Treatment of Impacted Canines With Aligners: An Alternative and Viable Option
Treatment of Impacted Canines With Aligners: An Alternative and Viable Option
Download as pdf or txt
You might also like
- Clinical Outcomes of Vertical Bone Augmentation To Enable Dental Implant Placement: A Systematic ReviewDocument13 pagesClinical Outcomes of Vertical Bone Augmentation To Enable Dental Implant Placement: A Systematic Reviewvanessa_werbickyNo ratings yet
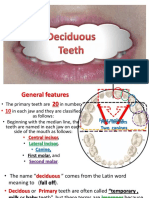
- Development of Occlusion 1 PDFDocument5 pagesDevelopment of Occlusion 1 PDFFadiShihabNo ratings yet
- Preformed Intrusion Bulbs On Clear Aligners Facilitate Active Vertical Control in A Hyperdivergent Skeletal Class II Case With Extraction - A Case Report With 4-Year Follow-UpDocument9 pagesPreformed Intrusion Bulbs On Clear Aligners Facilitate Active Vertical Control in A Hyperdivergent Skeletal Class II Case With Extraction - A Case Report With 4-Year Follow-UpThang Nguyen TienNo ratings yet
- Gallucci 1Document12 pagesGallucci 1Od GermanAgueroNo ratings yet
- Tanpa Judul PDFDocument7 pagesTanpa Judul PDFnadyashintakasihNo ratings yet
- Angle Orthod. 2019 89 6 839-46 PDFDocument8 pagesAngle Orthod. 2019 89 6 839-46 PDFbrookortontiaNo ratings yet
- Treatment of An Anterior Open Bite, Bimaxillary Protrusion and Mesiocclusion by The Extraction of Premolars and The Use of Clear AlignersDocument14 pagesTreatment of An Anterior Open Bite, Bimaxillary Protrusion and Mesiocclusion by The Extraction of Premolars and The Use of Clear AlignersAstrid HutabaratNo ratings yet
- Evaluación de La Precisión de Los Movimientos Ortodóncicos Con Alineadores Un Estudio Observacional ProspectivoDocument8 pagesEvaluación de La Precisión de Los Movimientos Ortodóncicos Con Alineadores Un Estudio Observacional ProspectivorocioNo ratings yet
- Agliardi - Immediate Fixed Rehabilitation ofDocument11 pagesAgliardi - Immediate Fixed Rehabilitation ofAnsaquilo AnsaquiloNo ratings yet
- qt2059w9zd NosplashDocument8 pagesqt2059w9zd NosplashCrișu LauraNo ratings yet
- Ajodo 3Document10 pagesAjodo 3ayisNo ratings yet
- Anchorage Control in Bioprogressive Vs Straight-Wire Treatment PDFDocument6 pagesAnchorage Control in Bioprogressive Vs Straight-Wire Treatment PDFsolodont1No ratings yet
- Conservative Endodontic Microsurgery To Protect Critical Anatomical Structures - Selective Curettage: A Case SeriesDocument12 pagesConservative Endodontic Microsurgery To Protect Critical Anatomical Structures - Selective Curettage: A Case SeriesClaudia Pérez LuisNo ratings yet
- Francetti, 2008 - All On Four Na Mandibula Com Implantes Distais Inclinados Tem Excelentes Resultados Clinicos. Bom ArtigoDocument9 pagesFrancetti, 2008 - All On Four Na Mandibula Com Implantes Distais Inclinados Tem Excelentes Resultados Clinicos. Bom Artigowender.bs10No ratings yet
- Cleft Maxillary Distraction Versus Orthognathic Surgery: Clinical Morbidities and Surgical RelapseDocument13 pagesCleft Maxillary Distraction Versus Orthognathic Surgery: Clinical Morbidities and Surgical RelapseRohan BhagatNo ratings yet
- Free Flaps MaxillaDocument7 pagesFree Flaps MaxillaFahad QiamNo ratings yet
- 11 B - All On Four Group 01 PDFDocument3 pages11 B - All On Four Group 01 PDFLuis Humberto BorgesNo ratings yet
- Outcome of Single Immediate Implants Placed inDocument8 pagesOutcome of Single Immediate Implants Placed injuanita enriquezNo ratings yet
- Endodontic Treatment of A Large Periradicular Lesion: A Case ReportDocument4 pagesEndodontic Treatment of A Large Periradicular Lesion: A Case ReportSholehudin Al AyubiNo ratings yet
- Endodontic Treatment of A Large Periradicular Lesion: A Case ReportDocument4 pagesEndodontic Treatment of A Large Periradicular Lesion: A Case ReportSholehudin Al AyubiNo ratings yet
