Download as pdf or txt
You might also like
- (PDF Download) Endovascular Skills Guidewire and Catheter Skills For Endovascular Surgery 4th Edition Peter A Schneider Fulll ChapterDocument64 pages(PDF Download) Endovascular Skills Guidewire and Catheter Skills For Endovascular Surgery 4th Edition Peter A Schneider Fulll Chapterncuteleevis100% (2)
- Skills Checklist-Critical CareDocument3 pagesSkills Checklist-Critical CareRom Anog100% (4)
- ICU Procedures ManualDocument64 pagesICU Procedures Manualenumula kumar100% (1)
- CriticalCare - ICU Skills ChecklistDocument8 pagesCriticalCare - ICU Skills Checklistyash Inficare100% (2)
- Medical-Surgical Nursing Knowledge & Skills ChecklistDocument3 pagesMedical-Surgical Nursing Knowledge & Skills Checklistnorthweststaffing100% (1)
- Psychiatric Nursing Knowledge and Skills ChecklistDocument5 pagesPsychiatric Nursing Knowledge and Skills Checklistnorthweststaffing100% (4)
- Pediatric Intensive Care Nursing Knowledge & Skills ChecklistDocument5 pagesPediatric Intensive Care Nursing Knowledge & Skills Checklistnorthweststaffing50% (2)
- Emergency Department Handbook PDFDocument461 pagesEmergency Department Handbook PDFdmallozziNo ratings yet
- 50 Landmark Papers Every Vascular and Endovascular Surgeon Should KnowDocument283 pages50 Landmark Papers Every Vascular and Endovascular Surgeon Should KnowAhmed Elmallah100% (1)
- RN Critical Care Competency ChecklistDocument19 pagesRN Critical Care Competency ChecklistMary ElizabethNo ratings yet
- Department of Nursing Initial Competency Validation Checklist: Orientation: RNDocument4 pagesDepartment of Nursing Initial Competency Validation Checklist: Orientation: RNAmeng GosimNo ratings yet
- Care of Ventilated PatientsDocument2 pagesCare of Ventilated PatientsRaydan Francis Magana Antojado100% (2)
- SBH/HSC Pre-Angiogram/ Angioplasty/Stent ChecklistDocument2 pagesSBH/HSC Pre-Angiogram/ Angioplasty/Stent ChecklistKena Ben100% (2)
- 93 - Operating Room ProtocolDocument25 pages93 - Operating Room ProtocolFelix Kwenandar100% (1)
- Post Anesthesia-Recovery Skills ChecklistDocument6 pagesPost Anesthesia-Recovery Skills Checklistnorthweststaffing100% (1)
- Aldrete Score SheetDocument1 pageAldrete Score SheetBoston GunawanNo ratings yet
- Presentation On Care of Critically Ill PatientDocument9 pagesPresentation On Care of Critically Ill Patientanamika sharmaNo ratings yet
- Patient Transfer Policy v4.0Document34 pagesPatient Transfer Policy v4.0Kharisma Putra100% (1)
- Infection Control Checklist Nursing DepartmentDocument5 pagesInfection Control Checklist Nursing DepartmentKhaskheli Nusrat100% (2)
- NCP Cholecystectomy RevisedDocument7 pagesNCP Cholecystectomy RevisedMariquita Buenafe100% (4)
- Tubing Misconnections Self Assessment For Healthcare FacilitiesDocument38 pagesTubing Misconnections Self Assessment For Healthcare FacilitiesAle Gastelum100% (1)
- PCP Obe-Cbtp Dops Rtp-Acc Form#7Document6 pagesPCP Obe-Cbtp Dops Rtp-Acc Form#7Ko HakuNo ratings yet
- IcuDocument8 pagesIcuBikul Nayar100% (1)
- Intensive Care Unit (ICU) Manual 2020-21Document146 pagesIntensive Care Unit (ICU) Manual 2020-21anithaNo ratings yet
- CCUDocument82 pagesCCUSarah100% (1)
- Manual IcuDocument229 pagesManual IcuMauricio PinneaparNo ratings yet
- Crash Cart Medication and ManagementDocument20 pagesCrash Cart Medication and ManagementSilpa Kuruvilla100% (2)
- Synopsis - Nursing ExcellenceDocument19 pagesSynopsis - Nursing ExcellenceD. Gandhiraj100% (1)
- NABH Staff RatioDocument1 pageNABH Staff RatioRetteri KUMARANNo ratings yet
