Scenario: Respiratory Disorders
Scenario: Respiratory Disorders
Download as docx, pdf, or txt
You might also like
- Quick Reference Guide To Unique Pet SpeciesDocument624 pagesQuick Reference Guide To Unique Pet SpeciesMartina Brescia100% (1)
- Inbound 2197063521713227868Document11 pagesInbound 2197063521713227868NylNo ratings yet
- Two Way User Guide MN006555A01-AC - Multilingual - Talkabout - Two-Way - Radio - T21X - T27X - Series - User - GuideDocument124 pagesTwo Way User Guide MN006555A01-AC - Multilingual - Talkabout - Two-Way - Radio - T21X - T27X - Series - User - GuideCarbunescu NicolaeNo ratings yet
- IPCC AR6 WGIII PressConferenceSlides PDFDocument28 pagesIPCC AR6 WGIII PressConferenceSlides PDFConstanza Canales SaavedraNo ratings yet
- 300 Spartan Medication EbookletDocument201 pages300 Spartan Medication EbookletSVPSNo ratings yet
- Clash of ClansDocument10 pagesClash of ClansBisma MuhammadNo ratings yet
- Instruction Manual ECP TMDocument33 pagesInstruction Manual ECP TMBryanJermyHendrikNo ratings yet
- 2021 09 01 Art Guide AustraliaDocument254 pages2021 09 01 Art Guide Australiaglauber silvaNo ratings yet
- xxxxPABLO FR PANAMA LETTER OF INTENT MILBERRY CONGODocument1 pagexxxxPABLO FR PANAMA LETTER OF INTENT MILBERRY CONGOHitendraSinh ParmarNo ratings yet
- Assignment OneDocument12 pagesAssignment Onegerrad cortezNo ratings yet
- Synthesis of Some New Pyridazine Derivatives For ADocument15 pagesSynthesis of Some New Pyridazine Derivatives For ADrHamdy KhameesNo ratings yet
- Project AWARE - Hackathon PresentationDocument11 pagesProject AWARE - Hackathon PresentationERUA HACKATHON100% (1)
- New Perspectives On HRMDocument51 pagesNew Perspectives On HRMbennaceur hamouNo ratings yet
- Specifications: Amp CM15RDocument2 pagesSpecifications: Amp CM15ROlivér KissNo ratings yet
- Rdms Chapter 5Document26 pagesRdms Chapter 5vibhav thakurNo ratings yet
- DS9247F CTM530aDocument2 pagesDS9247F CTM530adennisflorianNo ratings yet
- Lab 5 Osmosis and TonicityDocument6 pagesLab 5 Osmosis and TonicityKathleen RussellNo ratings yet
- ZK 29 Control Valve ZK 29 With Radial Stage Nozzle PN 160 DN 25, 50, 80, 100, 150 MM (1, 2, 3, 4, 6")Document4 pagesZK 29 Control Valve ZK 29 With Radial Stage Nozzle PN 160 DN 25, 50, 80, 100, 150 MM (1, 2, 3, 4, 6")Ilic SlobodanNo ratings yet
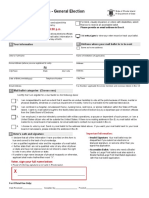
- Mail Ballot Application For Rhode Island General Election.Document2 pagesMail Ballot Application For Rhode Island General Election.Frank MaradiagaNo ratings yet
- Telecommunications Engineering Lab: Section: A Lab No: 5 GR No: Semester: Fall 21-22 DateDocument11 pagesTelecommunications Engineering Lab: Section: A Lab No: 5 GR No: Semester: Fall 21-22 DateShazzadNo ratings yet
- Case4 - Nupetco PPT - PastelDocument45 pagesCase4 - Nupetco PPT - PastelNurul Farah Mohd FauziNo ratings yet
- Industry SectorDocument21 pagesIndustry SectorRavikeshNo ratings yet
- Document 1312021 53807 AM ZrAxTn7pDocument8 pagesDocument 1312021 53807 AM ZrAxTn7pGisselle RodriguezNo ratings yet
- Act Love Sick Setlist LyricsDocument32 pagesAct Love Sick Setlist LyricsMaresol YakitNo ratings yet
- ZolpidemDocument27 pagesZolpidemAntonio SanchezNo ratings yet
- ARTPARK Annual Report 2020-21Document22 pagesARTPARK Annual Report 2020-21Hobi kobiNo ratings yet
- Coronavirus in PhiDocument9 pagesCoronavirus in PhiRoselainy AdapunNo ratings yet
- Intelligence and Its Mesurement FinalDocument57 pagesIntelligence and Its Mesurement FinalEzri Mariveles Coda Jr.No ratings yet