- Combined Orthodontic and Surgical Open Bite Correction: Principles For Success. Part 2Document15 pagesCombined Orthodontic and Surgical Open Bite Correction: Principles For Success. Part 2mlnunezNo ratings yet
- Drughelp - Care 6.22Document10 pagesDrughelp - Care 6.22Joko RifaiNo ratings yet
- FDP AvulsionDocument8 pagesFDP AvulsionNico BrantesNo ratings yet
- Surgery First in Bimaxillary Orthognathic SurgeryDocument8 pagesSurgery First in Bimaxillary Orthognathic SurgerySantiago SamacaNo ratings yet
- Twin Occlusion Prosthesis: An Alternative To Conventional Guide Ramp - A Case ReportDocument5 pagesTwin Occlusion Prosthesis: An Alternative To Conventional Guide Ramp - A Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Provisional RestorationsDocument4 pagesProvisional RestorationsMyri Gebert SchererNo ratings yet
- 2022 AiutoDocument7 pages2022 AiutovivianaNo ratings yet
- Francetti, 2010 - Implantes Inclinados Tem Boa Perfomance e Semelhante Aos Implantes Ratos em All On Four em Mandibula e MaxilaDocument9 pagesFrancetti, 2010 - Implantes Inclinados Tem Boa Perfomance e Semelhante Aos Implantes Ratos em All On Four em Mandibula e Maxilawender.bs10No ratings yet
- Cleft PalateDocument4 pagesCleft PalateShoaib A. KaziNo ratings yet
- Case Report: Management of Six Root Canals in Mandibular First MolarDocument6 pagesCase Report: Management of Six Root Canals in Mandibular First MolarArida Khoiruza Asy'ariNo ratings yet
- Lopes Et Al 2021Document14 pagesLopes Et Al 2021kaka**No ratings yet
- Zygomatic Implants Placed in Immediate FDocument14 pagesZygomatic Implants Placed in Immediate FJeTT BLaCKNo ratings yet
- A Case Report of Prosthodontics Treatment of Maxillary DefectDocument4 pagesA Case Report of Prosthodontics Treatment of Maxillary DefectAyu DamayantiNo ratings yet
- Mermigos 11 01Document4 pagesMermigos 11 01Sankurnia HariwijayadiNo ratings yet
- ALL On 4 Investigación MulticéntricoDocument6 pagesALL On 4 Investigación MulticéntricoOCTAEN POQUINo ratings yet
- 1 s2.0 S2210261221004363 MainDocument7 pages1 s2.0 S2210261221004363 MainFlávia de Souza BastosNo ratings yet
- 1 s2.0 S0020653923004392 MainDocument7 pages1 s2.0 S0020653923004392 MainWillmann Antonio Jiménez MoralesNo ratings yet
- Thesis Copy 6 CorrectedDocument54 pagesThesis Copy 6 CorrectedanushiNo ratings yet
- Zona Neutra Maxilofacial PacienteDocument6 pagesZona Neutra Maxilofacial Pacientemargarita de montenegroNo ratings yet
- ARTICULO3Document10 pagesARTICULO3enriquecollahuafloresNo ratings yet
- Treating Patella Fractures With A Fixed-Angle Patella PlateDocument7 pagesTreating Patella Fractures With A Fixed-Angle Patella PlateAldrovando JrNo ratings yet
- Ojsadmin, 388Document10 pagesOjsadmin, 388Srishti Jain MalooNo ratings yet
- Three-Dimensional Assessment of Mandibular and Glenoid Fossa Changes After Bone-Anchored Class III Intermaxillary TractionDocument7 pagesThree-Dimensional Assessment of Mandibular and Glenoid Fossa Changes After Bone-Anchored Class III Intermaxillary TractionRam RamNo ratings yet
- Case Report and Literature Review: Autonomous Robotic System Assisted Palatal Implantation at An Anterior Teeth Site Compromised by Periapical CystDocument7 pagesCase Report and Literature Review: Autonomous Robotic System Assisted Palatal Implantation at An Anterior Teeth Site Compromised by Periapical Cystyakebot0930No ratings yet
- MapaDocument9 pagesMapaRicha AhlawatNo ratings yet
- Sammartino 2007Document12 pagesSammartino 2007Roy Anthony Rivera RamirezNo ratings yet
- Teoria de Las 4 Columnas Pilon TibialDocument11 pagesTeoria de Las 4 Columnas Pilon TibialOscar Cayetano Herrera RodríguezNo ratings yet
