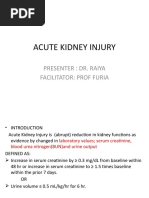
Acute and Chronic Kidney Disease
Acute and Chronic Kidney Disease
Download as pdf or txt
You might also like
- Lifestyle Incurable Diseases enDocument557 pagesLifestyle Incurable Diseases enJairo Suriel100% (1)
- PNLE: Maternal and Child Health Nursing Exam 3Document41 pagesPNLE: Maternal and Child Health Nursing Exam 3Lot Rosit50% (2)
- EMQs For Medical Students Volume 3 PDFDocument15 pagesEMQs For Medical Students Volume 3 PDFAbdulaziz Al-Araifi0% (1)
- 1 - Fluid and Electrolytes (Schwartz Based)Document52 pages1 - Fluid and Electrolytes (Schwartz Based)Alexandra RebosuraNo ratings yet
- Kidneys, L300Document44 pagesKidneys, L300Ko JoNo ratings yet
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesDocument44 pagesElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaNo ratings yet
- Aki & CKD 2024Document68 pagesAki & CKD 2024AhemigishaNo ratings yet
- Hypokalaemia and HyperkalaemiaDocument39 pagesHypokalaemia and HyperkalaemiaRZ NgNo ratings yet
- Chronic Renal Failure (CRF)Document37 pagesChronic Renal Failure (CRF)sivaNo ratings yet
- Chronic Kidney DiseaseDocument35 pagesChronic Kidney DiseaseNur'ain Nabila100% (2)
- Acute Chronic Kidney InjuryDocument29 pagesAcute Chronic Kidney InjuryPriya GKNo ratings yet
- Acute Renal Failure: DR Grania PriceDocument24 pagesAcute Renal Failure: DR Grania PriceCastro KisuuleNo ratings yet
- ARF. Lec, QIMS - For Medical StudentsDocument38 pagesARF. Lec, QIMS - For Medical StudentscodewithibfNo ratings yet
- Pathogenesis and Management of Renal Failure and Replacement Therapy For Stage V Chronic Renal DiseaseDocument30 pagesPathogenesis and Management of Renal Failure and Replacement Therapy For Stage V Chronic Renal DiseaseByzantine Wulandari ParubakNo ratings yet
- 7.acute Renal Failure (ARF)Document20 pages7.acute Renal Failure (ARF)Mahesh RathnayakeNo ratings yet
- AKIDocument22 pagesAKISatyabrata SinghNo ratings yet
- Renal Failure March 2020Document46 pagesRenal Failure March 2020dicksonsamboNo ratings yet
- Chronic Renal Failure: DR Vasudeva Upadhyaya, St. Johns Medical College Bangalore DR Ravi Bhat, SDM DharwadDocument38 pagesChronic Renal Failure: DR Vasudeva Upadhyaya, St. Johns Medical College Bangalore DR Ravi Bhat, SDM Dharwadasharhasan81No ratings yet
- Chronic Kidney DiseaseDocument18 pagesChronic Kidney Diseasephylliswambua661No ratings yet
- Acute Kidney Injury (AKI) :: FeaturesDocument3 pagesAcute Kidney Injury (AKI) :: FeaturesDavid PerezNo ratings yet
- Nephrotic Syndrome + ArfDocument64 pagesNephrotic Syndrome + ArfkrishnasreeNo ratings yet
- Acute Kidney Failure: Dr. Syamsudin, M.Biomed Fakultas Farmasi Universitas PancasilaDocument48 pagesAcute Kidney Failure: Dr. Syamsudin, M.Biomed Fakultas Farmasi Universitas PancasilariyuNo ratings yet
- Acute Kidney InjuryDocument54 pagesAcute Kidney InjuryggplabonNo ratings yet
- Renal Diseases " Review "Document22 pagesRenal Diseases " Review "api-3827876No ratings yet
- Plications of HemodialysisDocument30 pagesPlications of HemodialysisAISHWARYA T DNo ratings yet
- B. Acute Kidney InjuryDocument38 pagesB. Acute Kidney InjuryRachman RhizaNo ratings yet
- Chronic Kidney DiseaseDocument6 pagesChronic Kidney Diseaseashi leginNo ratings yet
- Session 24 Heart FailureDocument15 pagesSession 24 Heart FailuregwivahamaikoNo ratings yet