- AAOMS Residency Program ListDocument12 pagesAAOMS Residency Program Listlippincott2011No ratings yet
- AG13A020 InstallDocument12 pagesAG13A020 InstallUziNo ratings yet
- Fall Health & Wellness (October 2022)Document20 pagesFall Health & Wellness (October 2022)Watertown Daily TimesNo ratings yet
- DCNR Fall Foliage Report Oct. 6, 2022Document10 pagesDCNR Fall Foliage Report Oct. 6, 2022Avery Van EttenNo ratings yet
- Pro-Oxidant Strategies - Cancer Treatments ResearchDocument71 pagesPro-Oxidant Strategies - Cancer Treatments ResearchSpore FluxNo ratings yet
- Chapter 7Document15 pagesChapter 7Bea SeloterioNo ratings yet
- ODK DocumentationDocument571 pagesODK DocumentationAyoub FouzaiNo ratings yet
- Aero SemDocument182 pagesAero SemNaveen Singh100% (1)
- Shashi Tharoor SpeechDocument4 pagesShashi Tharoor SpeechShraddha AgarwalNo ratings yet
- 1987 Haapasalo, M., & Ørstavik, D. (1987) - in Vitro Infection and of Dentinal Tubules. Journal of Dental ResearchDocument5 pages1987 Haapasalo, M., & Ørstavik, D. (1987) - in Vitro Infection and of Dentinal Tubules. Journal of Dental ResearchAlexandra Illescas GómezNo ratings yet
- Ishan Report PDFDocument69 pagesIshan Report PDFprathmesh666patilNo ratings yet
- Mci 1Document34 pagesMci 1NAMITHA M RNo ratings yet
- 3Q Science Reaserch PTDocument2 pages3Q Science Reaserch PTFiona Clarisse ManuelNo ratings yet
- Annual Report 2022Document366 pagesAnnual Report 2022Sagar chNo ratings yet
- Review TestDocument8 pagesReview TestнуркызNo ratings yet
- Jama 2022 327 1379Document13 pagesJama 2022 327 1379silviaNo ratings yet
- Module 1 in HRMGTDocument26 pagesModule 1 in HRMGTShela Mae FranciscoNo ratings yet
- Betriebsanleitung General Operating ManualDocument24 pagesBetriebsanleitung General Operating ManualMaria Eugenia RiveraNo ratings yet
- Description: Data Cable, U/UTP, Category 6, AWG23, Euroclass CDocument2 pagesDescription: Data Cable, U/UTP, Category 6, AWG23, Euroclass Cosmanovic2020No ratings yet
- A Study On Customer Satisfaction of MobilesDocument66 pagesA Study On Customer Satisfaction of MobilesNirmal RajNo ratings yet
- Aquos Lc-40d68utDocument31 pagesAquos Lc-40d68utCesar Alfredo TrejoNo ratings yet
- Business Improvement DistrictsDocument27 pagesBusiness Improvement DistrictstaliagcNo ratings yet
- EMS Produkteflyer 05-2016 en WebDocument16 pagesEMS Produkteflyer 05-2016 en Webjerry chanNo ratings yet
- Periodic Properties - HandbookDocument12 pagesPeriodic Properties - HandbookHarsh KulkarniNo ratings yet
- Language Death - WikipediaDocument15 pagesLanguage Death - WikipediaJeremiah OlatunbosunNo ratings yet
- Ac 7000 F Blowing AgentDocument1 pageAc 7000 F Blowing AgentFraz Ahmad100% (1)
- Quality Matters in Recommender SystemsDocument4 pagesQuality Matters in Recommender SystemsCollinsNo ratings yet
- Lecture1 PH113 Module4Document12 pagesLecture1 PH113 Module4dtrhNo ratings yet
- PROJECTDocument50 pagesPROJECTBasil PNo ratings yet
- Elc 030 Movie Review Assignment (Haikal)Document10 pagesElc 030 Movie Review Assignment (Haikal)Wan Amir IslamNo ratings yet
- Material Safety Data Sheet (MSDS) : 1. Product and CompanyDocument6 pagesMaterial Safety Data Sheet (MSDS) : 1. Product and CompanySofy Y. C.No ratings yet
- Scenario: Respiratory DisordersDocument3 pagesScenario: Respiratory DisordersYelrebmik OdranrebNo ratings yet
- Case StudyDocument3 pagesCase StudyAJ BayNo ratings yet
- SFL Joining KitDocument11 pagesSFL Joining Kitdharam singhNo ratings yet