- ATT 1 Guidelines For ICU Admission-Discharge-And-TriageDocument3 pagesATT 1 Guidelines For ICU Admission-Discharge-And-TriageEmad Zakaria Sayed100% (1)
- Guidelines For ICU Admission Discharge and TriageDocument18 pagesGuidelines For ICU Admission Discharge and TriageTika SartikaNo ratings yet
- Introduction in Critical Care NursingDocument16 pagesIntroduction in Critical Care Nursingedison aoriano100% (2)
- Checklist and Quality Indicators ICU For NABH Accreditation PreparationDocument2 pagesChecklist and Quality Indicators ICU For NABH Accreditation PreparationSanjay Kadam100% (1)
- Emergency Department PolicyDocument18 pagesEmergency Department PolicyKumar Gavali Suryanarayana100% (1)
- Nursing Audit ToolDocument2 pagesNursing Audit Toolalaysa udok100% (3)
- DAILY ROUND Head NurseDocument1 pageDAILY ROUND Head NurseRao Rizwan ShakoorNo ratings yet
- Intensive Care UnitDocument12 pagesIntensive Care UnitAnt OnNo ratings yet
- INDICATORSDocument15 pagesINDICATORSMonish ParmarNo ratings yet
- Hospital Infection Control ManualDocument59 pagesHospital Infection Control Manualابراهيم الحربيNo ratings yet
- Blood Transfusion Single Use PathwayDocument6 pagesBlood Transfusion Single Use Pathwayropusan100% (1)
- Accomplishment Report 2017 - IcuDocument5 pagesAccomplishment Report 2017 - IcuMikhaelEarlSantosTacordaNo ratings yet
- Policy For Patients Under Restraints: Nursing Excellence UnitDocument22 pagesPolicy For Patients Under Restraints: Nursing Excellence UnitjinoNo ratings yet
- Nursing EmpowermentDocument1 pageNursing Empowermentsudhakar pNo ratings yet
- Ic-01-041 Infection Control in DialysisDocument15 pagesIc-01-041 Infection Control in DialysisDerick RanaNo ratings yet
- Central Venous Pressure Monitoring ManualDocument6 pagesCentral Venous Pressure Monitoring ManualCristina L. JaysonNo ratings yet
- Modified Early Warning Score ToolDocument6 pagesModified Early Warning Score Toolcicaklomen100% (1)
- Critical Care NursingDocument41 pagesCritical Care NursingAbirajan50% (2)
- Qi Format For Nursing Indicators (1) .XLSX - 1Document119 pagesQi Format For Nursing Indicators (1) .XLSX - 1Mamatha parella100% (1)
- Accident and EmergenciesDocument5 pagesAccident and EmergenciesArnel AlmutiahNo ratings yet
- Patient Identification PolicyDocument20 pagesPatient Identification PolicyZahwa DhiyanaNo ratings yet
- Assignment ON Documentation: Submitted To: Submitted byDocument12 pagesAssignment ON Documentation: Submitted To: Submitted byNagulan Nagul100% (1)
- DEM Module 1Document48 pagesDEM Module 1Nicolo Martin BelloNo ratings yet
- Improving Operating Theatre Performance Complete Step Guide Without Pic PDFDocument83 pagesImproving Operating Theatre Performance Complete Step Guide Without Pic PDFAddison RousdyNo ratings yet
- Nursing Services Manual, Aiims New Delhi - 25!2!21Document91 pagesNursing Services Manual, Aiims New Delhi - 25!2!21praveenjenaNo ratings yet
- 2019 Audit ChecklistDocument27 pages2019 Audit ChecklistChhaiyaAgrawalNo ratings yet
- ICU Scoring SystemsDocument35 pagesICU Scoring SystemsVijay Gadagi100% (3)
- Adult Critical Care Nursing Knowledge & Skills ChecklistDocument7 pagesAdult Critical Care Nursing Knowledge & Skills Checklistnorthweststaffing100% (3)
- Critical Care Nurse Skills ChecklistDocument4 pagesCritical Care Nurse Skills Checklistspartacuslives100% (1)
- Rapid Response TeamDocument4 pagesRapid Response TeamMichael SilvaNo ratings yet
- Quality Manager Job Description - 09-13Document3 pagesQuality Manager Job Description - 09-13DrSaswat LincolnNo ratings yet
