Psychiatric Mental Health Comprehensive Case Study
Psychiatric Mental Health Comprehensive Case Study
Download as docx, pdf, or txt
At a glance
Powered by AI
The case study provides details about a 16-year-old patient named K.B. who was admitted to an inpatient psychiatric hospital for suicidal ideation related to her diagnosis of major depressive disorder. The case study documents her experience in treatment and recovery.
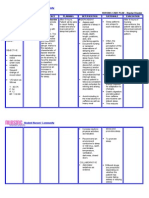
K.B. has a diagnosis of major depressive disorder and has experienced symptoms such as suicidal thoughts, loss of interest, feelings of hopelessness, difficulty sleeping, and social isolation.
During her hospitalization, K.B. participated in group therapy, learned new coping skills, and was prescribed medication to manage her depression. She showed improvement in her symptoms.
You might also like
- Neural Control & Coordination PowernotesDocument2 pagesNeural Control & Coordination PowernotesSushmit Srivastava83% (6)
- Expressed Emotion: Camberwell Family InterviewDocument3 pagesExpressed Emotion: Camberwell Family Interviewaastha jainNo ratings yet
- TBRBiology 1Document372 pagesTBRBiology 1Fabliha Huq100% (11)
- The Science of Monatomic GoldDocument6 pagesThe Science of Monatomic GoldLaron Clark75% (4)
- Chapter 03Document75 pagesChapter 03Tony DiPierryNo ratings yet
- SSRI (Selective Serotonin Reuptake Inhibitor)Document1 pageSSRI (Selective Serotonin Reuptake Inhibitor)Mike EveretteNo ratings yet
- Case Report: Psychotic Disorder Due To EpilepsyDocument8 pagesCase Report: Psychotic Disorder Due To EpilepsyAshraf IlmanNo ratings yet
- Final Period - Assignment NCM 105Document3 pagesFinal Period - Assignment NCM 105Chester NicoleNo ratings yet
- Sample Substance Use Conceptualization and Treatment PlanDocument9 pagesSample Substance Use Conceptualization and Treatment PlanNORAZLINA BINTI MOHMAD DALI / UPM100% (2)
- Psychotherapies and Therapeutic ModalitiesDocument153 pagesPsychotherapies and Therapeutic ModalitiesAsther MantuaNo ratings yet
- Carlson, 2005 - Psychology. The Science of Behaviour PDFDocument75 pagesCarlson, 2005 - Psychology. The Science of Behaviour PDFAnonymous gO4lgf286F100% (1)
- Ashton Manual English PDFDocument58 pagesAshton Manual English PDFMalissa Bowen100% (2)
- Psych Case StudyDocument10 pagesPsych Case Studyapi-455759072No ratings yet
- Comprehensive Case StudyDocument10 pagesComprehensive Case Studyapi-545708059No ratings yet
- Psychotherapy: Therapy SessionsDocument6 pagesPsychotherapy: Therapy SessionsCarlos RochaNo ratings yet
- MSE Sample PDFDocument5 pagesMSE Sample PDFSam Raven AndresNo ratings yet
- Mental Status Exam in DepressionDocument2 pagesMental Status Exam in DepressionChris PenNo ratings yet
- Concept Map For Paranoid SchizzopreniaDocument4 pagesConcept Map For Paranoid SchizzopreniaJu Lie Ann100% (1)
- Mental Health Case StudyDocument15 pagesMental Health Case Studyapi-508142358No ratings yet
- PSYCHOPHARMACOLOGYDocument2 pagesPSYCHOPHARMACOLOGYJulia Rae Delos SantosNo ratings yet
- The Mental Status ExaminationDocument4 pagesThe Mental Status ExaminationFreddy Jr PerezNo ratings yet
- MSEDocument20 pagesMSEJenny YenNo ratings yet
- Mental Status ExaminationDocument4 pagesMental Status ExaminationZamranos67% (3)
- Case Study - Mental Status ExaminationDocument5 pagesCase Study - Mental Status ExaminationSrivathsanNo ratings yet