- Gagal Ginjal Kronik: Jainuri Erik Pratama, M.Farm - Klin., AptDocument30 pagesGagal Ginjal Kronik: Jainuri Erik Pratama, M.Farm - Klin., ApthudayanaNo ratings yet
- Renal NotesDocument11 pagesRenal NotesPatty Pasarilla Passehl100% (2)
- 10 Renal FailureDocument32 pages10 Renal Failureyabais110No ratings yet
- Management of Acute Kidney InjuryDocument31 pagesManagement of Acute Kidney InjurysumitNo ratings yet
- Acute Renal FailureDocument45 pagesAcute Renal FailureRubinNo ratings yet
- Renal Function TestsDocument34 pagesRenal Function TestsMandavi HindNo ratings yet
- Lecture 3 CKDDocument53 pagesLecture 3 CKDPharmswipe KenyaNo ratings yet
- Haematological DisordersDocument28 pagesHaematological DisordersSamuel kuriaNo ratings yet
- Renal Failure PresentationDocument110 pagesRenal Failure PresentationMusa yohana100% (2)
- PathophysiologyDocument39 pagesPathophysiologymawialsaadawyNo ratings yet
- Chronic Kidney DiseaseDocument12 pagesChronic Kidney DiseaseabdurabengNo ratings yet
- Acute Kidney Injury (Acute Renal Failure)Document21 pagesAcute Kidney Injury (Acute Renal Failure)phylliswambua661No ratings yet
- Anaesthesia For Liver DieseaseDocument43 pagesAnaesthesia For Liver DieseaseShehan WijayasiriwardanaNo ratings yet
- Renal Faliure 1Document50 pagesRenal Faliure 1180045No ratings yet
- Acute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and NephrologistDocument43 pagesAcute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and Nephrologistokwadha simionNo ratings yet
- CKD Tipus UJianDocument28 pagesCKD Tipus UJianevanatalia29No ratings yet
- Presentation مسنين عمليDocument19 pagesPresentation مسنين عمليzoubia209No ratings yet
- Fluid and Electrolyte Balance (Rama)Document56 pagesFluid and Electrolyte Balance (Rama)rafiq eimanNo ratings yet
- Systolic Heart FailureDocument66 pagesSystolic Heart FailureFerinaTarizaIINo ratings yet
- Acute Kidney InjuryDocument23 pagesAcute Kidney InjuryBaraka SayoreNo ratings yet
- Renal FailureDocument21 pagesRenal Failureapi-3731294100% (2)
- Chronic Kidney Disease: Pembimbing: Dr. Pit Lan, SPPDDocument25 pagesChronic Kidney Disease: Pembimbing: Dr. Pit Lan, SPPDAnita ZhangNo ratings yet
- Healthy FoodDocument16 pagesHealthy Foodbearp3092No ratings yet
- Fluid & Electrolyte ImbalanceDocument37 pagesFluid & Electrolyte ImbalanceoutkastedNo ratings yet
- Definition-Acute Kidney InjuryDocument6 pagesDefinition-Acute Kidney Injuryashi leginNo ratings yet
- Renal Disease Management DPS 103 Jul 2022Document26 pagesRenal Disease Management DPS 103 Jul 2022spicebunny20No ratings yet
- Acute Kidney InjuryDocument30 pagesAcute Kidney InjuryNidhi JamesNo ratings yet
- AscitesDocument46 pagesAscitesRahul Kumar VermaNo ratings yet
- Chronic Kidney Disease (End-Stage Renal Disease)Document42 pagesChronic Kidney Disease (End-Stage Renal Disease)mercybiwott20No ratings yet
- Chronic Renal FailureDocument3 pagesChronic Renal FailureJashine DajayNo ratings yet
- UNIT 3.1 - AHN - Fluid & Electrolyte ImbalanceDocument31 pagesUNIT 3.1 - AHN - Fluid & Electrolyte Imbalanceannududi378556No ratings yet
- Renal Failure Acute and Chronic: NPN 200 Medical Surgical Nursing IDocument31 pagesRenal Failure Acute and Chronic: NPN 200 Medical Surgical Nursing IJuan ValadezNo ratings yet
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionFrom EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Haematological DisordersDocument28 pagesHaematological DisordersSamuel kuriaNo ratings yet