- Monitoring Tool For Evluation of Performance of The Staff Nurse During Admission, Transfer & Discharge of The PatientDocument12 pagesMonitoring Tool For Evluation of Performance of The Staff Nurse During Admission, Transfer & Discharge of The Patientmahbuburrahim9553No ratings yet
- Critical Care NursingDocument3 pagesCritical Care NursingMa Christina Herrera AntesNo ratings yet
- SOPs For Infection Control and PreventionDocument25 pagesSOPs For Infection Control and PreventionNoor ButtNo ratings yet
- Safetey BundlesDocument34 pagesSafetey BundlesshafinaNo ratings yet
- DapusDocument4 pagesDapusRiza ZaharaNo ratings yet
- Arteriovenous Malformation (Avm) Di Instalasi Radiologi Rsup DRDocument5 pagesArteriovenous Malformation (Avm) Di Instalasi Radiologi Rsup DRyani radiologyNo ratings yet
- Nextillo Dibs Topics SurgeryDocument13 pagesNextillo Dibs Topics SurgeryRishabh KashyapNo ratings yet
- "Distraction Osteogenesis in Orthodontics: A Comprehensive ReviewDocument8 pages"Distraction Osteogenesis in Orthodontics: A Comprehensive ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Brosur Flat Bottom LengkapDocument4 pagesBrosur Flat Bottom LengkapkhaidirNo ratings yet
- Fetal SkullDocument17 pagesFetal SkullRESHMA AJAYNo ratings yet
- Comeg ArthroDocument36 pagesComeg ArthroAlaa Salam0% (1)
- Kumpulan Journal Kompartemen SindromDocument6 pagesKumpulan Journal Kompartemen SindromBrinna Anindita SatriaNo ratings yet
- Candidate Guide Trauma Case Pelvic TraumaDocument6 pagesCandidate Guide Trauma Case Pelvic Traumadebby nirmasariNo ratings yet
- Medicine 1 3.03b Abdominal PainDocument4 pagesMedicine 1 3.03b Abdominal PainTyra TusingNo ratings yet
- Injury: Jae-Woo Cho, Jinil Kim, Won-Tae Cho, William T. Kent, Hyung-Jin Kim, Jong-Keon OhDocument10 pagesInjury: Jae-Woo Cho, Jinil Kim, Won-Tae Cho, William T. Kent, Hyung-Jin Kim, Jong-Keon OhKrishna CaitanyaNo ratings yet
- (Ebook PDF) Textbook of Critical Care 7th Edition Jean-Louis Vincent - Ebook PDF All ChapterDocument69 pages(Ebook PDF) Textbook of Critical Care 7th Edition Jean-Louis Vincent - Ebook PDF All Chapterdryndalifasi100% (14)
- Cardiopulmonary ResuscitationDocument21 pagesCardiopulmonary ResuscitationjefferyNo ratings yet
- Full Download Oxford Handbook of Obstetrics and Gynaecology, 4th Edition Collins File PDF All Chapter On 2024Document44 pagesFull Download Oxford Handbook of Obstetrics and Gynaecology, 4th Edition Collins File PDF All Chapter On 2024robbeorosil100% (3)
- EsophagogastroduodenosDocument4 pagesEsophagogastroduodenosjulia marie candelarioNo ratings yet
- Larynx Recap 1.1Document8 pagesLarynx Recap 1.1Khalid RefaeyNo ratings yet
- Gow Gates TechniqueDocument3 pagesGow Gates TechniqueAlanNo ratings yet
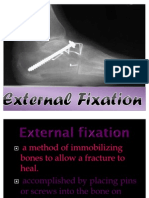
- External FixationDocument23 pagesExternal FixationJc LeeNo ratings yet
- 5 - Anatomy of The BreastDocument18 pages5 - Anatomy of The Breasthabtsh habshaNo ratings yet
- Muscles of The Soft PalateDocument2 pagesMuscles of The Soft PalateJOHN HAROLD CABRADILLANo ratings yet
- Profile: United Management AssociatesDocument17 pagesProfile: United Management AssociatesKhubaib KhawarNo ratings yet
- URO 458909 AA - AurigaXL BrochureDocument4 pagesURO 458909 AA - AurigaXL BrochureAndres Armando Bonuccelli IbañezNo ratings yet
- Etopic PregnancyDocument15 pagesEtopic PregnancyAileenNo ratings yet
- 2.2 Imm Apel2018Document640 pages2.2 Imm Apel2018Tatiana PopaNo ratings yet
- Highalertmedications PDFDocument1 pageHighalertmedications PDFIrza Tarawatu0% (1)