- Introduction To Psychological InterventionsDocument26 pagesIntroduction To Psychological InterventionsJay Mark Cabrera100% (1)
- Mental Status ExamDocument2 pagesMental Status Examkristel_nicole18yahoNo ratings yet
- Mental Status Examination - Bring To LectureDocument6 pagesMental Status Examination - Bring To LectureJae ChoiNo ratings yet
- Case StudyDocument14 pagesCase Studyapi-546705901No ratings yet
- Depressed Diane-Case Study On DepressionDocument27 pagesDepressed Diane-Case Study On DepressionFarhath Jabien100% (1)
- John NashDocument3 pagesJohn NashAlyx UbiadasNo ratings yet
- Final Capstone PaperDocument15 pagesFinal Capstone Paperapi-478784238No ratings yet
- Therapeutic Communication - Doc 12345Document8 pagesTherapeutic Communication - Doc 12345KBSNo ratings yet
- Psychological Report Writing: Adapted From UP-PGH FormatDocument22 pagesPsychological Report Writing: Adapted From UP-PGH FormatAhmad AliNo ratings yet
- Somatoform DisordersDocument6 pagesSomatoform Disordersgeorgeloto12No ratings yet
- Mental Status ExaminationDocument4 pagesMental Status ExaminationavigaeljoieNo ratings yet
- Basic Principles of Psychiatric NursingDocument5 pagesBasic Principles of Psychiatric NursingJo C Cuilan100% (1)
- The Mental Status ExaminationDocument7 pagesThe Mental Status Examinationdra.hadleyNo ratings yet
- Bipolar NCPDocument2 pagesBipolar NCPAngel BunolNo ratings yet
- Depressive Disorders Social Isolation/Impaired Social InteractionDocument5 pagesDepressive Disorders Social Isolation/Impaired Social InteractionYannesa S. Bantilan - Balbin100% (2)
- Mental Illness Case Analysis 1Document8 pagesMental Illness Case Analysis 1api-545354167No ratings yet
- Case Presentation SchizoDocument13 pagesCase Presentation SchizoBarbara Detaro100% (1)
- Substance-Induced Psychotic DisorderDocument24 pagesSubstance-Induced Psychotic DisorderMuhammad JulpianNo ratings yet
- A CASE sSTUDY OF MARY WITH MDDDocument13 pagesA CASE sSTUDY OF MARY WITH MDDericNo ratings yet
- MSEDocument13 pagesMSERobel Mae Lagos Montaño0% (1)
- OcdDocument11 pagesOcdNem AlNo ratings yet
- G CBT For DelusionDocument23 pagesG CBT For DelusionIoana DarjanNo ratings yet
- Mental Status ExamDocument24 pagesMental Status ExamKevin Leo Lucero AragonesNo ratings yet
- The Management of Acute DystonicDocument2 pagesThe Management of Acute DystonictaqinosNo ratings yet
- Anxiety: Psychiatric DisordersDocument21 pagesAnxiety: Psychiatric DisordersNdoo NdooNo ratings yet
- CBTDocument7 pagesCBTanzeishNo ratings yet
- Psychotherapies 117Document10 pagesPsychotherapies 117Josiah Alecz AranetaNo ratings yet
- Mental Status Examination (Mse)Document28 pagesMental Status Examination (Mse)Rujha Haniena Ahmad RidzuanNo ratings yet
- Hallucinations: Clinical Aspects and Management: Industrial Psychiatry Journal February 2020Document10 pagesHallucinations: Clinical Aspects and Management: Industrial Psychiatry Journal February 2020Nyong FenNo ratings yet
- Case StudyDocument4 pagesCase StudyJESSA MAE BAAYNo ratings yet
- Depression and Psychodynamic PsychotherapyDocument5 pagesDepression and Psychodynamic PsychotherapyRija ChoudhryNo ratings yet
- Reflection Journal About SchizophreniaDocument1 pageReflection Journal About SchizophreniaKit LaraNo ratings yet
- Laboratory Testing and Imaging Studies in PsychiatryDocument54 pagesLaboratory Testing and Imaging Studies in Psychiatrykrysdana22No ratings yet