- Liver DiseaseDocument20 pagesLiver DiseaseSamuel kuriaNo ratings yet
- Neurological DiseaseDocument15 pagesNeurological DiseaseSamuel kuriaNo ratings yet
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaNo ratings yet
- Glomerular DiseasesDocument16 pagesGlomerular DiseasesSamuel kuriaNo ratings yet
- Disorders of Small IntestineDocument41 pagesDisorders of Small IntestineSamuel kuriaNo ratings yet
- Disorders of Esophagus and StomachDocument29 pagesDisorders of Esophagus and StomachSamuel kuriaNo ratings yet
- Disorders of LeucocytesDocument12 pagesDisorders of LeucocytesSamuel kuriaNo ratings yet
- MRCS A SEPT 2021 RecallsDocument38 pagesMRCS A SEPT 2021 Recallsmuawazmuhammad2No ratings yet
- Dialyzer BrochureDocument8 pagesDialyzer BrochureAbdiNo ratings yet
- BioFluid Dynamics, Theory and ApprochDocument517 pagesBioFluid Dynamics, Theory and ApprochAshish Kotwal0% (1)
- My Maxicare Application Form 2023Document2 pagesMy Maxicare Application Form 2023Engilbert Maquera0% (1)
- Master Chart Thesis OsaDocument31 pagesMaster Chart Thesis OsaBiradar VijayNo ratings yet
- Answers in Questions PDFDocument53 pagesAnswers in Questions PDFArasiveluNo ratings yet
- Renin Angiotensin SystemDocument18 pagesRenin Angiotensin SystemLilian EdeniNo ratings yet
- Dr. Iskandar Rachmansjah Dr. Yessi Nurmalasari Dr. Tessa SDocument25 pagesDr. Iskandar Rachmansjah Dr. Yessi Nurmalasari Dr. Tessa SBellavia FransiscaNo ratings yet
- Contoh Analytical Exposition TextDocument3 pagesContoh Analytical Exposition TextAmelia PutriNo ratings yet
- PACES 3 - AbdomenDocument14 pagesPACES 3 - AbdomenDrShamshad KhanNo ratings yet
- Excrection 1Document18 pagesExcrection 1Liyana AziziNo ratings yet
- Chapter 26 Urinary System TransesDocument4 pagesChapter 26 Urinary System TransesMohamidin MamalapatNo ratings yet
- Sulfonamides: (Veterinary-Systemic)Document17 pagesSulfonamides: (Veterinary-Systemic)Ursula HilleNo ratings yet
- Bhalani 3.0 Final UpdatedDocument17 pagesBhalani 3.0 Final UpdatedinmymysteriousworldNo ratings yet
- Preeclampsia: Predisposing Factors: Precipitating FactorsDocument2 pagesPreeclampsia: Predisposing Factors: Precipitating FactorsAnton RossiniNo ratings yet
- Hypertensive NephropathyDocument33 pagesHypertensive NephropathyRon OpulenciaNo ratings yet
- Cm2021 AugustDocument72 pagesCm2021 AugustB L A C K N I G H TNo ratings yet
- Anaplastic Sarcoma of The Kidney With Chromosomal AbnormalityDocument5 pagesAnaplastic Sarcoma of The Kidney With Chromosomal AbnormalityJose Alejandro InciongNo ratings yet
- PC Metabolic AcidosisDocument4 pagesPC Metabolic AcidosisErine Emmanuelle Cawaling Hetrosa50% (2)
- PhysioEx Exercise 9 Activity 1Document4 pagesPhysioEx Exercise 9 Activity 1t4gjzhpfjcNo ratings yet
- Renal Physiology ReviewDocument7 pagesRenal Physiology ReviewHOD AnesthesiaNo ratings yet
- 15 MCQsDocument3 pages15 MCQsAisha HnwereyNo ratings yet
- HealthCheck 07oct2023Document18 pagesHealthCheck 07oct2023debahero1No ratings yet
- Nephrology AtfDocument128 pagesNephrology AtfGheorghe AdrianNo ratings yet
- Guidelines On Chronic Kidney Disease: (NKF K/Doqi)Document32 pagesGuidelines On Chronic Kidney Disease: (NKF K/Doqi)Laura PutriNo ratings yet
- Nejmoa2204233 AppendixDocument59 pagesNejmoa2204233 AppendixCindy PenaNo ratings yet
- Chandulal - Nanavati - Bio - Prelim Class 10th IcseDocument4 pagesChandulal - Nanavati - Bio - Prelim Class 10th IcseOmMen GamingNo ratings yet