American Heart Association: Precourse Written Examination May 2001
American Heart Association: Precourse Written Examination May 2001
Download as pdf or txt
You might also like
- ACLS Cheat SheetDocument8 pagesACLS Cheat SheetLenTheRN86% (28)
- ACLS Post TestDocument6 pagesACLS Post TestSheila Tolentino-Belanio73% (79)
- Acls Pre Course Self Assessment Study GuideDocument7 pagesAcls Pre Course Self Assessment Study Guidenova939100% (11)
- AHA ELearning ACLS Precourse Self-Assessment and Precourse WorkDocument1 pageAHA ELearning ACLS Precourse Self-Assessment and Precourse Work9kjsntkrzcNo ratings yet
- AHA ACLS Megacode ScenariosDocument6 pagesAHA ACLS Megacode ScenariosChad Sanford78% (18)
- ACLS Pretest Questions and Answers 2020 (Full Practice Test)Document23 pagesACLS Pretest Questions and Answers 2020 (Full Practice Test)김민길50% (4)
- ACLS Exam ADocument8 pagesACLS Exam ASean Johnson81% (31)
- ACLS Review TestDocument5 pagesACLS Review Testtostc60% (5)
- ACLS Answer KeyDocument23 pagesACLS Answer KeyKirana Budhiarta94% (17)
- American Heart Association Acls Post Test AnswersDocument4 pagesAmerican Heart Association Acls Post Test AnswersArun Jude Alphonse0% (10)
- ACLS PharmacologyDocument6 pagesACLS PharmacologyEunice Angela Fulgueras88% (8)
- ACLS - Precourse Questions and AnswersDocument18 pagesACLS - Precourse Questions and Answerssuperdockk58% (12)
- 2021 ACLS Study GuideDocument20 pages2021 ACLS Study GuideShane Brown88% (16)
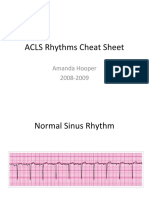
- ACLS Rhythms Cheat SheetDocument21 pagesACLS Rhythms Cheat SheetShannon Hagan Wilson100% (8)
- ACLS PrecourseAssessmentDocument19 pagesACLS PrecourseAssessmentBrigitte Elaine81% (21)
- ACLS Practice Test 1Document6 pagesACLS Practice Test 1tarrynwortmann5319100% (3)
- FREE 2022 ACLS Study Guide - ACLS Made Easy! PDFDocument18 pagesFREE 2022 ACLS Study Guide - ACLS Made Easy! PDFkumar23100% (2)
- TestDocument11 pagesTestzenagit123456100% (1)
- ACLS2Document7 pagesACLS2Jennifer Kaye L. DucaoNo ratings yet
- Cals ReviewbjvjvjDocument14 pagesCals ReviewbjvjvjCarl Jay M Ocariza100% (1)
- Acls QuestionsDocument28 pagesAcls QuestionsDsd100% (1)
- ACLS Pretest Exam AnnotatedDocument21 pagesACLS Pretest Exam AnnotatedMOLLYNo ratings yet
- ACLS PrecourseAssessmentDocument19 pagesACLS PrecourseAssessmentRaiedKhaled100% (2)
- ACLS Rhythms Practice Test 2020 Recognition Rhythm Strips (PDF)Document11 pagesACLS Rhythms Practice Test 2020 Recognition Rhythm Strips (PDF)김민길100% (3)
- Acls Test: 1. Start CPR, Beginning With Chest CompressionsDocument15 pagesAcls Test: 1. Start CPR, Beginning With Chest CompressionsBoby Jomol100% (11)
- ACLS Post Test (Copy) 낱말 카드 - QuizletDocument18 pagesACLS Post Test (Copy) 낱말 카드 - Quizlet김민길100% (2)
- ACLS Algorithms 2020 (Advanced Cardiac Life Support)Document1 pageACLS Algorithms 2020 (Advanced Cardiac Life Support)evelyn k100% (2)
- ACLS Megacode Testing ScenariosDocument12 pagesACLS Megacode Testing Scenariosealm10100% (2)
- Acls DrugsDocument10 pagesAcls DrugsChintami Octavia100% (1)