- Evidence-Based Concepts and Procedures For Bonded Inlays and Onlays. Part III. A Case Series With Long-Term Clinical Results and Follow-UpDocument17 pagesEvidence-Based Concepts and Procedures For Bonded Inlays and Onlays. Part III. A Case Series With Long-Term Clinical Results and Follow-UpCamilo SestoNo ratings yet
- A Rare Case of Periapical Healing in An Apically Extruding, Separated InstrumentDocument3 pagesA Rare Case of Periapical Healing in An Apically Extruding, Separated InstrumentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Secretos de La Mordida ProfundaDocument11 pagesSecretos de La Mordida Profundaaldair villazoNo ratings yet
- Weinstein 2010Document8 pagesWeinstein 2010gbaez.88No ratings yet
- IPIntJMedPaediatrOncol 9 2 77 82Document6 pagesIPIntJMedPaediatrOncol 9 2 77 82Laraduta AgustiniNo ratings yet
- Case SeriesDocument5 pagesCase SeriesPavithra balasubramaniNo ratings yet
- Carlino 2019Document9 pagesCarlino 2019Isabella WilkeNo ratings yet
- Salmen 2017Document7 pagesSalmen 2017Lorena PaulaNo ratings yet
- Significance of Saddle Angle in Myofunctional TherDocument11 pagesSignificance of Saddle Angle in Myofunctional TherGhazalaNo ratings yet
- 1 s2.0 S2772906024003558 MainDocument4 pages1 s2.0 S2772906024003558 MainWinda KhosasiNo ratings yet
- Influence of The Fixed Implant-Supported Provisional Phase On The Esthetic Final Outcome of Implant-Supported Crowns. David Furze. 2019. Wiley PeriodicalsDocument7 pagesInfluence of The Fixed Implant-Supported Provisional Phase On The Esthetic Final Outcome of Implant-Supported Crowns. David Furze. 2019. Wiley PeriodicalsValeria CrespoNo ratings yet
- Space Closure by Miniscrew-Assisted Mesialization of An Upper Third Molar and Partial Vestibular Fixed Appliance: A Case ReportDocument15 pagesSpace Closure by Miniscrew-Assisted Mesialization of An Upper Third Molar and Partial Vestibular Fixed Appliance: A Case ReportCarol Gissel FloresNo ratings yet
- Full-Mouth Rehabilitation With Implant-Supported Fixed ProsthesisDocument8 pagesFull-Mouth Rehabilitation With Implant-Supported Fixed ProsthesisRamesh GuptaNo ratings yet
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- Treatment of Maxillary Canine TranspositionDocument8 pagesTreatment of Maxillary Canine TranspositionFabian BarretoNo ratings yet
- Stability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesDocument8 pagesStability of Class II Malocclusion Treatment With The Distal Jet Followed by Fixed AppliancesFabian BarretoNo ratings yet
- Surgical-Orthodontic Treatment of Class I Malocclusion With Maxillary Vertical Excess - A Case ReportDocument7 pagesSurgical-Orthodontic Treatment of Class I Malocclusion With Maxillary Vertical Excess - A Case ReportFabian BarretoNo ratings yet
- Destefani 2020Document8 pagesDestefani 2020Fabian BarretoNo ratings yet
- Biomechanical Basis of Vertical Dimension Control During Rapid Palatal Expansion TherapyDocument7 pagesBiomechanical Basis of Vertical Dimension Control During Rapid Palatal Expansion TherapyFabian BarretoNo ratings yet
- Maxillary Canine-First Premolar TranspositionDocument9 pagesMaxillary Canine-First Premolar TranspositionFabian BarretoNo ratings yet
- Treatment of Class III Malocclusion: The Key Role of The Occlusal PlaneDocument9 pagesTreatment of Class III Malocclusion: The Key Role of The Occlusal PlaneFabian BarretoNo ratings yet
- Frankel 4Document13 pagesFrankel 4Fabian BarretoNo ratings yet
- Clase II División 2 (4645)Document6 pagesClase II División 2 (4645)Fabian BarretoNo ratings yet
- Dentición Normal (4646)Document6 pagesDentición Normal (4646)Fabian BarretoNo ratings yet
