NANDA Nursing Diagnosis: Ineffective Breathing Pattern Related To As Evidenced by NANDA Definition
NANDA Nursing Diagnosis: Ineffective Breathing Pattern Related To As Evidenced by NANDA Definition
Download as docx, pdf, or txt
You might also like
- Clinical Case Scenario 6Document17 pagesClinical Case Scenario 6Sean Menard Flores100% (1)
- Answers Lab10 RespPhysiologyDocument6 pagesAnswers Lab10 RespPhysiologyRafael Castillo100% (1)
- NCP (Icu)Document2 pagesNCP (Icu)jessie_nuñez_267% (9)
- The Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1From EverandThe Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1Rating: 5 out of 5 stars5/5 (2)
- Respiratory Therapy Pocket Reference: Ifnopt TriggerDocument2 pagesRespiratory Therapy Pocket Reference: Ifnopt TriggermohamedkorieshNo ratings yet
- Ineffective Breathing Pattern As Evidenced by Use of Accessory Muscles and Episodes of DyspneaDocument3 pagesIneffective Breathing Pattern As Evidenced by Use of Accessory Muscles and Episodes of DyspneaNiel MinatozakiNo ratings yet
- Nursing Diagnosis Nursing Intervention Rationale Breathing PatternDocument8 pagesNursing Diagnosis Nursing Intervention Rationale Breathing PatternJinaan MahmudNo ratings yet
- Nursing Diagnosis Nursing Intervention Rationale Breathing PatternDocument7 pagesNursing Diagnosis Nursing Intervention Rationale Breathing PatternJinaan MahmudNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaNo ratings yet
- NCP2tikikoDocument4 pagesNCP2tikikoanthonyocenararmaNo ratings yet
- Assesment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssesment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- Go NCP IneffectivebreathingpatDocument7 pagesGo NCP IneffectivebreathingpatSAMANTHA T. MODESTONo ratings yet
- Independent:: Melanie Claire Torillo Bsn2 LeiningerDocument12 pagesIndependent:: Melanie Claire Torillo Bsn2 LeiningermelanieclairetorilloNo ratings yet
- NCP - Explanation or ScriptDocument8 pagesNCP - Explanation or ScriptLee Rondeck Angelov CastilloNo ratings yet
- UntitledDocument5 pagesUntitledJayelles Dixien JuguilonNo ratings yet
- Viray, Messiah Jezreel: NCP #3 For RHDDocument3 pagesViray, Messiah Jezreel: NCP #3 For RHDJezzy VeeNo ratings yet
- Assessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentDocument7 pagesAssessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentQueenie Silva100% (1)
- NCP Ineffective Breathing PatternDocument4 pagesNCP Ineffective Breathing PatternSeika SouiNo ratings yet
- Plan of CareDocument27 pagesPlan of CareAnonymous 7i9XIgNo ratings yet
- NCP and Drug SheetDocument16 pagesNCP and Drug SheetLucil Jaine Abayan BellezaNo ratings yet
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternPaolo Anthony GonzalesNo ratings yet
- Actaul Drug StudyDocument2 pagesActaul Drug Studyjasper pachingelNo ratings yet
- Case Pres Ncps FinalDocument13 pagesCase Pres Ncps FinalMariejoy YadaoNo ratings yet
- Ineffective Breathing Pattern Related To HyperventilationDocument4 pagesIneffective Breathing Pattern Related To HyperventilationVanessa Charlotte LagunayNo ratings yet
- M. Top Three Nursing Care PlanDocument3 pagesM. Top Three Nursing Care PlanAraw GabiNo ratings yet
- NCP MiniparDocument9 pagesNCP MiniparKyla Avila TorrevillasNo ratings yet
- NCP Ineffective Airway ClearanceDocument8 pagesNCP Ineffective Airway Clearance1adie1907No ratings yet
- NCP For CAP TB.Document5 pagesNCP For CAP TB.Cherry Ann BalagotNo ratings yet
- NCP Hyperthyroidism-Rotation 3-Med WardDocument8 pagesNCP Hyperthyroidism-Rotation 3-Med WardChristine Joy MolinaNo ratings yet
- NCP Lung CancerDocument2 pagesNCP Lung CancerLezel LaracasNo ratings yet
- NCP For LEC Act. 5Document1 pageNCP For LEC Act. 5Keneth Dave AglibutNo ratings yet
