDocument14 pagesDoxorubicinhasuisoh fightingNo ratings yet
- Protocol For Blunt Abdominal TraumaDocument19 pagesProtocol For Blunt Abdominal TraumaabigailNo ratings yet
- Alphatirta Medica E-Catalog - Jayamas Medica - Karya Indah Medika - Mindray - Fresenius PDFDocument43 pagesAlphatirta Medica E-Catalog - Jayamas Medica - Karya Indah Medika - Mindray - Fresenius PDFFikri AmaliaNo ratings yet
- Tube Feeding Handouts 102819Document4 pagesTube Feeding Handouts 102819MariaNo ratings yet
- Cao Et Al 2022 Perioperative Fluid Management in Surgical Patients A ReviewDocument8 pagesCao Et Al 2022 Perioperative Fluid Management in Surgical Patients A Reviewyqxdbkd868No ratings yet
- A.) 62 Yo Male, S/P (Status Post) Exploratory Laparotomy Secondary Intestinal ObstructionDocument4 pagesA.) 62 Yo Male, S/P (Status Post) Exploratory Laparotomy Secondary Intestinal ObstructionKate Aenyle AgsoyNo ratings yet
- Benton DixonDocument9 pagesBenton DixonKunjal Kumar SinghNo ratings yet
- Assessment of The Critically Ill Patients and Their FamiliesDocument48 pagesAssessment of The Critically Ill Patients and Their Familiesjhing_apdan100% (2)
- Ob2rle Sas 3Document18 pagesOb2rle Sas 3Meow MeowNo ratings yet
- Complications of IV TherapyDocument2 pagesComplications of IV TherapyMarinill SolimanNo ratings yet
- Cytarabine Plus Idarubicin of Daunorubicin (LMA)Document8 pagesCytarabine Plus Idarubicin of Daunorubicin (LMA)Rocio SolervicensNo ratings yet
- Glucose InfusionDocument5 pagesGlucose InfusionPudyo KriswhardaniNo ratings yet
- INTRAVENOUSDocument38 pagesINTRAVENOUSLorelyn DelfinNo ratings yet
- HESI Women's Health:Newborn DrugsDocument8 pagesHESI Women's Health:Newborn Drugsisapatrick8126No ratings yet
- Magnesium Sulfa-WPS OfficeDocument21 pagesMagnesium Sulfa-WPS OfficeNeha SinghNo ratings yet
- JPN 321 Autumn 2019 PDFDocument60 pagesJPN 321 Autumn 2019 PDFjumantoNo ratings yet
- ChemotherapyDocument44 pagesChemotherapyJohn Mark Paracad100% (1)
- Bomba de Infiltracion Wells Johnson Manual OperacionDocument6 pagesBomba de Infiltracion Wells Johnson Manual OperacionDiana PedrozaNo ratings yet
- AIP-1200V Infusion Pump User ManualDocument57 pagesAIP-1200V Infusion Pump User ManualJim DonaireNo ratings yet
- Neonatal Care ClinicalDocument230 pagesNeonatal Care Clinicalأبو فضل الصلاحيNo ratings yet
- Objective Questions For NursingDocument53 pagesObjective Questions For NursingBIBI MOHANAN0% (1)
- Cisplatin Etoposide (Intravenous)Document7 pagesCisplatin Etoposide (Intravenous)Nurul Kamilah SadliNo ratings yet
- Slide 2 National Patient SafeDocument34 pagesSlide 2 National Patient Safeapi-3697326No ratings yet
- Technical ReportDocument27 pagesTechnical ReportAgbama Christopher ErunsunraNo ratings yet