- S 000 LBLDocument14 pagesS 000 LBLfaisal abbasNo ratings yet
- Ayurvedic Herbology: Dravya Guna ShastraDocument8 pagesAyurvedic Herbology: Dravya Guna ShastraMinakshi ki creativesNo ratings yet
- Activity Book TawjihiDocument80 pagesActivity Book TawjihiEyad SobehNo ratings yet
- Third Periodical Test in MAPEH Grade 10Document6 pagesThird Periodical Test in MAPEH Grade 10gabby ilagan100% (1)
- Acute Pancreatitis in DogsDocument4 pagesAcute Pancreatitis in Dogslisa sheridanNo ratings yet
- Discharge PlanDocument4 pagesDischarge PlanMaythresha GonzalesNo ratings yet
- Biological Classification - DPP 10 - Arjuna NEET (2025)Document4 pagesBiological Classification - DPP 10 - Arjuna NEET (2025)adityachandarNo ratings yet
- Intussusception: DR Phillipo Leo ChalyaDocument19 pagesIntussusception: DR Phillipo Leo ChalyaSibabaong'ombe MasakaNo ratings yet
- 11 - Genitourinary Injuries TestDocument3 pages11 - Genitourinary Injuries TestSusi YuliawatiNo ratings yet
- DVT User ManualDocument28 pagesDVT User ManualNourah Hamad AlsultanNo ratings yet
- Neet OrthopedicsDocument426 pagesNeet OrthopedicsBhupi AgrawalNo ratings yet
- 118A - Liver-Failure Handout #5 (Sir Marvin)Document5 pages118A - Liver-Failure Handout #5 (Sir Marvin)Joanna TaylanNo ratings yet
- Gluten Related Disorders Celiac Disease Wheat Allergy and Nonceliac Gluten SensitivityDocument17 pagesGluten Related Disorders Celiac Disease Wheat Allergy and Nonceliac Gluten SensitivityAngélica MuñozNo ratings yet
- Gagal NapasDocument157 pagesGagal NapasFia Delfia AdventyNo ratings yet
- Assisting The Patient During The Lumbar Puncture DefinitionDocument3 pagesAssisting The Patient During The Lumbar Puncture DefinitionSHAINA CADALINNo ratings yet
- Sepsis Syndromes in Adults - Epidemiology, Definitions, Clinical Presentation, Diagnosis, and Prognosis - UpToDateDocument46 pagesSepsis Syndromes in Adults - Epidemiology, Definitions, Clinical Presentation, Diagnosis, and Prognosis - UpToDateparou haNo ratings yet
- Deb Shapiro: Messages That Underlie LlinessaDocument372 pagesDeb Shapiro: Messages That Underlie Llinessacharlesburlan100% (1)
- CHN QUIZ COMPIL - MergedDocument8 pagesCHN QUIZ COMPIL - Merged2080315No ratings yet
- Echo Embark Ofa ReportDocument3 pagesEcho Embark Ofa Reportapi-283492496No ratings yet
- Literature Review Breast Self Examination ResearchDocument7 pagesLiterature Review Breast Self Examination ResearchaflsigakfNo ratings yet
- B. Gastroesophageal Reflux Disorder (GERD)Document15 pagesB. Gastroesophageal Reflux Disorder (GERD)Charisma MeromiNo ratings yet
- Oral Revalida Round 2Document63 pagesOral Revalida Round 2Mercy Anne EcatNo ratings yet
- RSLT An21100870 PDFDocument3 pagesRSLT An21100870 PDFMuhammed Ameen MoulaviNo ratings yet
- Instant Ebooks Textbook Evidence-Based Physical Examination Handbook 1st Edition Kate Gawlik Download All ChaptersDocument62 pagesInstant Ebooks Textbook Evidence-Based Physical Examination Handbook 1st Edition Kate Gawlik Download All Chaptersmodexxjhosue100% (6)
- Cardio Tonic DrugDocument25 pagesCardio Tonic DrugNistha MudgilNo ratings yet
- Cardiac AssessmentDocument54 pagesCardiac AssessmentAthira PSNo ratings yet
- PATHOPHYSIOLOGY (Schematic Diagram) : - Fever - LeukocytosisDocument3 pagesPATHOPHYSIOLOGY (Schematic Diagram) : - Fever - Leukocytosisranee diane100% (1)
- Biology Project On Effect of Antibiotics On MicroorganismsDocument13 pagesBiology Project On Effect of Antibiotics On Microorganismsitznush15No ratings yet