- Pulmo Nursing Care PlanDocument3 pagesPulmo Nursing Care PlanVincent RoyNo ratings yet
- Lumunok at Huminga, Nabibilaukan Din Ako Madalas" AsDocument4 pagesLumunok at Huminga, Nabibilaukan Din Ako Madalas" AsPatricia Ortega100% (1)
- NCP-2Document3 pagesNCP-2Trixie Shane TamboboyNo ratings yet
- "I Don't Have An Infection in My Gallbladder Which Is Good, But I Do Feel The Pain," As Verbalized by TheDocument2 pages"I Don't Have An Infection in My Gallbladder Which Is Good, But I Do Feel The Pain," As Verbalized by Theunnamed person100% (1)
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternNicole Genevie MallariNo ratings yet
- Nursing Care PlanDocument18 pagesNursing Care PlanLayo, Ivy L.No ratings yet
- Assessment Explanatio Nofthe Problem Objectives Nursing Intervention Rationale EvaluationDocument3 pagesAssessment Explanatio Nofthe Problem Objectives Nursing Intervention Rationale EvaluationAziil LiizaNo ratings yet
- Final Thyroid Storm NCPDocument6 pagesFinal Thyroid Storm NCPoguitekim1No ratings yet
- Nursing Care Plan: Cystic FibrosisDocument4 pagesNursing Care Plan: Cystic FibrosisYael EzraNo ratings yet
- Nursing Care Plan: Lopez, Maria Sofia B. 9/29/2020 3-BSN-B Prof. ZoletaDocument5 pagesNursing Care Plan: Lopez, Maria Sofia B. 9/29/2020 3-BSN-B Prof. ZoletaSofiaLopezNo ratings yet
- LDH NCP3Document2 pagesLDH NCP3Rheal P EsmailNo ratings yet
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Objectives Interventions Rationale EvaluationBianca Mikaela DosdosNo ratings yet
- Acute PainDocument2 pagesAcute PainNicole Genevie MallariNo ratings yet
- Myrna CruzDocument3 pagesMyrna CruzChris Opal NamocatcatNo ratings yet
- NCP Room 303 TelarmaDocument2 pagesNCP Room 303 TelarmaasdasdNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- Asthma Nursing Care Plan NCP Ineffective Airway Clearance CompressDocument2 pagesAsthma Nursing Care Plan NCP Ineffective Airway Clearance CompressMargarette GeresNo ratings yet
- NCP - Ineffective Breathing PatternDocument3 pagesNCP - Ineffective Breathing PatternJose Marlon CandelariaNo ratings yet
- Cap Nursing Care PlanDocument6 pagesCap Nursing Care PlanCharlene Grace ReginoNo ratings yet
- ASSESSMENT NCPDocument4 pagesASSESSMENT NCPjana manaloNo ratings yet
- DULNUANDocument2 pagesDULNUANJB tindonganNo ratings yet
- Case-Scenario Respiratoty Disease During Pregnancy NCPDocument4 pagesCase-Scenario Respiratoty Disease During Pregnancy NCPChristianne CapuaNo ratings yet
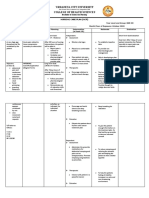
- 'Urdaneta City University College of Health Sciences: Bachelor of Science in NursingDocument4 pages'Urdaneta City University College of Health Sciences: Bachelor of Science in NursingDan Dan ManaoisNo ratings yet
- Programme: High Diploma in NursingDocument7 pagesProgramme: High Diploma in NursingYeesze ChanNo ratings yet
- Romero, Deinielle Ingrid M. (Hiv)Document8 pagesRomero, Deinielle Ingrid M. (Hiv)Deinielle Magdangal RomeroNo ratings yet
- NCP Copd FinalDocument3 pagesNCP Copd FinalGiselle EstoquiaNo ratings yet
- ASSESSMENTDocument6 pagesASSESSMENTZerimar Adawe DulnuanNo ratings yet
- Date Assessment Cues Need Nursing Diagnosis Background Knowledge Objectives Nursing Actions EvaluationDocument3 pagesDate Assessment Cues Need Nursing Diagnosis Background Knowledge Objectives Nursing Actions EvaluationJoyce Minerva Montero SamsonNo ratings yet
- Nursing Care Plan #1Document6 pagesNursing Care Plan #1Yamete KudasaiNo ratings yet
- Assessment: Nursing Care PlanDocument3 pagesAssessment: Nursing Care PlanDana LabusonNo ratings yet
- Ineffective Breathing PatternDocument4 pagesIneffective Breathing PatternJulmae AlcoverNo ratings yet
- Drug Study For WorkbookDocument7 pagesDrug Study For WorkbookTrisha VergaraNo ratings yet