- Accuracy of Measurements of Mandibular Anatomy andDocument7 pagesAccuracy of Measurements of Mandibular Anatomy andFabian BarretoNo ratings yet
- Fluoride Varnish For The Prevention of White Spot Lesions During Orthodontic Treatment With Fixed Appliances: A Randomized Controlled TrialDocument5 pagesFluoride Varnish For The Prevention of White Spot Lesions During Orthodontic Treatment With Fixed Appliances: A Randomized Controlled TrialFabian BarretoNo ratings yet
- Methods of Space GainingDocument95 pagesMethods of Space GainingVincent Ser100% (4)
- 5 Upper CanineDocument26 pages5 Upper Caninemoh.ahm3040No ratings yet
- Dental Anatomy - QuizDocument5 pagesDental Anatomy - Quizmu7me7100% (2)
- Stability of Extraction Space Closure: Original ArticleDocument7 pagesStability of Extraction Space Closure: Original ArticleSoe San KyawNo ratings yet
- Anatomy of Permanent TeethDocument76 pagesAnatomy of Permanent TeethSinchita MahataNo ratings yet
- Oral Anatomy Q&ADocument8 pagesOral Anatomy Q&AHanny CarinoNo ratings yet
- Deep Overbite Correction by IntrusionDocument22 pagesDeep Overbite Correction by IntrusionGuillermo Alvarado LassoNo ratings yet
- NomenclatureDocument12 pagesNomenclatureImran KhanNo ratings yet
- Cephalometric SentDocument17 pagesCephalometric SentMuhammad NiyalishNo ratings yet
- Seminar Space MaintainersDocument84 pagesSeminar Space MaintainersStranger DNo ratings yet
- Ceramic Laminate Veneers: Clinical Procedures With A Multidisciplinary ApproachDocument24 pagesCeramic Laminate Veneers: Clinical Procedures With A Multidisciplinary ApproachDaniel AtiehNo ratings yet
- Pearson Vue 1Document12 pagesPearson Vue 1panimalar madhaNo ratings yet
- 2 Deciduous TeethDocument36 pages2 Deciduous TeethAbdelrahman GalalNo ratings yet
- عبد الرحمن خالد الزميلي Assighment Of Dental Surgery /Principle of routine exodontiaDocument20 pagesعبد الرحمن خالد الزميلي Assighment Of Dental Surgery /Principle of routine exodontiaعبد الرحمن خالد الزميليNo ratings yet
- Myofunctional Appliances Part 2Document156 pagesMyofunctional Appliances Part 2AnahitaNo ratings yet
- Epi IDocument4 pagesEpi IAna-Maria MachidonNo ratings yet
- JDAT2023-11 Manuscript @14.9.66Document17 pagesJDAT2023-11 Manuscript @14.9.66aggasit manoNo ratings yet
- Intra-Oral Radiographic TechniquesDocument163 pagesIntra-Oral Radiographic TechniquesdrdeepsomrNo ratings yet
- 2 2 PreMolars Q.Document10 pages2 2 PreMolars Q.Ola Ali100% (1)
- 2016, Biofunctional ProstheticDocument6 pages2016, Biofunctional ProstheticlupitaNo ratings yet
- AbutmentDocument40 pagesAbutmentManal R. HassanNo ratings yet
- مرشد القارئ (ارب اوّل)Document5 pagesمرشد القارئ (ارب اوّل)syedismail40455No ratings yet
- 5.etiology of MalocclusionDocument20 pages5.etiology of MalocclusionAhmed Hegazy100% (2)
- Analysis of Dental Homologies and Phylogeny of Paucituberculata (Mammalia: Marsupialia)Document25 pagesAnalysis of Dental Homologies and Phylogeny of Paucituberculata (Mammalia: Marsupialia)mioclaenusNo ratings yet
- Functional Occlusion and Orthodontics: A Contemporary ApproachDocument9 pagesFunctional Occlusion and Orthodontics: A Contemporary Approachdrgayen6042No ratings yet
- Presented Before The Annual Meeting of The American Association of Orthodontists, Dal-Las, Texas, April, 1953Document13 pagesPresented Before The Annual Meeting of The American Association of Orthodontists, Dal-Las, Texas, April, 1953Paola LoloNo ratings yet
- TuversonDocument19 pagesTuversonFabio RibeiroNo ratings yet
- Damon SystemDocument121 pagesDamon SystemPraveen Raghav80% (5)
- Evaluation of Moyer's Mixed Dentition Space Analysis in Indian ChildrenDocument6 pagesEvaluation of Moyer's Mixed Dentition Space Analysis in Indian ChildrenfadillaNo ratings yet