- ACLS 2020 Algorithms: American Heart Association 2020 GuidelinesDocument8 pagesACLS 2020 Algorithms: American Heart Association 2020 GuidelinesNofi Nurina100% (4)
- Acls Version B QuizDocument9 pagesAcls Version B QuizRokunuz Jahan Rudro0% (1)
- Acls ExamDocument42 pagesAcls ExamScribdTranslations50% (2)
- 12 To 24 HoursDocument45 pages12 To 24 HoursstellaNo ratings yet
- This Is A Single-Answer Multiple-Choice Examination. There Is Only One Correct Answer To Each QuestionDocument8 pagesThis Is A Single-Answer Multiple-Choice Examination. There Is Only One Correct Answer To Each QuestionUgeshwaran Aristotle Reddy50% (2)
- ACLS Practice TestDocument5 pagesACLS Practice Testprettynpink0867% (3)
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- 2011 ACLS Pretest Annotated Answer KeyDocument19 pages2011 ACLS Pretest Annotated Answer KeyMohammed Abdou92% (13)
- ACLS ECGsDocument4 pagesACLS ECGsEman Elzeftawy100% (7)
- ACLS NotesDocument9 pagesACLS Notestasha0% (1)
- ACLSDocument17 pagesACLSms_lezah100% (4)
- Pals With Bls 2016Document53 pagesPals With Bls 2016Etcvh Gvbj100% (2)
- ACLS Test PrintscreenedDocument13 pagesACLS Test Printscreenedhellfireomega67% (9)
- Acls AllDocument71 pagesAcls Allezzat salemNo ratings yet
- Rhythm Recognition - ACLS Medical Training 1Document9 pagesRhythm Recognition - ACLS Medical Training 1Catalina BorquezNo ratings yet
- ACLS Test QuestionsDocument2 pagesACLS Test QuestionsNyle GreyNo ratings yet
- ACLS Exam ADocument8 pagesACLS Exam AAgil Rumboko Sumitro100% (4)
- ACLS PharmacologyDocument5 pagesACLS PharmacologyKuruva MallikarjunaNo ratings yet
- Acls Pretest Answer Key: Rhythm Identification (Part I)Document3 pagesAcls Pretest Answer Key: Rhythm Identification (Part I)aditNo ratings yet
- ACLS QuizletDocument7 pagesACLS Quizletek.9006001No ratings yet
- ACLS Instr Fac GuideDocument43 pagesACLS Instr Fac GuideOnek KothaNo ratings yet
- Acls - Megacode - UpdatedDocument4 pagesAcls - Megacode - UpdatedDivine Dela Pena100% (3)
- BLS Training - Question PaperDocument3 pagesBLS Training - Question PaperNav J Kar100% (3)
- Advance Cardiac Life Support: Short, Sweet and to the PointFrom EverandAdvance Cardiac Life Support: Short, Sweet and to the PointRating: 3 out of 5 stars3/5 (2)
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Adult CCRN Exam Flashcards, Third Edition: Up-to-Date Review and PracticeFrom EverandAdult CCRN Exam Flashcards, Third Edition: Up-to-Date Review and PracticeNo ratings yet
- General Patho Lab2 2Document93 pagesGeneral Patho Lab2 2عبد الرحمن عصام ابوديابNo ratings yet
- Procedure For DefibrillationDocument6 pagesProcedure For DefibrillationTasia DeastutiNo ratings yet
- Family Nursing Care Plan & Community DXDocument65 pagesFamily Nursing Care Plan & Community DXIris Caberte80% (10)
- ECG Rhythm Master I Health And WillnessDocument1 pageECG Rhythm Master I Health And Willnessday alcoberNo ratings yet
- Understanding pharmacology essentials for medication safety 2 edition Edition Lacharity 2024 scribd downloadDocument46 pagesUnderstanding pharmacology essentials for medication safety 2 edition Edition Lacharity 2024 scribd downloaddortymodenuu100% (1)