- Pulmonary Embolism: PathophysiologyDocument1 pagePulmonary Embolism: PathophysiologyTrisha VergaraNo ratings yet
- Client's Chart: PathophysiologyDocument1 pageClient's Chart: PathophysiologyTrisha VergaraNo ratings yet
- CardiomyopathyDocument1 pageCardiomyopathyTrisha VergaraNo ratings yet
- Pulmonary Function TestsDocument57 pagesPulmonary Function Testsmerin sunilNo ratings yet
- Skill: Assessing The Thorax and LungsDocument3 pagesSkill: Assessing The Thorax and LungsKathrina AlfonsoNo ratings yet
- Nursing Care Plan Children With Asthma: by HaryatiningsihpurwandariDocument19 pagesNursing Care Plan Children With Asthma: by HaryatiningsihpurwandariARUM APRIANI 1No ratings yet
- Bronchiolitis Seminar.Document15 pagesBronchiolitis Seminar.Sudha YadavNo ratings yet
- Discharge Plan - Dinson, Red Angela O. BSN 1-BDocument2 pagesDischarge Plan - Dinson, Red Angela O. BSN 1-BRed Angela DinsonNo ratings yet
- English Question Paper 2010Document6 pagesEnglish Question Paper 2010priyankaNo ratings yet
- MG I Tema 6 - Limba EnglezaDocument2 pagesMG I Tema 6 - Limba EnglezaAlisa StefaniaNo ratings yet
- ASTHMA AND COPD PharmacologyDocument42 pagesASTHMA AND COPD Pharmacologycarla osbourneNo ratings yet
- Health and Safety in Cement Industry: June 2022Document7 pagesHealth and Safety in Cement Industry: June 2022shibanand.pandaNo ratings yet
- Schatz 2014Document4 pagesSchatz 2014zavoianu.diana21No ratings yet
- Hydrocortisone Ointment-Drug StudyDocument1 pageHydrocortisone Ointment-Drug StudyTrisha CayabyabNo ratings yet
- The Respiratory Muscles: How Is The "Ventilatory Pump" Made?Document2 pagesThe Respiratory Muscles: How Is The "Ventilatory Pump" Made?Badrul AhsanNo ratings yet
- Grade 9 Respiratory SystemDocument22 pagesGrade 9 Respiratory SystemMelanie Tagudin TrinidadNo ratings yet
- Assessment Diagnosis Planning Intervention EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention EvaluationCharissa Magistrado De LeonNo ratings yet
- Course Unit 4 Respiratory Assessment Techniques and Monitoring System. Acdemesa. 2023Document66 pagesCourse Unit 4 Respiratory Assessment Techniques and Monitoring System. Acdemesa. 2023Bianca BautistaNo ratings yet
- Administering Oxygen by Nasal CannulaDocument5 pagesAdministering Oxygen by Nasal CannulaAndrea Bayaga WaganNo ratings yet
- Soal Latihan Kls 9 SMT 1-Part 2Document6 pagesSoal Latihan Kls 9 SMT 1-Part 2Primaplus SamarindaNo ratings yet
- Pharmacology - Respiratory SystemDocument9 pagesPharmacology - Respiratory Systemwedikaf807No ratings yet
- Bronchial Asthma!: A C E S G V CDocument10 pagesBronchial Asthma!: A C E S G V CAmalNo ratings yet
- Welding Fume Control: Control Approach 1 Control Approach 2Document9 pagesWelding Fume Control: Control Approach 1 Control Approach 2garden00589No ratings yet
- HSE Free Ceramics COSHH For ManagersDocument3 pagesHSE Free Ceramics COSHH For ManagersTony RobertsNo ratings yet
- BCCH PRAM Score For Assessment For AsthmaDocument3 pagesBCCH PRAM Score For Assessment For Asthmadini kusmaharaniNo ratings yet
- SBI241 - Week 7 Kahoot's QuizDocument4 pagesSBI241 - Week 7 Kahoot's Quizjessicalrogers01No ratings yet
- I. Concept Mapping: Legend: (Color/shape)Document3 pagesI. Concept Mapping: Legend: (Color/shape)taehyungieeNo ratings yet
- RTM 3Document8 pagesRTM 3Christine Danica BiteraNo ratings yet
- Journal Reading: Asma: Raden Muhamad HidayatDocument28 pagesJournal Reading: Asma: Raden Muhamad HidayatRaden Muhammad HidayatNo ratings yet
- Seminar Topic 3Document32 pagesSeminar Topic 3Guenevere DamasinNo ratings yet
- Cap. 21. MEDICAL Emergeencies in Dental PracticeDocument10 pagesCap. 21. MEDICAL Emergeencies in Dental PracticeVlad LichiNo ratings yet