- NCP001 IsolationDocument2 pagesNCP001 IsolationJoyh LasutaNo ratings yet
- Disturbed Thought ProcessDocument3 pagesDisturbed Thought ProcesschessaNo ratings yet
- The Mental Status ExamDocument7 pagesThe Mental Status ExamAnonymous ewPKlLWtfhNo ratings yet
- MSE1Document3 pagesMSE1Angelo ErispeNo ratings yet
- Group NCPDocument17 pagesGroup NCPNiña Noreen Torres VallegaNo ratings yet
- Racism and Psychiatry: Contemporary Issues and InterventionsFrom EverandRacism and Psychiatry: Contemporary Issues and InterventionsMorgan M. MedlockNo ratings yet
- Solution Focused Harm Reduction: Working effectively with people who misuse substancesFrom EverandSolution Focused Harm Reduction: Working effectively with people who misuse substancesNo ratings yet
- Arousal TheoryDocument30 pagesArousal Theoryapi-359167484No ratings yet
- Section Autonomic Drugs: Chapter 6 Introduction To Autonomic PharmacologyDocument30 pagesSection Autonomic Drugs: Chapter 6 Introduction To Autonomic PharmacologyJonathan TapiasNo ratings yet
- UNIT 3 III Drugs Addiction A.: Reading PassageDocument5 pagesUNIT 3 III Drugs Addiction A.: Reading PassageaNo ratings yet
- Microbes and The MindDocument5 pagesMicrobes and The MindPaula Manalo-Suliguin100% (2)
- Study Guide (Psy 101)Document215 pagesStudy Guide (Psy 101)Allison Tapia100% (1)
- Emerging Memory Devices For Artificial SynapsesDocument21 pagesEmerging Memory Devices For Artificial SynapsesrajeshrsNo ratings yet
- Neurobiology of Addiction: Toward The Development of New TherapiesDocument16 pagesNeurobiology of Addiction: Toward The Development of New Therapiesguessimfloatin GNo ratings yet
- 2 Biopsych Neuroscience and Behavior SlidesDocument48 pages2 Biopsych Neuroscience and Behavior Slidesapaul8096No ratings yet
- AmphetamineDocument87 pagesAmphetamineSATYABBSR83% (12)
- The Secret To Signals: o o o o o o o oDocument3 pagesThe Secret To Signals: o o o o o o o oecdubonNo ratings yet
- Mouse PartyDocument8 pagesMouse PartyPearlNo ratings yet
- M Pharm Pharmacology SylabiDocument23 pagesM Pharm Pharmacology SylabiDr. Anil LandgeNo ratings yet
- 2024 mock paper marking scheme 英文版Document19 pages2024 mock paper marking scheme 英文版ming sum lawNo ratings yet
- Train Your Brain Build A Framework For Clear ThinkingDocument235 pagesTrain Your Brain Build A Framework For Clear ThinkingyashyiNo ratings yet
- Psy Chapter 2Document146 pagesPsy Chapter 2OceanNo ratings yet
- Electrical Chemical Brain StimulationDocument3 pagesElectrical Chemical Brain StimulationNavneet DhimanNo ratings yet
- Ghosh2018 - Happy Hormones at WorkDocument10 pagesGhosh2018 - Happy Hormones at WorkMarco NavaNo ratings yet
- Neuropeptides in Dental Pulp - The Silent Protagonists PDFDocument16 pagesNeuropeptides in Dental Pulp - The Silent Protagonists PDFGerardo AragónNo ratings yet
- Action PotentialDocument24 pagesAction Potentialaniyawarren2160No ratings yet
- Case Study - Bipolar DisorderDocument24 pagesCase Study - Bipolar Disordermattheus101100% (12)
- 1 With Answer KeyDocument13 pages1 With Answer KeySandy Vangyi100% (1)
- Pharma CNSDocument353 pagesPharma CNSEndre Shitaye KulkiNo ratings yet
- Chapter 2 NeurobiologyDocument31 pagesChapter 2 Neurobiologyanitha1118No ratings yet
- Biology 9701 On23 P42Document15 pagesBiology 9701 On23 P422190ibrahimazeemNo ratings yet