- The Aga Khan University Hospital Pediatric SCU Course Final Exam Test Paper Name: - UnitDocument5 pagesThe Aga Khan University Hospital Pediatric SCU Course Final Exam Test Paper Name: - UnitUmar RashidNo ratings yet
- Decompensated Congestive Cardiac Failure Secondary To No1Document4 pagesDecompensated Congestive Cardiac Failure Secondary To No1Qi YingNo ratings yet
- IRON5Document11 pagesIRON5scgtm6gc46No ratings yet
- A Phase I Feasibility Study of Yoga On The Physical Health and Coping of Informal CaregiversDocument11 pagesA Phase I Feasibility Study of Yoga On The Physical Health and Coping of Informal CaregiversFranco EliasNo ratings yet
- Kr2med 2004engDocument49 pagesKr2med 2004engSuma LathaNo ratings yet
- At The Hospital Quick Reference Glossary PDFDocument12 pagesAt The Hospital Quick Reference Glossary PDFFaisal IqbalNo ratings yet
- PMLS 2 PrelimsDocument55 pagesPMLS 2 PrelimsCassey Stephane PinedaNo ratings yet
- Advanced Cardiac Life SupportDocument13 pagesAdvanced Cardiac Life SupportEldonVinceIsidroNo ratings yet
- FajtorDocument6 pagesFajtorMarshaAsmaraditaNo ratings yet
- Histologi Organ Dan Sistem Sirkulasi PoltekkesDocument28 pagesHistologi Organ Dan Sistem Sirkulasi PoltekkesJeon WonwooNo ratings yet
- 03 Cardiopulmonary PhysiologyDocument17 pages03 Cardiopulmonary Physiologyice cream1000791100% (1)
- Periodic Test in Science 4 1st - 4thDocument17 pagesPeriodic Test in Science 4 1st - 4th엘라엘라No ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationSiddhant GautamNo ratings yet
- Q4 STEM General Biology 2 Week 4Document4 pagesQ4 STEM General Biology 2 Week 4Bernard D. Fajardo Jr.0% (1)
- Nursing Bullets: Fundamentals of Nursing ReviewerDocument44 pagesNursing Bullets: Fundamentals of Nursing ReviewerErl DiamanteNo ratings yet
- Ischemic Heart Disease: Dr. Amin ShneifiDocument65 pagesIschemic Heart Disease: Dr. Amin Shneificarmitjulya228No ratings yet
- 01 - Prevention & Control of Communicable & Non-Communicable DiseaseDocument153 pages01 - Prevention & Control of Communicable & Non-Communicable DiseaseMegat Mohd Azman Adzmi100% (3)
- Bahir Dar University College of Medicine and Other Health ScienceDocument61 pagesBahir Dar University College of Medicine and Other Health ScienceGizachew AsimareNo ratings yet
- Differentiating Abbreviations From Acronyms: MuscleDocument10 pagesDifferentiating Abbreviations From Acronyms: MusclePrince Rener Velasco PeraNo ratings yet
- Effect of Quran On AnxietyDocument8 pagesEffect of Quran On Anxietyezuan wanNo ratings yet
- فەرهەنگی پزیشکی من (Kaka)Document120 pagesفەرهەنگی پزیشکی من (Kaka)mrben2596No ratings yet
- Definition:: Checking The Vital Signs (VS)Document18 pagesDefinition:: Checking The Vital Signs (VS)Loyd Tuvilla100% (1)
- 220 Triathlon UK - January 2024Document120 pages220 Triathlon UK - January 2024Omar Magdy AhmadNo ratings yet
- Delfin Leslie Pearl E. CONCEPT MAPDocument1 pageDelfin Leslie Pearl E. CONCEPT MAPJeremiah Andre Poissonier AyupanNo ratings yet
- Clinical Guidelines MSFDocument311 pagesClinical Guidelines MSFAndrea Z Milano100% (1)